Article Text

Abstract
Objectives: To determine the aetiology of genital ulcer disease (GUD) and its association with HIV infection in the mining community of Carletonville, South Africa, from two cross sectional surveys of consecutive men presenting with genital lesions during October 1993 to January 1994 and July to November 1998.
Methods: A multiplex polymerase chain reaction (M-PCR) assay combined with amplicon detection was used to identify DNA specific sequences of Treponema pallidum, herpes simplex virus (HSV), and Haemophilus ducreyi. A real time PCR assay was used to differentiate between HSV-1 and HSV-2.
Results: M-PCR detected T pallidum, HSV, and H ducreyi in 10.3%, 17.2%, and 69.4% of 232 GUD patients during 1993–4 and in 12.4%, 36.0%, and 50.5% of 186 GUD patients in 1998. The proportion of patients with more than one agent increased significantly from 7.3% (17/232) in 1993–4 to 16.7% (31/186) in 1998 (p <0.01). HSV-2 was detected in a higher proportion of ulcer specimens from HIV infected patients than in specimens from HIV uninfected patients during both time periods (1993–4: 26.2% v 6.7%, p <0.001; 1998: 42.1% v 29.6%, p >0.09).
Conclusions: Based on two cross sectional surveys, 4 years apart, chancroid remained the leading cause of GUD in men who presented at the STD clinic with genital ulcers in the mining community of Carletonville, South Africa. The relative prevalence of primary syphilis has remained low. However, HSV-2 has emerged as a more significant cause of GUD and the proportion of GUD patients infected with more than one agent also increased significantly. HSV-2 DNA was detected in a significantly higher proportion of ulcer specimens from HIV positive patients than from HIV negative patients. No association was found between HIV infection status and the relative prevalence of chancroid or syphilis.
- genital ulcer disease
- herpes simplex virus
- HIV
- polymerase chain reaction
Statistics from Altmetric.com
Sub-Saharan Africa remains the region of the world most severely affected by the HIV epidemic where the transmission of human immunodeficiency virus type 1 (HIV-1) is predominantly through heterosexual contact.1–3 One theory to explain this extensive heterosexual spread of HIV-1 in these regions is the presence of sexually transmitted diseases (STDs), especially genital ulcer disease (GUD), which is known to facilitate the transmission of HIV.4–7 The estimated annual global incidence of GUD exceeds 20 million cases.8 In African countries worst affected by HIV infection, the proportion of men and women with STD who had genital ulcers is in the range of 45%–68% and 13%–68%, respectively.9 The most common aetiological agents of GUD are Treponema pallidum, Haemophilus ducreyi, herpes simplex virus type 2 (HSV-2), and HSV-1.
In developing countries, chancroid has often been documented as the most common cause of GUD, whereas in Europe and North America, genital herpes is the leading cause of GUD. Numerous epidemiological studies conducted in South Africa in the 1980s indicate that chancroid and syphilis were major causes of GUD, representing 70%–90% of cases of GUD,10 while genital herpes accounted for only a relatively small proportion (3.3%–10%). However, many areas in Africa have shown increasing prevalence of genital herpes during the 1990s.11
Despite a strong association between GUD and HIV infection,12–14 the aetiology of GUD can vary both geographically and temporally as well as vary in its association with HIV infection.15–17 The objective of this study was to determine the aetiology, the relative prevalence rate, and the association of specific agents of GUD with HIV infection in men with genital lesions attending an STD clinic in the mining community of Carletonville, South Africa, from two cross sectional surveys conducted during October 1993 to January 1994 and July to November 1998.
METHODS
Study population
Genital ulcer and serum specimens were obtained from a total of 418 male patients with GUD attending the same STD clinic in Carletonville. Specimens were obtained from 232 consecutive patients in October 1993 to January 1994 and from 186 male patients in July to November 1998. The patients entered in the study had not received antibiotics during the previous 4 weeks. Swab specimens were taken directly from ulcers of >2 mm in size. Written informed consent was obtained from all patients enrolled, and guidelines of the Department of Health, South Africa, were followed in the conduct of this study.
