Article Text

Abstract
Objectives: This study measured the effect of information about family planning methods and STD risk factors and prevention, together with personal choice on the selection of intrauterine devices (IUDs) by clients with cervical infection.
Methods: We conducted a randomised, controlled trial in which family planning clients were assigned to one of two groups, the standard practice (control) group in which the provider selected the woman's contraceptive and the information and choice (intervention) group. The study enrolled 2107 clients in a family planning clinic in Mexico City.
Results: Only 2.1% of the clients had gonorrhoea or chlamydial infections. Significantly fewer women in the intervention group selected the IUD than the proportion for whom the IUD was recommended in the standard care group by clinicians (58.2% v 88.2%, p=0.0000). The difference was even more pronounced among infected women: 47.8% v 93.2% (intervention v control group, p=0.0006).
Conclusions: The intervention increased the selection of condoms and reduced the selection of IUDs, especially among women with cervical infections, for whom IUD insertion is contraindicated.
- reproductive health
- sexually transmitted diseases
- contraception
Statistics from Altmetric.com
Introduction
Evidence shows the prevalence of reproductive tract infections (RTIs) and sexually transmitted diseases (STDs) among women to be high in various developing countries.1 In many of these same countries, public policy has promoted the widespread adoption of long acting, provider dependent contraceptive methods. However, non-barrier contraceptive methods do not protect against STDs and can increase the risk of pelvic inflammatory disease (PID).2–12 For example, the intrauterine device (IUD) is an extremely effective contraceptive, with pregnancy rates less than one per 100 woman years,3, 8, 9 yet it does not protect against STDs and, in fact, can increase the risk of PID. Once inserted, IUDs can be used for years (the Copper T is approved for up to 12 years of use). Estimates from the demographic and health surveys and similar surveys indicate 12% of reproductive age women who are married (more than 106 million women worldwide) use IUDs13 making this the second most commonly used family planning method and the most commonly used reversible method in the world.14 In Mexico, 22% of contraceptive users use an IUD, and the Mexican Social Security Institute (IMSS) provides 44% of modern contraceptives.15
The safe provision of IUDs in any environment depends on adequate training, clinical experience, access to laboratory services, technical skill, and commitment to high quality service delivery. IUDs are most appropriate when exposure to STDs is minimal. In any environment, IUD insertion must be performed under strict aseptic conditions and women must be free of genital tract infections to minimise the possibility of infecting the upper reproductive tract.6
Clinical algorithms have been developed by the World Health Organisation to identify women with signs and symptoms in clinic settings where laboratory testing is not feasible16–21 and variants of these have been used to identify women who should not receive IUDs. However, these algorithms have been shown to be insensitive with poor positive predictive screening value for STDs.16
Since women with cervical infection are often asymptomatic, we tested another simple procedure, providing information and contraceptive choice, which all family planning clients should receive, to determine if this helps avoid the use of IUDs by women who have cervical infections. This procedure involved providing women with information about contraceptives, their benefits and risks, and information about STDs and PID after which they were asked their choice of contraceptive method. The purpose of this study was to determine the combined effect of providing this information and clients' choice on the selection of IUDs for contraception.
Methods
SUBJECTS
We designed a randomised, controlled trial in which family planning clients were assigned to a standard practice (control) group or to an information and choice (intervention) group. The study design was reviewed and approved by the institutional review boards of Instituto Nacional de Salud Publica and the Population Council. Our hypothesis was that patient choice after provision of information on STD risk and family planning methods would result in more appropriate IUD selection than standard clinical practice. In standard clinical practice, physicians routinely recommend a contraceptive method based on their clinical examination and any chart review or verbal interaction with their clients. We hypothesised that clinicians would correctly not recommend IUDs for 30% of all laboratory identified chlamydia/gonorrhoea positive clients and that, given informed choice, 50% of infected women in the intervention group would correctly not select an IUD. The study was designed to enrol 1460 (730 per study group) family planning clients to conduct a one sided test of this hypothesis, given a prevalence of gonorrhoea and/or chlamydial infections of 10%, an alpha (type I) error of 0.05, and a statistical power of 80%.
