Article Text

Abstract
Background: Trichomonas vaginalis, which affects at least 170 million individuals globally, may increase the risk of transmission of HIV and predispose pregnant women to premature rupture of membranes and early labour.
Objective: To more clearly define the epidemiology of trichomoniasis and to develop a mathematical model of disease transmission dynamics in order to explore various treatment strategies.
Design: A deterministic model of trichomoniasis was constructed. Parameter values were set to fit the model to known endemic prevalence levels of Trichomonas vaginalis. Two treatment interventions (“screening” and “syndromic management”) were simulated.
Results: The age specific prevalence of the disease was seen to differ from other STDs in a number of studies. Parameter fitting indicates that the average duration of infection in women is at least 3–5 years and approximately 4 months for men. “Syndromic management” (that is, treating only those with symptoms of disease) had minimal effect upon the endemic prevalence of disease even at high levels of coverage. “Screening” (that is, identification of individuals with both symptomatic and asymptomatic infection) was shown to be the most efficient method of control, but was sensitive to the screening interval.
Conclusions: The control of trichomoniasis seems to have been a success in developed countries because of the regular access to health care, whereas it has remained endemic in many developing countries where control may only be possible by regular screening and treatment. However, without a large investment in services, success in controlling trichomoniasis is likely to be transitory.
- HIV
- trichomoniasis
- Trichomonas vaginalis
- mathematical modelling
- screening
- syndromic management
Statistics from Altmetric.com
Introduction
Trichomonas vaginalis is one of the commonest sexually transmitted pathogens in the world, with an estimated 170 million cases occurring each year.1 The epidemiology of the disease is still poorly understood and some practitioners continue to question its importance. However, there is growing evidence that T vaginalis is an important pathogen, both in its own right due to the “immediate” morbidity associated with infection,2 for its role in the promotion of premature rupture of membranes, premature labour, and low birth weight,3, 4 and because of the likely facilitation of HIV transmission.5–7 While a slightly increased risk for HIV transmission may have minor significance for an individual, it may be of considerable importance at a community level.8 Understanding the relation between T vaginalis and other sexually transmitted infections would assist its use as a marker for the success of behavioural and treatment interventions targeting other STDs including HIV.
In this paper we review the transmission dynamics of T vaginalis infection in the context of a mathematical model of the infection. Parameters needed for the development of this model were estimated from a review of the relevant, largely historical, literature. The review illustrates the difficulties found in describing the epidemiology of a treatable, frequently asymptomatic infection, which probably contributes to the scant attention devoted to this organism. We present some of the insights gained from analysis of this model, which have implications for the design of public health programmes for the control of STDs, with particular relevance to developing countries.
Prevalence studies
The prevalence of T vaginalis varies markedly according to the setting (table 1).4, 9–37 The estimates presented in the table are subject to important biases: the diagnostic methods employed are not consistent and, with only three exceptions,14, 37, 38 the data are drawn from clinic based surveys. Although there is anecdotal evidence that T vaginalis prevalence is low in women in higher socioeconomic groups, the published studies show that the prevalence may be as high as 50% in women in the developing world and in minority groups in industrialised populations. Similarly, the prevalence in men in developed countries appears to be low but there are only limited data in men in developing populations. A study in Papua New Guinea showed that the male indigenous population had a prevalence of 10.9% compared with a prevalence of 0% in the male white population.16 Only four studies have determined the age specific prevalence of T vaginalis infection.14, 16, 38, 39 In each the prevalence was shown to increase monotonically with age among women, a feature not seen in short duration, bacterial STDs, representing a fundamental difference in the epidemiology of this pathogen.
