Article Text

Abstract
Objective: To evaluate sexual behaviour (including abstinence), sex partner change, and condom use during the 3 month period following treatment for Neisseria gonorrhoeae, Chlamydia trachomatis, Trichomonas vaginalis, or non-gonococcal urethritis.
Methods: 251 14–21 year old participants (83% female; 83% African-American) diagnosed with gonorrhoea, chlamydia, trichomonas, or non-gonococcal urethritis or sexual contacts of infected partners. Participants were clients of a public sexually transmitted diseases clinic or primary care adolescent clinics. Data were collected by structured interview at treatment, 1 month post-treatment, and 3 months post-treatment. At each visit, participants were asked about coital frequency and condom use for each recent partner. At 1 month, participants were asked when coitus occurred following treatment. At each follow up visit, sex partners were compared to partners named at treatment and classified as “same partner(s),” “new partner(s),” or both “same and new partner(s).”
Results: Post-treatment abstinence was reported by 26% and 19% for the 1 month and 3 month visits, respectively. Abstinence was associated with greater likelihood of infection at enrolment although abstainers reported fewer lifetime STI and fewer lifetime sex partners. A substantial proportion of participants reported additional sexual contact with a previous partner. The average proportion of condom protected coital events increased from about 45% at enrolment to 64% at 1 month and 58% at 3 months (p<0.05). Higher levels were sustained for the 3 months following treatment.
Conclusions: Many adolescents adopt, at least temporarily, risk reduction behaviours such as abstinence or increased condom use. Sexual re-exposure to potentially untreated previous partners may increase risk of subsequent reinfection.
- adolescents
- condom use
- sexual behaviour
Statistics from Altmetric.com
Treatment of common sexually transmitted infections (STI) such as gonorrhoea, chlamydia, and trichomonas is a central element of public health STI control efforts. From an individual’s perspective, treatment confirms susceptibility and translates STI risk into certainty. From a theoretical perspective, STI treatment is a salient occurrence likely to serve as an important “cue to action” for behaviours that could reduce risk of subsequent infection. A “cue to action” serves an important function in the initiation of health protective behaviours.1
The behavioural responses of adolescents to STI treatment are quite variable in form and efficacy. “Wishful thinking” is the most common response but adolescent girls with negative views about future STI acquisition use more positive coping strategies.2 The value and importance of sex itself may be questioned and accompanied by a period of sexual abstinence.3 An STI diagnosis raises questions about the source of infection (“Who gave me this STI?”), transmission (“Did I give an STI to someone else?”), as well as consideration of the implications of these questions for current and future relationships (“Has my partner been unfaithful?”). Some sexual relationships are discontinued because of violation of trust by a partner or because the partner becomes perceived as risky. Communication with the partner about the infection increases likelihood of partner treatment although several studies show that client initiated partner notification only occurs in 30%–60% of cases.4–6
A more detailed understanding of adolescents’ responses to STI treatment could inform improved interventions to prevent subsequent STI. Such interventions are important since up to 40% of adolescents with an initial STI have a second infection within a few months.7,8 The purpose of this paper, therefore, is to describe the sexual and condom use behaviours of adolescents during a period of up to 3 months following treatment for curable STIs.
METHODS
This study is part of a larger project evaluating factors associated with repeated bacterial and protozoan STI.7,8 Participants were ages 14–21 attending a metropolitan STI clinic or one of three community adolescent health clinics and were eligible for entry if they were treated for Neisseria gonorrhoeae, Chlamydia trachomatis, Trichomonas vaginalis, non-gonococcal urethritis (NGU), or were sexual contacts of these infections. Participant recruitment began in 1995 and was completed in 1999. Appropriate single dose treatment was provided for each subject, along with provision of condoms and counselling to advise sex partners of the need for testing and treatment. Each subject provided written informed consent but the requirement for parental consent was waived. The study was approved by the institutional review board of Indiana University/Purdue University at Indianapolis.
Data were collected at three time points using a structured interview administered by trained research assistants. A baseline interview was conducted at study enrolment. Each of the four most recent partners during the previous 2 months was identified by initials or first name. Participants responded to subsequent items about sexual and condom use behaviours with each partner. The baseline interview required 20–25 minutes for completion.
