Article Text

Abstract
Objective: To assess the impact of the sexual component of AIDS and HIV campaigns on transmission of HIV and other sexually transmitted infections (STIs).
Design: Comparison of time series data.
Setting: England, 1971–1999.
Outcome measures: HIV transmission and diagnoses among men who have sex with men (MSMs), rates of attendances and specific STI diagnoses (per 100 000 total population) at genitourinary medicine (GUM) clinics.
Results: Awareness of AIDS and campaigns in 1983–4 among homosexual men coincided with substantial declines in transmission of HIV and diagnoses of syphilis among MSMs. During general population campaigns in 1986-7 new GUM clinic attendances requiring treatment fell by 117/105 in men and 42/105 in women. Rates for gonorrhoea fell by 81/105 and 43/105 and genital herpes by 6/105 and 4/105, respectively. Previous rises in genital wart rates were interrupted, while rates of attendances not requiring treatment (the “worried well”) increased by 47/105 and 58/105 for men and women, respectively. Since 1987 diagnoses of HIV among MSMs have not declined, averaging 1300–1400 annually. Following a period of unchanging rates there have been substantial increases in GUM attendances requiring treatment, notably for gonorrhoea, syphilis, and viral STIs since 1995.
Conclusions: Self help initiatives and awareness among homosexual men in 1983–4 contributed significantly to a fall in HIV transmission among MSMs, and the general campaigns of 1986–7 were associated with similar effects on all STI transmission. Both effects seem to have occurred through changing sexual behaviour, and probably contributed to the UK's low national HIV prevalence. Bacterial STI incidence has increased significantly since 1995 and there is no evidence that recent prevention initiatives have reduced HIV transmission among MSMs, hence sexual health initiatives need to be comprehensively reinvigorated in England.
- HIV
- gonorrhoea
- syphilis
- interventions
- health promotion
- homosexual males
- heterosexuals
- England
Statistics from Altmetric.com
Introduction
The primary purpose of programmes intended to control sexually transmitted infections (STIs) is the interruption or reduction of transmission. Activities that contribute to achieving this goal include the reduction of risky sexual behaviours, case finding, screening, and partner notification.1 Programmes targeting human immunodeficiency virus (HIV) are no different in this respect from those aimed at other STIs.
AIDS cases began to be diagnosed in the United Kingdom in late 1981. Indigenous HIV transmission then accelerated abruptly in the early 1980s, primarily through sex between men.2 Public health responses began in 1983–4 with information and awareness initiatives run by, and directed at, members of the gay (male homosexual) community. They were followed, in 1986, by campaigns for the whole population (table 1).3 These interventions were more timely and vigorous than in other European countries4 and some have suggested that this is the reason that HIV prevalence in the United Kingdom is lower than in most of continental Western Europe.5, 6 However, the campaigns, and ongoing programmes, were also criticised as being unfocused, wasteful, or unnecessary.7 This analysis aims to evaluate the possible impact on sexual health outcomes of the anti-AIDS campaigns by examining national time series data for temporal associations between the interventions and key outcome measures: HIV transmission and diagnoses among men having sex with men (transmission through drug injecting is outside the scope of this analysis, and most of the heterosexually transmitted HIV infections diagnosed in the United Kingdom were acquired abroad8), attendances, and diagnoses of specific STIs at genitourinary medicine clinics. This is the first national evaluation for the United Kingdom using HIV statistics and STI surveillance data.
AIDS and HIV awareness and related sexual health promotion campaigns, UK 1983–99
Methods
The period 1971–99 was chosen. A period extending back to the start of the 1970s was investigated because changes in STI epidemiology were taking place in the 1970s and it was important to distinguish these longer term trends from those that might be attributed to AIDS awareness and campaigns in the 1980s and 1990s. The analyses were confined to England as detailed STI data were only available for that area. Details of AIDS awareness and campaigns from 1983 were gathered from historical sources: published articles, the HIV-AIDS media library at the London School of Hygiene and Tropical Medicine, Health Education Authority files, press records and discussions with historical authorities, and those active in the field.
