Article Text

Abstract
Background/objectives: There has been a recent shift in the epidemiology of early syphilis in the developed world with sporadic outbreaks on a historic low level of background disease. Here we describe an ongoing outbreak of syphilis in Brighton.
Methods: Data collected on all patients with a diagnosis of early infectious syphilis at Brighton GUM clinic.
Results: 30 cases of early syphilis were diagnosed over a 25 month period beginning in July 1999. 28 were homosexual or bisexual men, giving a rate of 134 cases per 100 000 homosexual men. The cases reported a median of three sexual contacts (range 1–50) in the preceding 6 months and 77% had concurrent regular and casual partners. 83% of contacts were casual and untraceable. Over one third (11) of these cases reported oral sex as their only risk factor for syphilis acquisition and were unaware of this transmission route. 70% were diagnosed with primary or secondary infection, the remaining 30% being asymptomatic with early latent infection. Eight of the cases were HIV positive and a further eight remain untested for HIV. At least one concurrent STI was found in 40% of cases. Regular outbreak control meetings, involving relevant healthcare professionals, were held to plan appropriate interventions.
Conclusion: The high rate of casual and untraceable contacts in this outbreak suggest that alternative control measures are necessary, including on-site testing and further health education regarding the oral transmission of syphilis. Continued vigilance for syphilis is essential, especially in those patients who are HIV positive.
- syphilis
- homosexual men
Statistics from Altmetric.com
Introduction
Over recent years the epidemiology of syphilis in developed countries has been characterised by sporadic outbreaks on an otherwise low level of background disease. In the United States, within these outbreaks, there has been a high rate of disease among homosexual men of whom up to 72% are co-infected with HIV.1 The Centers for Disease Control and Prevention responded by publishing the US National Plan in 1999 to eliminate syphilis, with the goal of complete eradication by 2005.2 In the United Kingdom, the PHLS is currently developing outbreak control guidelines3 in response to an increasing number of outbreaks over the past 4 years affecting both heterosexual4–6 and homosexual populations.7–9
Brighton and Hove is a cosmopolitan city on the south coast of the United Kingdom with a vibrant homosexual community of approximately 10 000.10 As a liberal seaside resort its population varies seasonally from 250 000 to approximately one million in the summer months. We describe an outbreak of syphilis in Brighton, which has been almost exclusively in homosexual men, with rates (134/100 000) comparable with those in the United States1 (200/100 000).
Description of cases
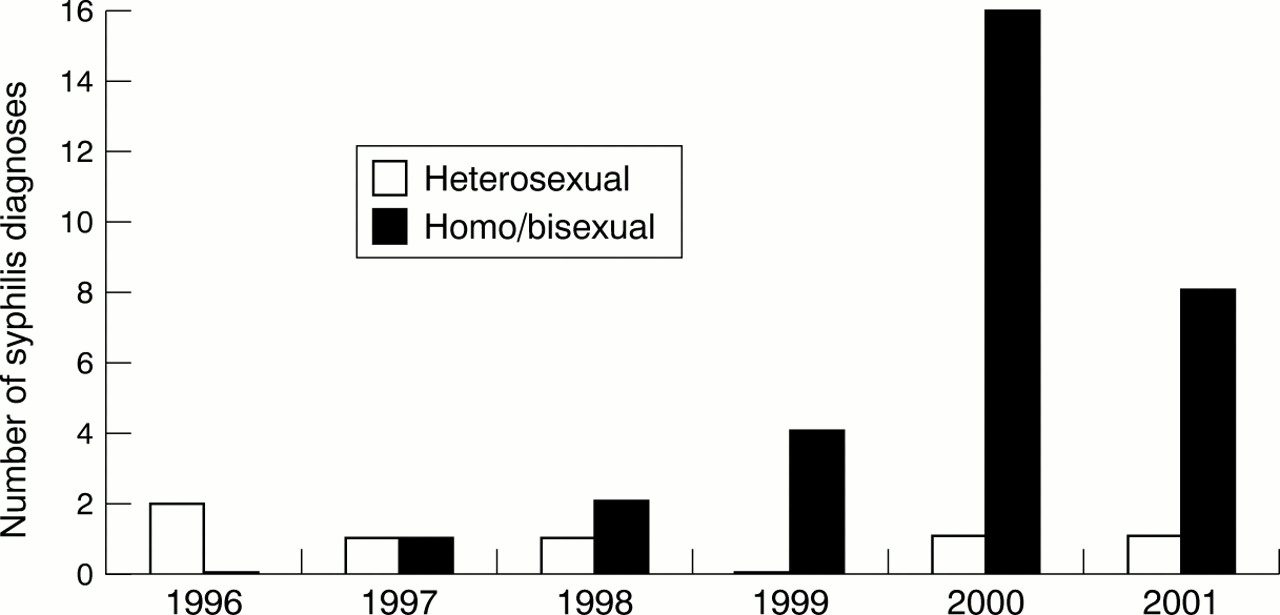
A total of 30 cases of early syphilis were diagnosed in Brighton between July 1999 and July 2001, a considerable increase compared with seven cases diagnosed in the previous 3 years (see fig 1). The median age of cases was 31.5 (range 23–48). Of these, 28 were homosexual or bisexual men, all of whom were white. One African woman with secondary syphilis and one white heterosexual man with early latent syphilis, almost certainly acquired the infection in South Africa and Thailand, respectively. Of those who had been tested for HIV 36% (8/22) were HIV-1 antibody positive.