The follow up interviews were conducted approximately 1 month and 3 months after the baseline interview. At the 1 month interview, the initials or first name of each of the four partners identified during the baseline interview were confirmed. A series of questions inquired about interim behaviours with each partner. These questions addressed resumption of sexual activity, condom use, and sex partner communication. Additional items addressed interim sexual activity with new partners not identified during the baseline interview.
The 3 month interview identified up to four sex partners from the previous 2 months (that is, since the 1 month interview). Coital frequency and condom use were assessed for each partner. New partners were defined as those not identified at either the baseline or 1 month interview.
Measures
At each visit, participants were asked to identify sex partners by first name or initial. Coital frequency was assessed by asking “How many times in the past 2 months [“one month” was used at the 1 month visit] did you have sex with [insert partner’s name or initials]?” Responses were recorded verbatim. Participants with responses such as “don’t know,” “lots,” or “too many” were asked for an approximate number, and “missing” was entered when a precise estimate was not provided. Abstinence was defined as a report of no coital events during the interval in question. Condom use was assessed by a subsequent item: “Of the times you had sex with [insert partner’s name or initials], how many times was a condom used?” Condom use was subsequently defined as the proportion of condom protected events with a specific partner. Established partners were defined as any partner identified at baseline and subsequently at a 1 month or 3 month visit. New partners-1 month were defined as partners named at the 1 month interview but not in the baseline interview. New partners-3 months were defined as partners named at the 3 month interview but not at the baseline or 1 month interview. Participants were then categorised as “established partners only,” “new partners only,” or “both established and new partners” based on their partnerships during the follow up interval.
Behaviour change associated with STI treatment was assessed by comparison of coital frequency and condom use reported at 1 month and 3 months post-treatment with baseline reports.
Statistical analyses
Summary statistics are presented as frequency and percentage for categorical variables and as mean (SD) for continuous variables. The median and range is presented if the distribution of a continuous variable was skewed. Pearson’s χ2 test was used to compare categorical variables between analysis groups and either Student’s t test or Wilcoxon’s rank sum test was used for continuous variables. Appropriate 95% confidence intervals (CI) were calculated for parameter estimates. A paired Student’s t test or Bhapkar’s test for marginal homogeneity was used to compare outcomes between the 1 month and 3 month visits. The average percentage condom use at the 1 month and 3 month follow up visits was modelled using a repeated measures analysis of variance model. Time invariant characteristics included in the model were sex, race, STI infection status, and percentage condom use. Time varying characteristics in the model were coital frequency, partner status, and an indicator for the 3 month visit. Generalised estimating equations (GEE) were used to adjust parameter estimates for participants with multiple partners during a given measurement interval. The statistical software sas version 8.1 (SAS institute, Cary, NC, USA) was used for all analyses. Statistical significance was defined at the α = 0.05 level.
RESULTS
Of the 444 participants enrolled into the study, 251 (56.5%) returned for both a 1 month and 3 month visit. Of the 193 that did not return for both visits, 89 were lost to follow up after enrolment and 104 returned for at least one subsequent visit. Subsequent analyses are limited to participants completing both follow up visits in order to focus on the entire 3 month period following STI treatment. Included participants were younger, more likely to be female, were more likely to enrol from an adolescent clinic, and were more likely to have an STI at enrolment but there were no differences in race, history of STI, lifetime partners, recent abstinence, or condom use (table 1).
Enrolment characteristics, by follow up status
Abstinence was relatively common in the period before each follow up visit. At treatment, 25 participants (10.0%) reported no sexual activity in the previous 2 months, while at the 1 month and 3 month visits 64 (25.5%) and 47 (18.7%), respectively, reported no interval sexual activity (data not shown). In total, 86 (34.3%) participants reported no sexual encounters in the period before at least one of the two follow up visits. Participants reporting any period of post-treatment abstinence were younger, more likely to be female, more likely to be black, and more likely to enrol from adolescent clinics (table 2). Post-treatment abstinence was also associated with greater likelihood of infection at enrolment although abstainers reported fewer lifetime STI and fewer lifetime sex partners. Among non-abstaining participants, the median interval until first post-treatment coitus was 8 days (range 0–48; data not shown).