Estimates of HIV transmission among men having sex with men (MSMs) were derived using back calculation2 based on data to the end of 1995 (since 1996 such estimates have been profoundly affected by more effective therapy), and reports of new HIV diagnoses corrected for reporting delays and averaged to overcome seasonal reporting fluctuations. Routine data on annual attendances at genitourinary medicine (GUM) clinics in England were examined for trends.9 Categories examined were total attendances, new attendances requiring and not requiring treatment, and four specific STI diagnoses whose reporting format changed little over the period; infectious syphilis (KC60 code A1-A3), uncomplicated gonorrhoea (B1-B2), all genital herpes (C11) and all genital warts (C10). (Chlamydia and non-specific urethritis were excluded; chlamydia testing only became available in the late 1980s when the chlamydia diagnosis started taking cases from “non-specific urethritis.” These two categories were therefore not useful for time trend analysis over the study period.) Male infectious syphilis was especially associated with MSMs in the 1970s and 1980s10 (Routine annual GUM clinic returns did not start to identify subtotals of selected infections as being contracted through sex between men until after 1987) and male homosexual transmission of syphilis was monitored by annual ratios of male to female infectious syphilis cases.
Otherwise data were analysed separately for males and females and total population rates per 100 000 were calculated using mid-year population estimates for England from the Office for National Statistics. The annual rates of the STI categories were analysed with stata 6.0 for Windows using normal regression models to test for trends. The pattern of change across the whole period was described, estimating linear trends. Probabilities expressed in the results are the likelihood of differences or changes being by chance alone and refer to differences between groups (males v females), differences from no change in rates (for rises or falls in rates), or differences in rates over time (for when trends in rates seem to have steepened or flattened). The impact of the sexual component of the campaigns was examined by observing the trends in rates over narrower periods before, during, and after the most intense interventions of 1983 to 1984 (homosexual males) and 1986 to 1987 (general population).
Results
AIDS AND HIV SEXUAL HEALTH CAMPAIGNS
Attempts to spread information on AIDS, and how to avoid it, began informally in the male homosexual community in early 1983, led by various non-governmental organisations (table 1).3, 4 The gay press gave extensive coverage to AIDS issues thereafter resulting in growing awareness in the gay community between 1983 and 1984 (table 1).3 A government led programme of education for the general population began with a major campaign in March 1986. There were larger campaigns in the winter of 1986-7 (including a leaflet sent to every household in January 1987) and the spring of 1987. These generated intense media coverage. In “AIDS week” in February 1987 the topic dominated all broadcasting schedules.3, 4 After 1987 general and MSM programmes continued at lower intensity (table 1). Notable features were a character with HIV appearing in a television serial (EastEnders) (1990), personal testimony from prominent people (1991), and a new UK HIV/AIDS strategy in 1995.11 Two periods of intense national publicity could therefore be identified; a mix of awareness and then self help campaigning among MSMs from early 1983 to the end of 1987 and a more identifiable set of campaigns for the general population, from March 1986 to the end of 1987.3, 4 Both periods lacked distinct ends as they evolved into ongoing anti-HIV sexual health promotion. (The periods are indicated in the figures by vertical lines.)
Trends in HIV transmission and new attendances at NHS GUM clinics during and after awareness and AIDS campaigns
HIV TRANSMISSION THROUGH SEX BETWEEN MEN
Back calculation estimates indicate that incidence of HIV among MSMs was most intense around 1983 with about 6000 transmissions occurring by 1984. A rapid decrease in transmission that year was followed by plateauing (fig 1). Estimated numbers of new transmissions and diagnoses changed little after 1987, averaging 1300 to 1400 per annum (fig 1).

Back calculation estimates of HIV incidence in homosexual and bisexual men: England and Wales 1979–96 (median and 95% confidence intervals) and new diagnoses of HIV probably acquired through sex between men.