Estimates of the prevalence of T vaginalis infection and proportion with symptoms
Description of the model
We adopted a deterministic model which was originally developed for Neisseria gonorrhoeae infection.40, 41 This model simplifies the natural history of T vaginalis infection by dividing the population at risk into three disease states (i) those susceptible to T vaginalis infection (X); (ii) those with symptomatic infection (Y), and (iii) those with asymptomatic infection (A). The flow from one disease state to another is determined by a set of defined parameters. The population is divided into four sexual activity classes, defined according to the rates of sexual partner change of each group.42 Although infection with T vaginalis induces humoral, cellular, and secretory immune responses there is no evidence for the development of long term immunity. We therefore assume that there is no immune class and that individuals return to the susceptible population following recovery from infection.
A description of the differential equations that define this model are available on request.
EPIDEMIOLOGICAL PARAMETER ESTIMATION
The major infection specific parameters are the duration of infection and its transmissibility. Although there are no recent community based studies that adequately describe the epidemiology of T vaginalis infection, there were a number of surveys and experiments undertaken before the beginning of effective therapy which provide insights into the natural history of the disease. This information can assist in the estimation of parameters and state variables to be used in the modelling described below.
Transmission probability
There is some empirical evidence that permits rough insights about the transmission probability of T vaginalis (table 2).
Percentage of individuals infected by partners with known T vaginalis infection
Male to female:
Catteral43, 44 showed that between 85% and 100% of the female partners of a series of 120 men identified with T vaginalis in two hospital clinics were also positive for T vaginalis. Additionally, Whittington45 found that 10/15 (66%) of the female contacts of male patients with T vaginalis were infected.
Female to male:
Studies have shown the number of infected male partners of infected women ranges from 4–80%. Lancely and McEntegart46 quote a study by Karnacky undertaken in 1938 in which 38/150 (25.3%) of the husbands of women with T vaginalis were found to be infected, but figures of 41.9%, 60%, and 80% were found when more careful investigation was undertaken.14, 47, 48
The interpretation of such contact tracing data is fraught with difficulties. A first problem is to identify the source and direction of infection. If a man is infected but his female partner is not, then presumably the man acquired infection first from someone else and failed to subsequently infect the traced partner. However, if both are infected, did the man infect the woman or vice versa? Or least likely, did both acquire infection from separate sources? From contact tracing data in the absence of excluding transmission in one direction we may be able to infer the upper but not the lower bounds for the transmission probabilities.
Upper bounds:
It is reasonable to assume that all T vaginalis infected individuals are infectious. If infection in women is indefinite (as appears to be the case), and assuming that the methods of diagnosis are sensitive, then the proportion of men's contacts that are infected is an upper bound of the transmission probability from men to women. The calculation of the transmission probability from women to men is more difficult since within a partnership a man can become infected, recover, and be reinfected. The proportion of male sex partners infected at a given time will be a function of the frequency of sex within the partnership, the transmission probability per sex act, and the duration of infection in men. The longer the duration of infection in men the lower the transmission probability per sex act that will generate a given proportion of infected men. Our standard model for STDs has a transmission probability per partnership, which is adequate for an initial investigation of T vaginalis epidemiology, but a full understanding will require a more sophisticated appreciation of re-infection within partnerships. The transmission probability from women to men is probably higher than 50% over the duration of a long term partnership. However it might be a reasonable upper limit for short term partnerships, or per year within the partnership.
Lower bounds:
Here, the direction of transmission is of paramount importance but there are no data to determine this. Women who are partners of infected men may have infected those men rather than vice versa. Clearly transmission is occurring but it is not possible to decide exactly where the lower bounds lie.
Another problem is that the means of diagnosing T vaginalis was not consistent in these studies and the lower figures in the female to male studies may have resulted from the relative insensitivity of the diagnostic method used. Culture of a urethral swab, prostatic fluid, and semen14, 47, 48 was probably the most sensitive combination (before the introduction of molecular techniques) but this was not always undertaken. A further problem is the small sample size of many studies, a problem particularly apparent when estimating the proportion of infections that remain asymptomatic and their duration.