Enrolment characteristics of participants with any post-treatment abstinence period*†
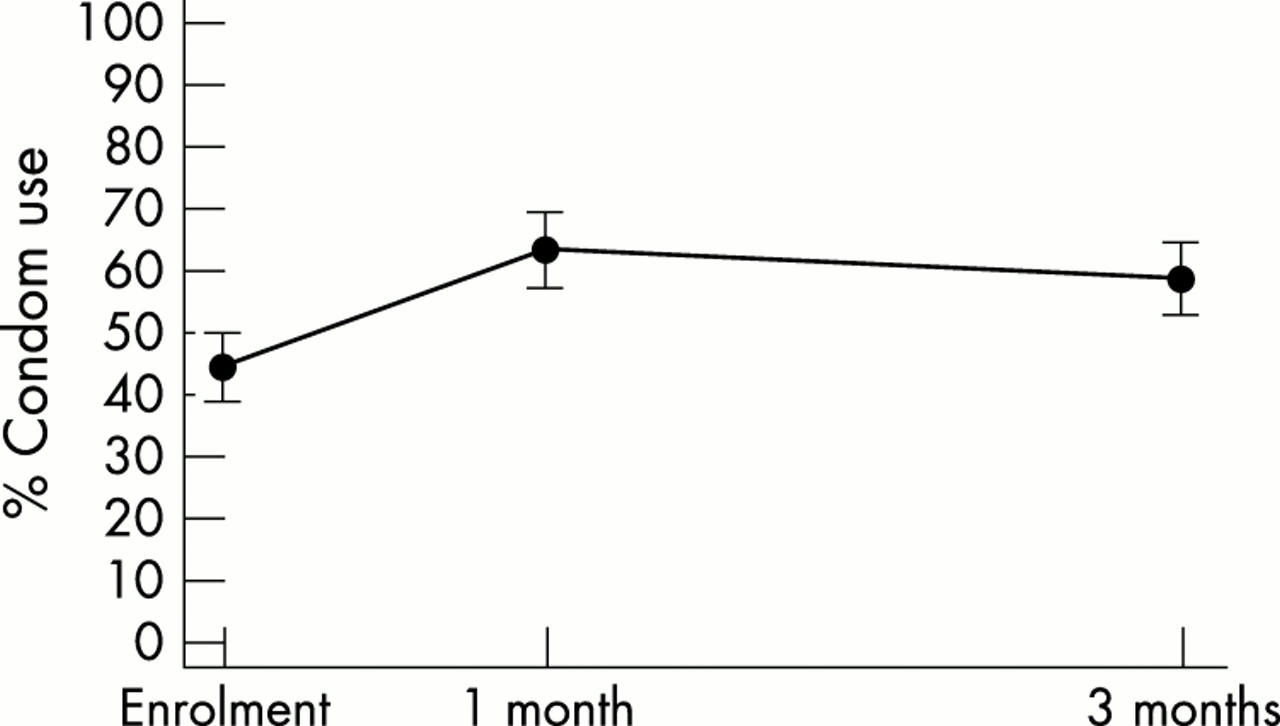
Levels of condom use and their 95% confidence intervals at each visit are shown in figure 1. Overall, the average proportion of condom protected coital events increased from about 45% at enrolment to 64% at 1 month, and 58% at 3 months. Significant increases in condom use (compared to enrolment levels) were seen at both 1 month and 3 month visits as indicated by non-overlapping confidence intervals.
{kind=link}
Change in proportion of condom protected coital events from 2 months before STI treatment (Enrolment), 1 month, and 3 months post-treatment. Note: Vertical bars represent 95% confidence intervals.
Post-treatment partner status and change in condom use are shown in table 3. As noted above, about 25% of participants abstained between the enrolment and 1 month visit. Most participants who resumed sexual activity reported only established partners (44.6%) during the 1 month interval following treatment. Smaller proportions reported contact with both established and new partners (n = 23; 9.2%) and about 21% reported new partners only. Average condom use increased by 21% between enrolment and the 1 month follow up.