NEW ATTENDANCES AT NHS GUM CLINICS
Over the whole period (1971–99) the annual number of attendances, seen at GUM clinics increased threefold from 299 905 to 1 052 719. (Tables of annual data totals are available on the STI website.) The upward trend was steeper in females than males (p<0.001) and from 1994 female attendance rates overtook those of males (fig w1 on the STI website). Within these general trends there were different patterns for component categories.
NEW ATTENDANCES REQUIRING AND NOT REQUIRING TREATMENT
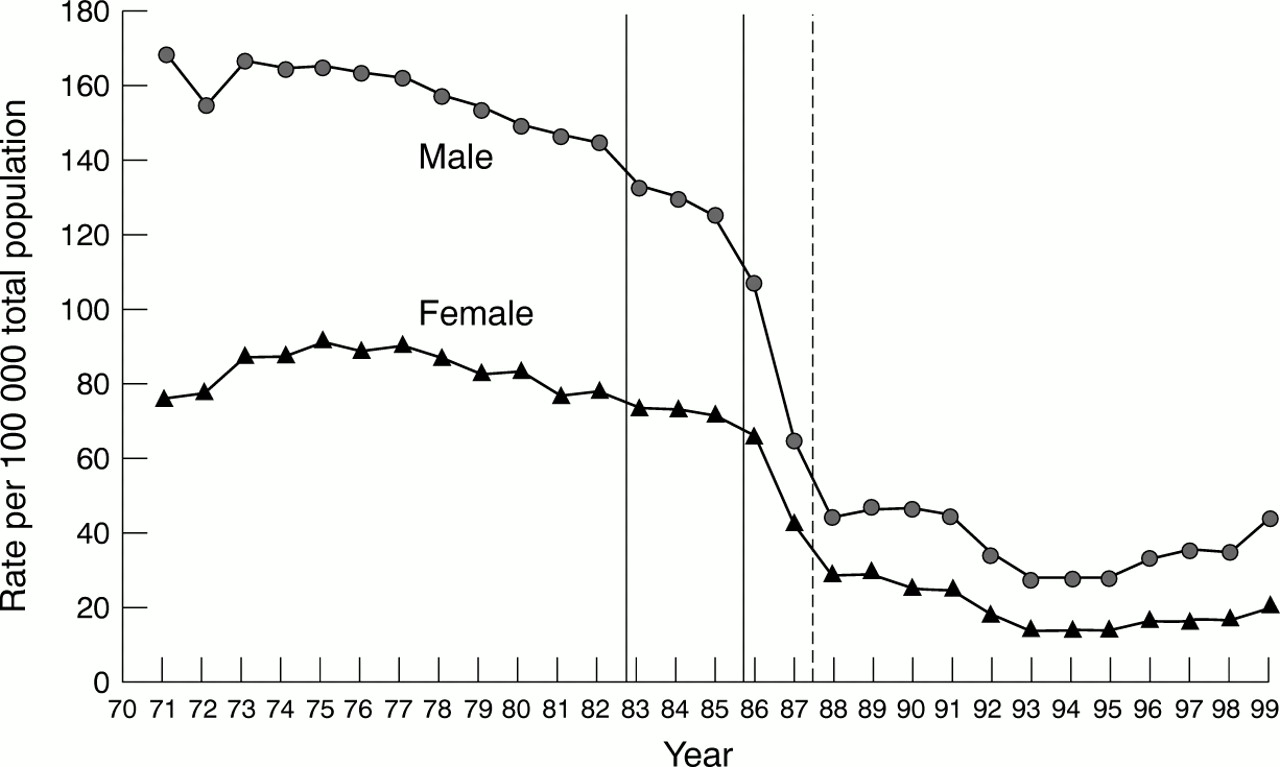
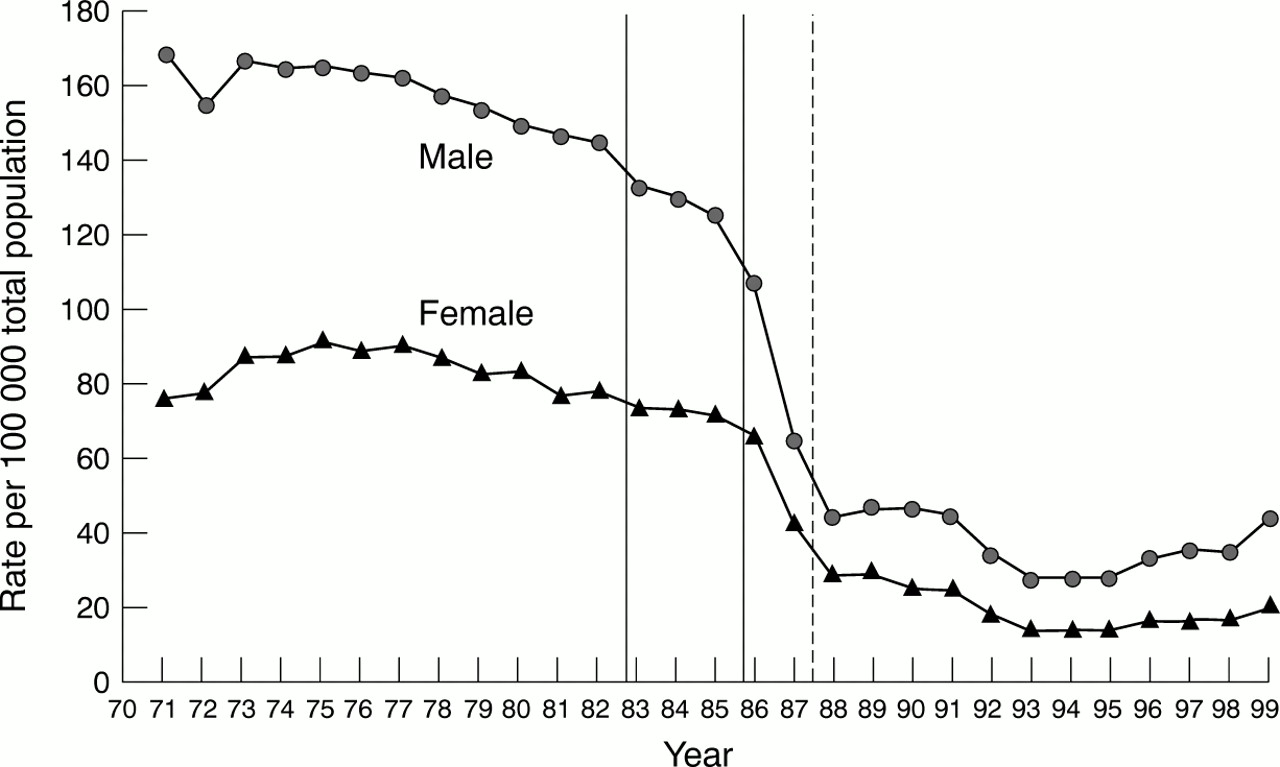
Annual numbers of attendances requiring treatment more than doubled from 147 423 to 361 020 (fig 2). Between 1971 and 1986 male rates (per 100 000 total male population) increased with an average annual rise of 19.1/105. This upward trend was significant (p<0.001). For females the rate also increased, on average by 16.2/105 annually (p<0.001). During 1987, the rates fell (fig 2) by 117/105 for males and by 42.1/105 for females. Rates of attendances not requiring treatment (“the worried well”) unlike those of attendance requiring treatment rose rather than fell, male by 47.4/105 and 57.8/105 in men and women respectively. Rates in both sexes declined again in 1988. In contrast, between 1987 and 1995, rates of male attendances requiring treatment declined by an average of 7.6/105 annually. Female rates re-attained and exceeded the 1986 level by 1988, but then remained essentially unchanged between 1988 and 1994 with no evidence of an upward or downward trend (p=0.81). Between 1995 and 1999 male rates increased again at an average annual increase of 50.5/105. The rising trend was significant (p<0.001), and rates regained and exceeded 1986 levels (fig 2). Female rates also rose steeply and significantly at an average of 43.0/105 per annum (p<0.001).