Asymptomatic infections
The propensity to cause symptoms is an important feature of an organism as it determines the “immediate” morbidity and influences the frequency with which infected individuals will spontaneously seek medical attention. When considering their epidemiological relevance “symptomatic” infections could be defined as those which cause subjective awareness of illness in the infected individual, while “asymptomatic” infection is infection which leads to either no symptoms at all or to symptoms that are insufficiently troubling to lead the individual to seek care. The rate of asymptomatic disease may therefore be influenced by the prevailing expectations of health of the particular population.
Since most studies of T vaginalis come from clinics, and are subject to important selection biases, it is not possible to determine the true proportion of patients with asymptomatic infection from these surveys. Nevertheless, they give some indication of the minimum proportion likely to occur in the broader community. Even in samples from the community the prevalent proportion of asymptomatic infections will only equal the proportion of incident infections that remain asymptomatic if symptomatic and asymptomatic infections have a similar duration. This is more likely to be true before the development of an effective treatment or in populations where symptoms go unrecognised.
Men: It was recognised in the pre-antibiotic era that the majority of men with T vaginalis infection had mild or no symptoms. In a study of 926 male military recruits in the 1940s, Feo10 found that 15% were infected with T vaginalis but that “all were relatively free of symptoms”. Only one of seven infected male contacts of women involved in a T vaginalis study in the United Kingdom admitted to symptoms when questioned11 and of 63 male partners of infected women identified in a subsequent study by the same author, 12 (20%) had no symptoms but the remaining 51 were said to have “very mild symptoms”.45 Eight of 13 (61.5%) infected male contacts of women identified in an STD clinic were asymptomatic.15 Studies before 1970 should be interpreted with caution as Chlamydia trachomatis diagnosis was not widely available and a proportion of symptoms may have been attributable to co-infection with T vaginalis and C trachomatis. A more recent study of 447 men attending an STD clinic in the United States found that 27/50 (54%) men with T vaginalis infection had symptoms,49 while in a high risk male population 24/49 (49%) had symptoms.25 It is reasonable to conclude that these latter two percentages are upper limits of symptomatic disease (table 1).
Women: Symptoms referable to infection with a specific STD may also be caused by non-transmissible pathogens or syndromes such as candidiasis or bacterial vaginosis, making the estimation of the proportion with symptomatic disease problematic. The only recent study to include a randomly selected community sample of women found that in 201 women living in rural areas of Papua New Guinea there was no statistically significant difference between women with T vaginalis and those who were uninfected with respect to symptoms.37 Similar results were found in a survey of STD clinic patients in the United States.50 In a study of women attending a naval obstetric and gynaecology clinic Peterson9 found that only 36% had symptoms compatible with T vaginalis infection. Feo51 found 13/24 (54.2%) postmenopausal women with T vaginalis to be symptomatic, while Wisdom and Dunlop found that 71.7% of female STD clinic attendees with T vaginalis were symptomatic.15 A community based study of Aboriginal women in northern Australia showed that approximately 10% of women with T vaginalis had reported symptoms at the time of diagnosis52 and in a Ugandan study only 19% of women with T vaginalis or bacterial vaginosis reported symptoms in the previous 6 months.53
Because of the potential biases associated with the data presented, which are likely to lead to an overestimation of the proportion with symptoms, we have assigned the average proportion of symptomatic women with T vaginalis infection as 0.4 and of men as 0.5.
It is unknown if symptomatic disease has a different coefficient of transmission from symptomatic disease and for simplicity we make the assumption that the two are identical.
Duration of infectiousness
The duration of infectiousness (D) is also very difficult to determine.