{kind=link}
Early syphilis in Brighton, 1996–July 2001.
Ten cases (33%) presented with primary syphilis (six penile and four perianal ulcers), 11 (37%) with secondary syphilis (rash only three; uveitis two; condylomata lata one; rash and PUO one; headache and PUO one; rash, oral ulceration and lymphadenopathy one; non-specific symptoms two) and nine cases (30%) were diagnosed with early latent disease, based on serology only (all had negative serology in the past 12 months and/or evolving serology consistent with recent infection). Both cases with uveitis initially presented to the ophthalmology department and one with rash to the dermatology department.
Nine patients were diagnosed with a concurrent STI (three gonorrhoea; two genital warts; two chlamydia; one genital herpes; one hepatitis A) and three patients had two concurrent STIs (one gonorrhoea and chlamydia; one NSU and genital warts; one genital herpes and warts). Out of the 30 cases 13 (43%) had a previous history of STIs.
Sexual history
Twenty eight cases had casual partners (defined as a “one-off” known or unknown sexual contact) and of these 23 had concurrent regular partners. The remaining two cases had regular partners only. There was a median of three contacts per case. Thirteen cases had one casual partner, nine cases had between one and five casual partners, one case had 5–10 casual partners, and five cases had >10 casual partners (10–50).
Many of the cases did not perceive themselves to have been at risk, with 11 cases reporting oral sex as their only risk factor and only five of the cases reporting unprotected anal sex in the past 6 months.
Contact tracing
Cases cited a total of 206 contacts within the past 6 months. Of these 177 (86%) were casual partners. A total of 172 (83%) contacts were untraceable, either because they were anonymous partners or they had moved abroad. Of the 34 traceable contacts 19 (56%) were seen in the GUM department, of which five (26%) were diagnosed with early syphilis, three of whom were asymptomatic.
Interventions
In response to the increased number of syphilis cases, an outbreak control meeting was set up involving healthcare professionals from genitourinary medicine, public health, microbiology, and health promotion. The following approaches were implemented within the first year:
-
Letter sent to all general practitioners in the area by the health authority through established links
-
Help line set up at the GUM clinic
-
Additional homosexual men's health clinics, with extra staffing
-
GUM consultant briefed outreach workers from local voluntary sector organisations
-
Health promotion organised a prevention campaign, which included: an article and further advertising published in the local gay press, syphilis alert cards given out in condom packs at Brighton Gay Pride, and posters for the clinic and Brighton's annual gay festival.
Progress meetings were held on a regular basis. After 12 months, as the outbreak appeared to be continuing, a second meeting was held to discuss further interventions. These included creating a website for homosexual men encouraging sexual health screening and providing information on syphilis, educational events for local GPs and practice nurses, an update for outreach workers, a local radio broadcast, and preventive work with local gay bars and saunas. An application has now been submitted for funding of on-site testing in bars, saunas, and public sex venues. At the time of publication the outbreak is continuing and further methods to reduce transmission and improve contact tracing are under investigation using prospective methods of evaluation.
Discussion
We have described an ongoing outbreak of syphilis in Brighton with rates in homosexual men comparable with the high rates seen in recent outbreaks in the United States.1 Many individuals had a high rate of casual sexual partners with only 16% of contacts being traceable. The predominantly homosexual outbreaks in Dublin (17.5% of contacts traceable9) and Manchester (10% of contacts traceable7, 11) found similar difficulties. Attempts to control the outbreak have been hampered owing to obvious limitations with partner notification. An alternative approach would be to pursue on-site screening for syphilis in gay venues. In combination with effective health promotion healthcare workers in Dublin have found this both feasible and acceptable.9
The observation that 30% of the cases attending GUM services were asymptomatic highlights the importance of on-going screening in this setting. Just over one quarter (26%) of contacts attending the clinic were diagnosed with early syphilis highlighting not only the high infectious risk per sexual contact, but also the importance of effective partner notification when the contact is known. A high number of cases declined HIV testing. Of those who had tested a substantial proportion (36%) were positive. Given that there is evidence of increased HIV transmission with ulcerative STIs (HIV acquisition increased by up to eightfold and transmission increased by up to 11-fold12), it is essential that the sexual health needs of HIV positive patients are addressed. There were also a significant number of concurrent STIs (30%), emphasising the importance of screening for all STIs when patients attend GUM. In this outbreak 37% of cases admitted to oral sex as their only risk factor. This further highlights the need for health education regarding transmission routes.
The characteristics of this outbreak highlight the need for continued vigilance for syphilis in both GUM and non-GUM settings. By extending control efforts into the community we hope to limit the further spread of syphilis in Brighton in the coming months.
Acknowledgments
Contributors: DW, GD, MP, and PC identified the patients; MP, GD, and PC collected the patient data; MP and GD wrote the initial manuscript which was commented on and revised by all the co-authors; MF and AI instigated the initial outbreak programme; MF, DW, AI, and GD all participated (and continue to participate) in the ongoing outbreak management team.
Footnotes
-
Conflict of interests: none.