Annual rates of new attendances requiring treatment at genitourinary medicine clinics in England; males and females, 1971–99.
Trends in specific diagnoses during and after awareness and AIDS campaigns
INFECTIOUS SYPHILIS
The annual number of new diagnoses decreased from 1606 to 401 (fig 3A). Trends differed for males and females. Between 1971 and 1978 male rates rose by an average of 0.7/105 annually. Rates declined between 1978 and 1983, by an average of 0.6/105 annually. A steeper decline began in 1983 with the rate falling by a total of 6.3/105 by 1988. The rate of decline was significantly steeper than in the preceding period (p<0.001) (fig 3A). The fall was statistically significant. Rates remained low between 1988 and 1998. There was a rise in 1999 especially among gay men.9 Female rates were lower but also declined after 1982 (fig 3A). The male to female ratio increased slowly until the early 1980s peaking at 8:1 in 1983 because of a fall in female cases that year (fig 3B). There was then a more rapid decline to 2.7:1 in 1987. The declines in MSM HIV transmission, male infectious syphilis, and the male to female syphilis ratio coincided with the AIDS awareness and campaigns among homosexual men in 1983-4 (figs 1 and 3).


(A) Annual rates of new attendances at genitourinary medicine clinics: England with diagnoses of infectious syphilis; males and females, 1971–99. (B) Annual ratio of male to female new diagnoses of infectious syphilis at genitourinary medicine clinics in England 1971 to 1999.
GONORRHOEA
Before 1975 trends differed between the sexes but were similar after that. Male rates declined from 1975 to 1985, with an average annual decrease of 4.1/105 (fig 4) (p<0.001). From 1985 to 1988 rates declined significantly more steeply compared with 1982 to 1985 (p=0.001) and 1988 to 1991 (p<0.001) at an average of 28.3/105 annually, falling by 80.5/105 (fig 4). The rates changed little between 1988 and 1991 but then fell to 28/105 in 1995 after which they rose again, increasing to 43.7/105 in 1999. Rates in women followed a similar pattern (fig 4) rising between 1971 and 1975, declining slowly at 2.07/105 annually between 1975 and 1985, and showing a steeper decline between 1985 and 1999 with the rate of decline in that period being significantly steeper, compared with 1982 to 1985 (p=0.001) and 1988 to 1991 (p=0.002). There was a fall of 43.2/105 between 1985 and 1988. After falling from 27.9/105 in 1988 to 12.9/105 in 1994, female rates started increasing again in 1995, rising to 19.6/105 in 1999.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual rates of attendances at genitourinary clinics in England with new diagnoses of gonorrhoea; males and females 1971 to 1999.
GENITAL HERPES (FIG W2 ON sti website)
Over the whole period, the annual new diagnoses increased more than sevenfold from 3671 to 29 221 (fig w2 on STI website). Rates quadrupled for males (a total increase of 37.5/105) and increased 17-fold (64.3/105) for females. Rates increased steadily between 1971 and 1981 but steepened between 1981 and 1984 (fig w2). Rates declined between 1986 and 1988, falling by 5.8/105 for males and 3.5/105 for females. After 1988 rates resumed their upward courses; and after 1991, female rates increased more steeply, exceeding male rates. In men the rate changed little after 1992 but for women the rate continued to increase. Rates stopped increasing between 1996 and 1999 in females (fig w2).
GENITAL WARTS
Over the whole period, the annual numbers of new diagnoses increased eightfold from 13 730 to 113 528 (fig w3 on STI website). Rates followed similar trends for males and females (fig w3). From 1971 to 1982 they rose slowly in both sexes, then the rate of increase steepened between 1982 and 1987. For males the average annual rise between 1982 and 1987 was 21.1/105 but the male rates did not change significantly (p=0.252) between 1987 and 1991. For females there was an average annual increase of 14.9/105 between 1982 and 1987, followed by a significantly shallower (p=0.001) rise of 3.7/105 annually between 1987 and 1991. After a small decline in 1995 rates rose again from 1995 to 1999 increasing annually by 11.6/105 and 8.0/105 in males and females respectively. The upward trends after 1995 were significant for males (p = 0.02) and for females (p = 0.014).