We selected a large, sophisticated polyclinic that is part of the Mexican Institute of Social Security (IMSS) system in Mexico City as the study site. The polyclinic provides 70 different healthcare services serving a population of 280 000 from 162 neighbourhoods and is open Monday to Friday 8 am to 8 pm. The family planning service sees 20–50 patients in each of two shifts per day and provides IUDs, oral contraceptives, and condoms. Patients desiring oral contraceptives or condoms may go directly to the family practice service in the polyclinic where these are distributed. During the study period, some patients may have come to the family planning service from other services through referral or because they heard that the family planning service was providing free STD screening.
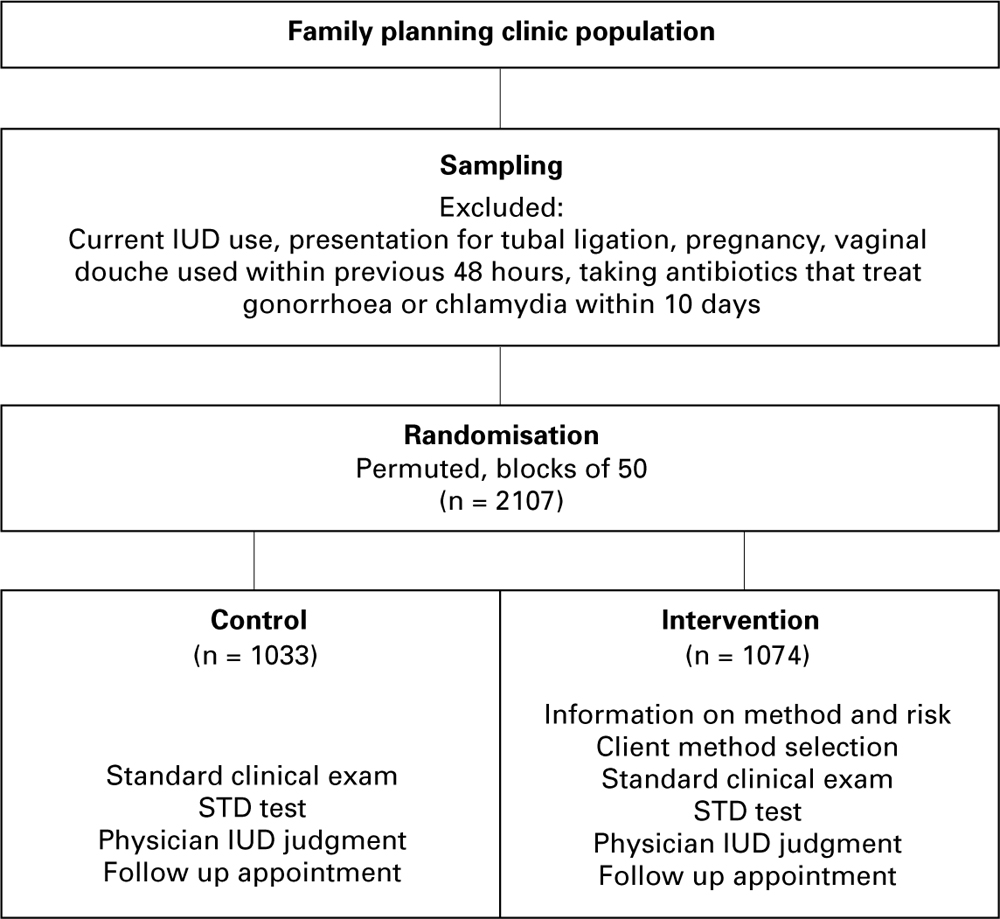
All women who presented to the family planning clinic and gave informed consent were eligible to participate in the study except those currently using an IUD, those coming for tubal ligation, those who were pregnant, had used a vaginal douche within 48 hours or had taken antibiotics that treat gonorrhoea or chlamydia within 10 days of presentation (fig 1). The refusal rate was 2%. We extended the study after a preliminary data review showed the prevalence of infection to be much lower than expected (2% instead of 10%). Ultimately, 2107 women were assigned to study groups, 1033 to the control and 1074 to the intervention groups, by permuted randomisation done in blocks of 50 to assure equal sample sizes between the groups.
{kind=link}
Study group assignment.
Each woman answered a short questionnaire about her background, reproductive health status, and past contraception. Women in both arms received a standard clinical examination by a medical officer and free STD testing. After completing the physical examination, the medical officer recorded for each woman whether he thought the client should or should not be offered an IUD. We purposefully did not ask about women's decisions in the control group to avoid any effect that the question itself might produce on routine care. All women returned for a follow up visit after laboratory results were available (usually within 2 weeks) to receive a contraceptive method and be treated for identified infections.