Men: One survey suggests that in industrialised settings the duration of symptoms in men before they seek treatment is short (median of less than 1 day)49 but a study in Zimbabwe showed that 78% of men with urethral trichomoniasis had symptoms present for more than 4 weeks.54 The studies from the pre-antibiotic era demonstrate that the duration may be longer but the evidence is conflicting and plagued by incomplete data, differing diagnostic criteria, and inconsistent protocols. Inoculation experiments in three volunteers, carried out in the 1950s, found the parasite for 4, 44, and 94 days respectively.46 A study of 19 untreated men who were partners of known infected women found that T vaginalis could be identified for up to 101 days before treatment was given. Only five of the 19 (26.3%) were seen to spontaneously resolve within 2 weeks.45 Weston and Nicol55 found that 10/38 (26.3%) men with T vaginalis infection spontaneously cleared the organism within 2 weeks of the presumed exposure, but overall there was a mean duration of at least 35 days (three patients had infection of greater than 84 days).
It is logical to conclude that patients who are aware of symptoms (and of their significance and have access to medical services) will have a shorter duration of infection than patients without symptoms. Only screening and contact tracing will identify asymptomatic individuals who will remain infected until natural recovery occurs. Unfortunately, there are few data to help estimate these respective values. Assuming that prolonged infection is the norm in the untreated individual but that spontaneous resolution occurs, we assigned a 120 day average duration of infection in men.
Women: Before metronidazole, treatment was of limited efficacy and many authors considered the disease to be of indefinite duration in women.56 This is supported indirectly by the observation of higher prevalence in older age groups in two surveys.14, 16 An age structured survey of STD prevalence in Aboriginal women in northern Australia38 demonstrated that unlike N gonorrhoeae and C trachomatis where prevalence decreases with age, the prevalence of T vaginalis increases with age, reaching 40% in the older than 40 years age group. These data demonstrate that there are important differences in the dynamics of infection between T vaginalis and the other two STDs. As the rates of partner change and sexual mixing patterns are properties of the behaviour of the host population that are independent of the three infections, it must be differences in the duration of infectiousness or the coefficient of transmission that are responsible for the discrepant prevalences. We believe that an extremely long duration of infectiousness best explains such a high prevalence of T vaginalis in the older age groups.
Model uncertainty and sensitivity analysis was investigated using Latin hypercube sampling (LHS) and a description of this work is available on request.57–59
TREATMENT EFFECTS
Efficacy of treatment
A single dose of a nitroimidazole (for example, metronidazole) results in cure rates above 90%60; however, for the purposes of the model we have assumed that cure rates are 100%.
“Syndromic management” versus screening
Syndromic management is the practice of treating individuals with a specific constellation of symptoms and signs according to a set protocol, without the need for a definitive laboratory diagnosis. The utility of this approach is that it is cheap, requires no laboratory services, and results in the immediate treatment of infected individuals. Its fundamental failing is that it does not deal with the majority of the infected population who are asymptomatically infected and who are only identified through screening (which identifies both asymptomatic and symptomatic individuals). In addition, symptomatic T vaginalis infection is usually manifest as vaginal discharge or itch and the performance of syndromic management protocols in this context have been questioned.61
“Serial” versus “constant” screening
In some areas of high prevalence there may be considerable opportunity for individuals to use health services (for example, in urban settings in developed countries) while in others the health services may be rudimentary (for example, many developing countries). In the former group, the ready availability of appropriate testing, treatment, and counselling may result in the provision of what we have called “constant” screening, in which a set fraction of the population is screened over a unit time. The magnitude of this fraction will be determined by a number of factors—for example, the health seeking behaviour of the population, the acceptability of the services, and the effectiveness of their promotion.
The effect of treatment on the endemic prevalence of disease was simulated by altering the modelled fraction of infected individuals treated. If we consider the process of case finding and administering appropriate drugs, then the rate at which people are screened and treated, φ, over time will lead to a fraction treated, F, over a given period, t. Thus, F=1 − e−φt.62 Over a year the rate of treatment required to reach this fraction, F, is given by φ = −ln(1 − F). To translate screening and treatment into a rate of recovery of those infected this rate was calculated from the fraction of cases that would be treated per year in the absence of spontaneous recovery. Alternatively, the effect of “serial” screening on treatment was simulated by removing a proportion of individuals at one time point from the infected class and placing them in the susceptible class. This process was repeated at intervals of 6 months, 1, 2, and 5 years.