Discussion
The data presented are consistent with the theory that sexual health components of the UK's AIDS campaigns of 1986–7 influenced sexual behaviour in the general population. The temporal associations of the campaigns and substantial rises in new attendances at GUM clinics not requiring treatment (also reflected by increases in HIV testing12), and falls in all treated cases, gonorrhoea, and genital herpes are very unlikely to be coincidental. The delayed slowing of previously rising rates of genital warts in 1987 is consistent with that disease's longer incubation period. The bacterial infections, syphilis, and gonorrhoea had begun declining in the 1970s (figs 3A and 4) and the reasons for this are unknown. However, the decline in the period 1996–7 was significantly steeper and also affected herpes and warts. There were also significant increases in condom sales and use at that time.12 Whatever they achieved in preventing HIV transmission, the general population campaigns were associated with reduced transmission of other STIs, seemingly through behaviour change and heightened awareness of risky sexual practices.
The fall in HIV transmission among homosexual and bisexual men (MSMs) in 1983–4 (fig 1) coincided with the AIDS awareness and informal AIDS campaigns conducted by the gay community. However, could that decline be because most men at highest behavioural risk had been infected with HIV by that date? The 6000 men estimated to have been infected before 1984 represented only 6% of MSMs attending GUM clinics in England, a fraction of the MSM population at higher behavioural risk.14 Therefore an “exhaustion of the susceptibles” is unlikely. The simultaneous fall in the incidence of male infectious syphilis (fig 3), and contemporary reports of changes in gay male behaviour around 1983–4,3, 15, 16 make it more plausible that the growing gay male awareness and AIDS campaigns caused falls in transmission of both HIV and syphilis among MSMs through changing behaviour. The decline in ulcerative syphilis may also have accelerated the reduction in HIV transmission.17
Whether the sexual health campaigns of 1983–7, and initiatives against drug injecting,8 protected the United Kingdom from the impact of HIV experienced by many other Western European countries (where the population prevalence of HIV is up to six times higher than in the United Kingdom6) is more arguable. However, early interventions against HIV emerging in a country are considered to be most effective.18 It is striking that among Western European countries only Sweden, Norway, and Finland (countries which also mounted vigorous public health campaigns against HIV early relative to their local epidemics4) have HIV prevalences below that of the United Kingdom.6 This is despite a particular overlay in the United Kingdom of HIV from African countries.19 Therefore it is probable that an early vigorous approach to AIDS blunted the penetration of HIV in the United Kingdom.