Comparison of partner status and change in condom use in two post-treatment intervals
Between the 1 month and 3 month follow up visits, about 19% reported abstinence (although a few of these participants had sex during the 1 month interval following treatment) (see table 3). About 40% of participants reported only established partners during each of the two intervals following treatment. A larger proportion of participants reported only new partners at the 3 month follow up than at the 1 month follow up. Average condom use decreased by 7% between the 1 month visit and the 3 month follow up (p<0.05 by paired t test). Thus, the proportion of condom protected coital events initially increases after STI treatment and then declines towards baseline levels within 3 months but remains above initial levels.
Repeated measures analysis of variance (adjusted for multiple partners within person by GEE) was used to model mean condom use at 1 month and 3 months post-treatment. Covariates included sex (female/male), race (black/non-black), infection status at enrolment (yes/no), interval coital frequency, and the status of partners over the previous interval (established/new partners/established only and new partners only/established only). As shown in table 4, increased condom use during the 3 months following STI treatment was associated with lower levels of interval coital frequency (β = −1.5; 95% confidence interval −1.8 to −1.1) and higher levels of condom use at enrolment (β = 0.3; 95% confidence interval 0.2 to 0.4). Sex, race, and partner status were not independently associated with average level of post-treatment condom use. Statistical non-significance of the indicator for the 3 month visit shows that condom use did not decrease significantly over the 3 month post-treatment follow up period.
Predictors of post-treatment condom use*
DISCUSSION
STI treatment was followed by abstinence for a substantial proportion of adolescents. The median time to resumption of coital activity was about a week after treatment, perhaps reflecting adherence to treatment guidelines that advise abstinence after STI treatment.9 More than half of participants had additional coital exposures to a partner established before the time of treatment, suggesting that partner treatment remains an important element of prevention of reinfections. Among those with continued coital activity, condom use increased markedly, especially during the first month after treatment. STI treatment was clearly associated with attempts to reduce subsequent risk although these attempts appear to decline over time.
Some studies of adults show that risk reduction behaviours increase following STI diagnosis.10,11 Data from the 1991 National Survey of Men showed that about one third of adult men do not modify sexual behaviour or condom use following an STI.12 Data from the French national survey of sexual behaviour showed that women modified behaviour following an STI but men did not.11 We found that women were more likely to report post-treatment abstinence than men, but did not find evidence of sex effects on post-treatment condom use.
Our data are unique in that infection status and antecedent behaviours were determined prospectively. Use of a relatively short follow up interval may allow more accurate self report of resumption of sexual activity and other sexual behaviours after STI treatment. Diary records or other event signalling techniques could add additional precision although the importance of such precision is unclear. Longer periods of follow up could enhance understanding of the longer term influence of STI treatment on risk behaviours. However, maintenance of cohorts of at-risk adolescents is difficult and expensive. More importantly, factors associated with post-treatment risk behaviours may also be associated with cohort attrition. Subsequent research could also benefit from increased attention to potential sex differences in adolescents’ post-treatment behaviours. The sample of males in the current study was too small to conduct reliable sex comparisons.
The findings of this research suggest several strategies that could be adopted to encourage maintenance of protective post-treatment behaviour change. These include recognition of the prevalence of continued exposure to established partners. Provision of single dose medications for delivery to partners may reduce the incidence of subsequent infections and is well accepted by patients.13 Routine post-treatment follow up visits—perhaps 3 or 4 months after treatment—to allow STI rescreening and counselling specifically designed to reduce behavioural relapse. Post-treatment rescreening is suggested in the 2002 STI treatment guidelines compiled by the US Centers for Disease Control and Prevention.14 Additional research is needed to determine the acceptability among adolescents of such screening practices as well as influence on subsequent infection.
Acknowledgments
Sponsored in part by the National Institute of Allergy and Infectious Diseases (U19 AI31494) and the Maternal Child Health Bureau (MCJ 18965). The authors thank Patricia Brooks and Cathy Roberts for data collection. Portions of these data were presented at the International Society for Sexually Transmitted Diseases Research, Seville Spain, 19 October 1997.
CONTRIBUTORS JDF, study design, data collection, data analysis, and manuscript preparation; EJB, data analysis and manuscript preparation; BPK, study design, data analysis, and manuscript preparation; DPO, study design, data collection, and manuscript preparation.
REFERENCES
Linked Articles
- Brief Encounters