INTERVENTION
Women assigned to the intervention group received a 20 minute one on one information session from a nurse before physical examination and STD sampling. A 14 page laminated colour flip chart was developed on site before initiating the intervention. The flip charts were used as the information presentation guide in all sessions to ensure standardisation.
Three registered nurses with previous experience in research were employed, two to conduct the information sessions (one per shift) and a third to screen the potential subjects, randomly assign them to one of the two study arms, and fill in when either of the other nurses was absent.
The study purpose and design were carefully explained to the nurses, who were provided with background materials on STIs, contraceptive methods, and counselling techniques and then participated in an intensive 2 day training session. The training session included technical education on contraceptive methods and STIs from a gynaecologist, question and answer sessions, and role play simulations on counselling techniques, and establishing rapport with the clients. The nurses were trained until their presentations were uniform in use of the pretested flip chart to present the information and the model penis to provide condom use demonstrations. They were also trained to provide standard responses to common questions regarding contraceptive methods and STDs and ways for women to convince partners to use condoms.
Women were encouraged to ask questions at the beginning of each information session. During the information session, the nurse explained the advantages and disadvantages of condoms, pills, and IUDs (the reversible family planning methods available at that clinic) and described STDs and their risk factors with particular reference to the different contraceptives available.
During this session, women were informed about behavioural correlates of STD risk but not asked any questions about whether they viewed themselves to be at risk of STDs as a result of their own or their partner's behaviour. Such questions may inadvertently or purposefully generate inaccurate information. At the end of the counselling session, women were asked to select the contraceptive method they felt to be most appropriate for themselves on a confidential form.
LABORATORY ANALYSIS
Vaginal secretion specimens were taken daily at the IMSS clinic, and chemical and microscopic analyses of bacterial vaginosis, candidiasis, and trichomonas were conducted at the clinic laboratory according to conventional methodology. In addition, endocervical specimens were obtained and transported at 4°C daily to the national institute of public health in Cuernavaca, Morelos where they were stored at −20°C until standardised molecular diagnostic analyses were performed to detect Neisseria gonorrhoeae and Chlamydia trachomatis by means of nucleic acid hybridisation based test, using the Pace 2C and Pace 2 kits from Gene-Probe Inc, San Diego, CA, USA.22
STATISTICAL ANALYSIS
To verify the comparability of the intervention and control groups, we conducted bivariate analyses using χ2 and Student's t tests of the sample characteristics and results. We also conducted logistic regression analyses to determine the association between the intervention and method choice adjusted for potentially confounding factors. Data were entered in foxpro and analysed using spss/Windows 6.0.
Results
Sociodemographic and reproductive characteristics and the number of infected women found in each group (21 in the control and 23 in the intervention groups) were remarkably similar between study groups (table 1). However, more women in the intervention group had used IUDs in the past (14.8% v 10.8%, p=0.006) and fewer had used contraceptive suppositories in the past (0.7% v 1.5%, p=0.048).
Study group characteristics
Only 44 of 2107 study participants had gonorrhoea (n=1) or chlamydia (n=43). Overall, fewer women in the intervention group selected the IUD compared with women recommended by physicians to use the IUD in the standard care group (58.2% v 88.2%, p=0.0000, table 2). The difference was even more pronounced in women with gonorrhoea or chlamydia, where 47.8% of infected women in the intervention group inappropriately choose the IUD compared with 95.2% of infected women in the control group for whom physicians recommended the IUD (p=0.0006).
IUD choice
Physician recommendation was also recorded for the intervention group women. There, physicians recommended IUDs for 90.0% of all women in the intervention group (p=0.0000 v women's choice) and for 87.0% of infected women in the intervention group (Yates's corrected p=0.012 v women's choice). More infected than uninfected women in the intervention group chose condoms as their method of contraception (21.7% v 15.5%), although not significantly more.
We conducted logistic regression analyses to determine the effects of the intervention, having gonorrhoea or chlamydia, and the interactive effects of receiving information and being infected on IUD selection. Logistic regression analyses were also conducted adjusted for standard covariates (age, education, marital status, parity) and for variables that are proxies of socioeconomic status found to be statistically different between the intervention and control groups in the general or infected sample (colour TV, refrigerator, and videocassette ownership, reported number of sex partners, and previous IUD use).