Syndromic management was simulated by adjusting the recovery rates (or by removal from the infected class for “serial” treatment) of those with symptomatic disease. Screening or mass presumptive antibiotic administration was simulated by “treating” an identical fraction within both the symptomatic and asymptomatic groups. Treatment of infected partners was not included in either of the treatment simulations.
The mean parameter values obtained in the LHS simulations which produced a prevalence of female infection of 0.30–0.35 were used in the treatment simulations (table 3).
Descriptive statistics of output and input parameters for female prevalence of 0.30–0.35
Results
On the basis of community studies in sub-Saharan Africa we chose to view a third of sexually active women infected to be a “reasonable” estimate of the prevalence of infection in the communities of interest. We then used this as a starting point (with a little leeway—that is, 30–35% prevalence) in uncertainty analysis to indicate the combinations of parameter values which could generate such a prevalence (table 3). The parameter values that produce a prevalence of 0.30–0.35 are described using measures of central tendency and variation in table 3. Noteworthy are the high recovery rates for men and the low rates for women indicating that the estimates derived from the literature are consistent with observed prevalences.
In our model we have simulated the effects of “syndromic management” and screening, applied in a “serial” and “constant” programme (fig 1). It is not surprising, given the proportion of asymptomatic disease, that even very high levels of syndromic management coverage (which are almost certainly unobtainable in the field) result in only modest reductions in the endemic prevalence of infection. On the other hand, modest (and presumably achievable) levels of coverage of screening lead to significant reductions in the prevalence of T vaginalis, with “constant” screening (facilitated by a good health infrastructure) being more effective than “serial” screening. We have assumed that 50% of disease is asymptomatic for the model but we believe that this is a conservative estimate (tending to underestimate)—the true benefit of syndromic management is therefore likely to be less than the simulations suggest.
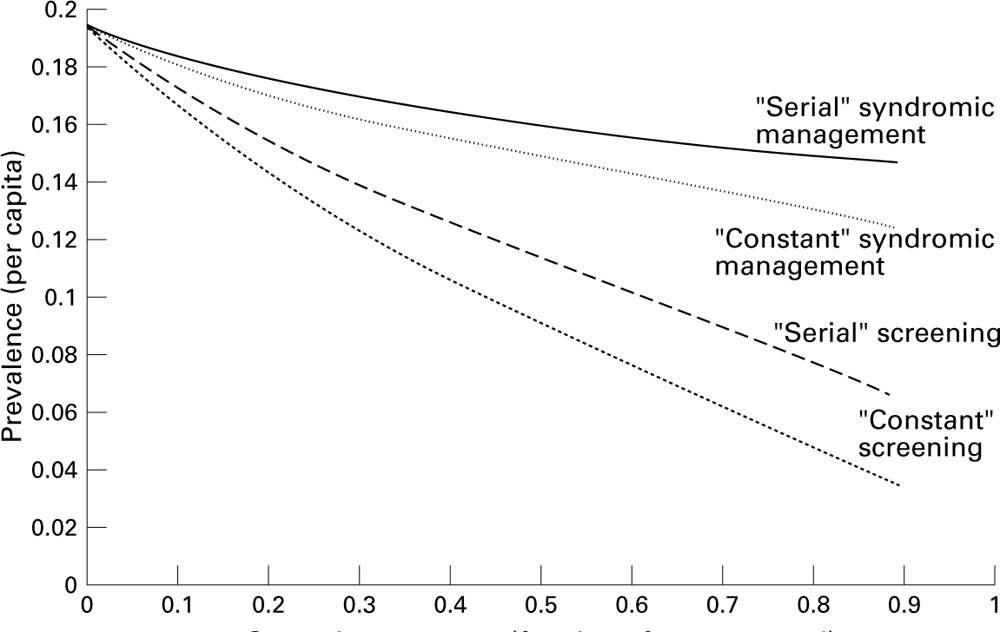
The effect of different levels of coverage (fraction of infections treated) on the equilibrium prevalence of infection for “serial” and “constant” syndromic management (that is, treatment of symptomatic cases only) compared with serial and constant screening of mass antibiotic administration for the whole population. The mean parameters from table 3 were used as a baseline.