The improving trends in gay sexual health indices in the mid-1980s were not sustained. High levels of risk taking behaviour were recorded in gay and bisexual men in the early 1990s.20, 21 The evidence of recent, ongoing HIV transmission among MSMs, and increasing STI diagnoses in the general population is especially disquieting.9 There is little evidence from these data of any positive impact of the 1995 strategy.9, 11 “Risk profiles,” and other HIV reporting data for homosexual and bisexual men show results consistent with ongoing HIV transmissions and continuing or even rising levels of risk taking.22, 23 Specifically since 1995 gonorrhoea diagnoses have increased significantly,9, 24 several outbreaks of syphilis have occurred25, 26 and behavioural monitoring suggests increasing behavioural risk among MSMs.27 There has been a rise in rectal gonorrhoea so that the rise in gonorrhoea in gay men is unlikely to be the result of adoption or safe sex practices.19
The recent general increases in STI diagnoses are likely to be genuine. There were changes in reporting practices and codes in 1995 but these were minor compared with those in 1988, which occurred without appreciable effect on trends.9 Responsibility for the collection of clinic returns was transferred to CDSC in 1995.9 However, the upward trends have been sustained for over 4 years9, 24 and are unlikely to be explicable by minor alterations in coding or collection practices, which would mostly affect a single year. Nevertheless, it should be emphasised that the rises in attendances requiring treatment do not necessarily indicate increased incidence of all STIs. Increasing ability to diagnose chlamydia, greater healthcare seeking behaviour, or improved clinic services explain some of the rises.9 However, rates of gonorrhoea, short term trends in which are considered a sensitive indicator of sexual behaviour, have increased by over 30% since 1994.9, 24 They cannot be explained by new diagnostic molecular techniques which are not yet in widespread use. This rise, in combination with the trends in STIs and behaviours among MSMs,23, 25, 26 makes it likely that the impact of the HIV/AIDS campaigns of the 1980s has worn off. New generations becoming sexually active since then are likely to be less aware of the dangers of HIV and it seems likely that there has recently been an increase in risky sexual behaviour.8
In conclusion, the results of this analysis show that almost certainly the AIDS awareness and campaigns among gay men had a major impact, reducing HIV transmission in England in the early 1980s, and that the later general population campaigns reduced the transmission of other STIs among heterosexuals, probably also reducing the penetration of HIV into the population. The more recent sustained HIV transmission among gay men and increasing transmission of gonorrhoea and syphilis among all gay men and heterosexuals indicate that the forthcoming sexual health strategy for England, in particular its HIV/AIDS and STI components, will have to be comprehensive and vigorous.28, 29
Key messages
-
AIDS awareness and campaigns to reduce HIV transmission in England in the early and mid-1980s had major impacts in reducing indigenous homosexual transmission of HIV and heterosexual transmission of other STIs, in the general population.
-
The success of the early campaigns probably also explains why overall prevalence of HIV in the United Kingdom is lower than most other Western European countries.
-
There is however evidence of substantial ongoing transmission of HIV among homosexual and bisexual men in the 1990s.
-
Attendances at genitourinary medicine clinics with sexually transmitted diseases have increased substantially since 1995.
-
These data strongly support the need for vigorous new sexual health and HIV/AIDS strategies.
Acknowledgments
This analysis is entirely reliant on primary STI data supplied by genitourinary medicine clinics and HIV data were from voluntary confidential reporting by clinicians, microbiologists, and others to CDSC. The authors would also like to thank Michael Bland for producing visual presentations of these data and Angela McHenry and Pauline Deeks for management of the HIV and STI data. Virginia Berridge, Janet Mortimer, and Donald Acheson provided helpful advice and comments on earlier drafts of this paper.
Contributors: AN designed the analysis and wrote the paper; MD gathered the primary information on the HIV/AIDS campaigns and made early drafts of the paper while working as specialist registrar on placement at CDSC. All statistical analyses were undertaken by SL, apart from back calculation of HIV incidence, which was undertaken by DDeA with ONG. STI data were collated, compiled, and analysed under the directions of GH and MC; BE and ONG undertook this role for HIV data; GH, MC, BE, KF, and ONG helped with interpretation of the data and commented on the text. GH and KF contributed significantly to the writing of the paper. Angus Nicoll acts as guarantor of the paper.
Conflicting interests: There were no known conflicting interests of the authors and the costs of the study were met from core PHLS funding.
References
Supplementary materials
Web Figure 1: Annual rates of total new attendances at genitourinary medicine clinics in England, males and females 1971�99.
Web Figure 2: Annual rates of attendances at genitourinary clinics in England: with new diagnoses of genital herpes; males and females, 1971�99.
Web Figure 3: Annual rates of attendances at genitourinary clinics in England with new diagnoses of genital warts; males and females, 1971�99.
Web Table 2: Numbers and rates (per 100 000 total population) of attendances at genitourinary medicine clinics in England.
Web Table 3: Numbers and rates (per 100 000 total population) of attendances at genitourinary medicine clinics in England.
{kind=link}
{kind=link}
{kind=link}