In the unadjusted regression model, there is a highly significant (p=0.0000, table 3) reduction in the estimated selection of IUD associated with the intervention. This model estimates over five times as many women in the intervention group did not choose IUDs as a contraceptive method than physicians recommended for women in the control group. Infected women were estimated to be almost three times more likely to select or have a clinician select an IUD as their method of choice (not significant). The interaction of receiving the intervention and being infected, however, was associated with an estimate of being four times less likely to choose an IUD above and beyond the individual effects of receiving the intervention or being infected. The adjusted odds ratios are very similar to the unadjusted results. Analyses of infected women demonstrate a significant protective effect of the intervention against inappropriate IUD selection (p=0.0053 unadjusted, p=0.0130 adjusted, table 3).
Logistic regression results
Conclusions
Providing information about family planning methods, STD risk factors, and choice of contraceptive method to family planning clients may reduce the inappropriate and potentially harmful selection of IUDs as a contraceptive method and increase the selection of condoms for contraception in clinics providing these services, even where the IUD is presented as the most effective contraceptive method (as it was in this study's intervention). The increase in condom selection in the intervention group cannot be attributed to the study's condom distribution as condoms were provided to all study participants in the interim between their clinic visit and receipt of laboratory results.
The results of this study confirm the belief that physicians' “perception” of women's STD risk places women at greater risk of inappropriate IUD insertion than women's informed choice. Clinicians' inability to identify family planning clients with chlamydial and gonococcal infections may be a consequence of several factors: emphasis on family planning and lack of training in reproductive health issues including STDs and RTIs; lack of awareness of the magnitude of the problem; limited time spent with each client; lack of sensitive or specific clinical signs; and the strong promotion of IUDs in the Mexican public health sector.
This study did not try to determine whether a particular message (that is, risk behaviour v method benefits) from the information session accounted for the observed results. The extent to which women's choice was affected specifically by the content of the information received rather than simply by being given a choice in method selection may require further investigation. However, women seeking family planning services should universally receive information about STDs, family planning methods and their relation to STDs, and clients should be allowed to choose their preferred method unless that method is contraindicated for them.
Further evaluation of this intervention should be conducted in other settings where the prevalence of gonorrhoea and chlamydia is higher and where the contraceptive method mix is different to determine the extent to which the study results are generalisable. Since the implementation of one on one information sessions with providers may not be feasible or affordable in all settings, we are currently testing the impact of videotaped information shown in waiting rooms to determine if this less expensive mechanism is associated with similar outcomes of clients' method choices.
The best way to screen for STDs in services providing IUDs has not yet been determined; universal laboratory diagnosis of STDs (chlamydia in particular) would be ideal, but is not conducted owing to the high costs of the required materials in many parts of the developing world.23 Providing mass prophylactic treatment to all IUD users is not standard practice because of its costs and unnecessary treatment of uninfected women. The use of clinical algorithms based on visual inspection and client questioning has been shown to be inadequate.16–20 Restricting IUD insertion when STD prevalence is low and many women have an exceedingly low risk of developing PID as a result of IUD use seems unwarranted, especially in areas where contraceptive alternatives are limited.
In this study, women who were asked to select the contraceptive method they felt was most appropriate after participating in the information session were half as likely to choose the IUD. Giving family planning clients contraceptive and STD information and an opportunity to choose a contraceptive method is an imperfect, but powerful and preferable, alternative to current practices that are dependent on clinicians' judgment alone to reduce the risk of PID associated with IUD insertion. This intervention also does not exclude the IUD as part of the array of methods. In addition, giving women information and choice increases women's participation in their own reproductive health care.
Acknowledgments
New York and Mexico Population Council staff, together with colleagues from the Mexican National Public Health Institute (INSP), conducted this project with funds from the Andrew W Mellon Foundation. We would like to express our gratitude for the invaluable assistance of our Mexican partner organisations, the Mexican Social Security Institute and the National Public Health Institute. We would also like to acknowledge support from our US partner organisations in implementing this study, AVSC International, the International Center for Research on Women and, their partner organisation, the Mexican Institute for Research on the Family and Population (IMIFAP, AC), and to the Pacific Institute for Women's Health.
Contributors: All authors participated in the writing and approval of this article; ECLP, NLS, BW, AL, JS, and CC are responsible for the conceptualisation and design of the project; ECLP, NLS, BW, AL, CJC-G, CC, and AH are responsible for the data analysis and interpretation.