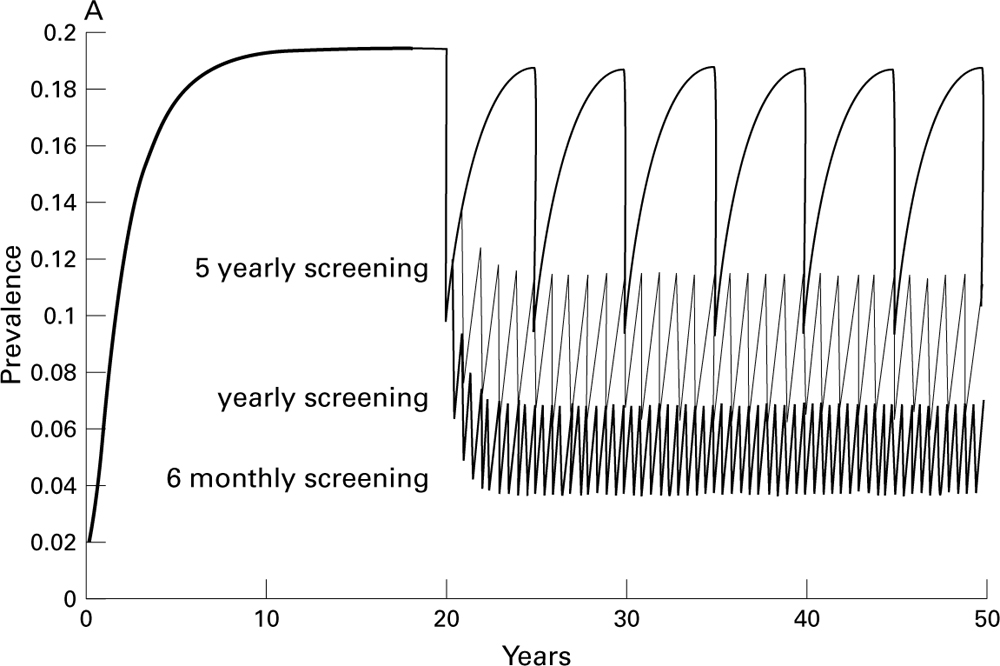
The effect of different coverage rates and screening intervals on the endemic prevalence is shown in Figure 2A and B. Screening at 5 yearly intervals has minimal effect on prevalence regardless of coverage, while 6 monthly screening is highly effective (but probably impractical). An interval of 12 months may be achievable in some healthcare systems and will result in substantial reductions in prevalence of disease.

The impact of serial treatment on the prevalence of Trichomonas vaginalis starting at year 20 using mean parameters from table 3. (A) The impact through time of the frequency of treating a random sample of 50% of infections at different intervals. (B) The relation between the fraction of infections treated at each round (screening coverage) and the average steady state prevalence for treatment of infections at different intervals.
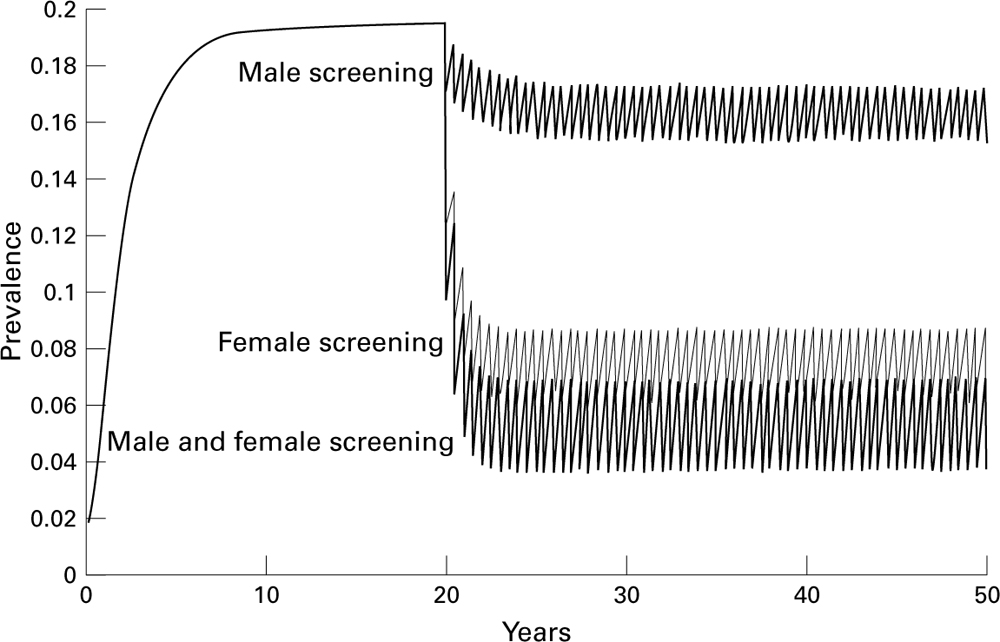
Assuming 50% coverage of the population occurring at yearly intervals, we simulated the effect of screening either both sexes together or one sex alone (fig 3). Screening men alone has minimal impact on prevalence, and although the nadir of prevalence is lower in screening of both sexes, there was only a modest difference in the total prevalence at the due time of the next screen if women only were screened.
{kind=link}
{kind=link}
{kind=link}
The impact of “serial” screening of one or both sexes at yearly intervals with a 50% coverage using mean parameters from table 3.
Discussion
The absence of prospective data in well defined populations means that the true dynamics of T vaginalis infection are unknown. Nevertheless, the most striking feature of the epidemiology is the consistently high prevalence found in women in developing and disadvantaged populations.
The effects of T vaginalis on pregnancy outcome have been known for many years20 and are now receiving increased attention.4 It is possible that treatment of women with T vaginalis in pregnancy will reduce the incidence of premature rupture of membranes and premature labour, although one study has failed to show this.63 Of course, lowering the risk of infection in the first place through reductions in the community prevalence of the disease is a better long term option.
Although some authors consider the epidemiology of T vaginalis to be similar to other bacterial STDs,64, 65 the few studies which look at age specific prevalence14, 16, 38 demonstrate a continuous increase with age, a feature that is not common to N gonorrhoeae or C trachomatis. Targeting of particular age groups is sometimes suggested as a strategy for STD control but if N gonorrhoeae or C trachomatis are chosen as the marker diseases, older women infected with T vaginalis will not be identified.
In addition, T vaginalis almost always occurs at higher prevalence than the bacterial STDs in studies in disadvantaged communities. These observations can best be explained by postulating an extremely long duration of infectiousness, an assumption supported by the pre-antibiotic literature. In our model a duration of 3–5 years was needed in the female group to produce a prevalence of 35% in women. The duration in men is almost certainly shorter, as a result of the protective effects of non-specific urethral immunological defences, the physical clearing by the stream of urine and possibly the increased proportion of men with symptomatic disease which brings them to medical services. The relative rarity of T vaginalis in developed country populations is likely to be due to the identification of T vaginalis through Pap smears, antenatal care, and through the increased rate of health seeking behaviour (linked to adequate access to suitable services) experienced by individuals in these settings. The widespread treatment of the syndrome of bacterial vaginosis with nitroimidazoles may also have had an important effect. In addition, there may be differences in the interaction of sexual networks and sexual core groups between the two populations.
The fact that the epidemiology of T vaginalis differs from the two major bacterial pathogens is important as it influences the approach that is required to design control strategies. The model we have described is a simple representation of the presumed dynamics of T vaginalis infection. The uncertainty and sensitivity analyses show that there are a number of important gaps in our knowledge about the epidemiological parameters that constitute the model. Nevertheless, the model demonstrates a number of salient points: (i) the importance of the proportion of individuals with asymptomatic disease in influencing the success or otherwise of the syndromic approach to STD control. There is uncertainty about the fraction of infections that remain asymptomatic, but what is not in doubt is that asymptomatic infections are common and the greater the proportion of infections without symptoms or the less well recognised they are the less the impact of syndromic management. Without a general improvement in health care it is clear that any programme for T vaginalis that relies solely upon this strategy will be unlikely to achieve a sustained decrease in the total prevalence of disease regardless of the degree of patient coverage; (ii) the frequency of screening will determine the ultimate endemic prevalence; (iii) the presumed asymmetry of the recovery rates for male and females means that treatment of women is likely to have a greater effect on prevalence than treatment of men. The treatment of both sexes rather than just women will result in only a small decrement in the prevalence. This result depends upon the duration of infectiousness being lower for men than women, which seems to be a realistic assumption. Its consequence is that energies should be directed more to female screening than to male screening, which probably occurs already in reality as women tend to use health services on average more often than men in most areas where T vaginalis in endemic; (iv) “constant” screening (that is, the provision of good primary healthcare STD services with good population outreach) is more effective than “serial” screening, because for a given coverage the fraction of infections actually treated is greater. In effect we are comparing treating a given percentage of infections at one point in time with treating a fraction of all cases. Unfortunately the impoverishment of most endemic areas means that such services are uncommon. Regular “serial” screening may be more achievable in most settings.
In presenting our results we have chosen to use one set of parameter values, but the impact of varying parameters on interventions is easily summarised. To generate a particular endemic prevalence of infection before an intervention there is a trade off between the duration of infectiousness, the contact rate, and the transmission probability. A shorter duration of infectiousness implies a higher contact rate or a higher transmission probability. The higher the latter two values the more rapidly infection can bounce back following around of treatment. A shorter duration of infectiousness would reduce the impact of both continuous and serial interventions.
An important assumption in this model is that identification and treatment of disease does not lead to any change in sexual behaviour—that is, reduction in number of sexual partners or use of condoms. It is likely that properly conducted screening activities which are linked to counselling services will have some effect upon behaviour and would result in a larger reduction in prevalence than is predicted from these simulations.
The advent of non-invasive testing for STDs using amplification technology (for example, from first void urine samples in men and self administered swabs in women) should facilitate prospective, age structured epidemiological studies of T vaginalis in the community, which will be useful in helping to shape future control programmes. Diagnostic tests will probably remain expensive and the hyperendemicity of the disease in many populations raises the possibility of instituting widespread treatment of all women regardless of symptoms, signs, or laboratory investigations. In some areas the positive predictive value for T vaginalis infection of the marker of residence in the population will equal the prevalence of the disease—that is, 35–50%, a level that many investigators would be happy to achieve for a sophisticated diagnostic test for other pathogens of lower prevalence. Recommendations for single dose nitroimidazole therapy for all women who have been sexually active at any stage in their life may be appropriate and could be instituted at family planning clinics and other primary healthcare facilities in areas of known high endemic prevalence.
Infection with T vaginalis has been largely ignored by most health professionals since its discovery over 160 years ago but its relative importance is now beginning to be recognised. Control of the disease is dependent on a cheap, safe, and well tolerated antibiotic and should not be ignored
Acknowledgments
Contributors: The mathematical model was developed and parameterised in collaboration between the authors. FB carried out the literature review; GG coded the model solution and the sensitivity analysis routine; and FB carried out and analysed the simulations. Both authors drafted the manuscript.
The authors thank Neil Ferguson, Azra Ghani, and Andrew Roddam for helpful comments. GPG is a Royal Society University Research Fellow. FJB was supported by a Wellcome Trust Travelling Fellowship.
The appendix to this paper is available on request from the journal office.