Specimen collection
After thorough cleansing of each lesion with a gauze pad, specimens were collected from the base of each ulcer for detection of T pallidum, H ducreyi, and HSV specific DNA sequences by using a multiplex polymerase chain reaction (M-PCR) assay that was performed at the Centers for Disease Control and Prevention (CDC), Atlanta, GA, USA. When multiple ulcers were present, the specimen was collected from the largest. The swab was put into a sterile tube and shipped on dry ice to CDC, where the dry swab was placed in 0.5 ml of Amplicor specimen transport medium (Roche Diagnostic Systems, Branchburg, NJ, USA), agitated, and then discarded. The specimen was aliquoted and stored frozen at − 70°C until analysed.
Serological testing for syphilis and HIV-1
Serum specimens, obtained by venepuncture, were tested by the quantitative rapid plasma reagin test (RPR; Omega Diagnostics, Alloa, UK) and the fluorescent treponemal antibody absorption test (FTA-ABS; Murex, Dartford, UK). HIV serology was performed by enzyme linked immunosorbent assay (ELISA; Abbott Laboratories, Abbott Park, IL, USA), with low positive results confirmed by western blot assays (HIV blot 2.2; Diagnostic Biotechnology, Singapore) and high positive results confirmed by a direct fluorescent antibody test (Serofluor; Virion, Ruschlikon, Switzerland).
M-PCR amplification
DNA from each ulcer specimen was extracted in the presence of carrier DNA (calf thymus DNA, Sigma Chem Co, St Louis, MO, USA) using a DNA mini kit from Qiagen (Valencia, CA, USA). No internal control DNA was incorporated into the M-PCR assay. A “mock” clinical specimen consisting of buffer was included in every set of DNA extractions. Precautions were used to prevent carryover contamination. The M-PCR amplification conditions were identical to those previously described15 except that various 5′-fluorescein labelled primers were used instead of 5′-biotinylated oligonucleotides: TET (tetrachloro-6-carboxy-fluorescein) was used to label the forward primer for HSV, FAM (6-carboxy-fluorescein) on the reverse primer for H ducreyi, and HEX (hexachloro-6-carboxy-fluorescein) on the reverse primer for T pallidum. Amplification was performed in a thermal cycler (Perkin-Elmer PCR System 9600 or 9700). All primers were synthesised by the Biotechnology Core Facility at CDC, Atlanta, GA, USA.
Detection of PCR products
An ABI Prism 310 genetic analyser (Applied Biosystems, Foster City, CA, USA) was used to detect the amplicons based on their specific fluorescent tags and sizes. After amplification, 1 μl of the reaction mixture was added to 15 μl of a solution (ratio 19:1) of formamide (Life Technologies, Gaithersburg, MD, USA) and GeneScan-500 (Applied Biosystems) for fragment analysis. GeneScan-500 consists of TAMRA (6-carboxy-tetramethyl-rhodamine) labelled size standards varying from 100–500 bp. The sample mixture was heated at 95°C for 3 minutes and cooled on ice before being injected into a 47 cm capillary filled with gel mixture (POP4, Applied Biosystems). The capillary run was performed at 15 kV, 9 mA, and at 60°C for 20 minutes for each sample. The specific size of each amplicon was determined using the labelled standards and the GeneScan. The expected sizes of the amplicons for T pallidum, HSV, and H ducreyi were 260 bp, 431 bp, and 439 bp, respectively.
Real time PCR and HSV typing
Typing of HSV was performed by real time PCR using the Smart Cycler (Cepheid, Sunnyvale, CA, USA). For each reaction, real time fluorescence values were measured during amplification as a function of the quantity of a reporter dye released from a dually labelled fluorogenic probe oligonucleotide (TaqMan probe) by the 5′ to 3′ exonuclease activity of Taq DNA polymerase. A threshold cycle value for each sample was determined as the number of the first cycle at which the measured fluorescence exceeds the threshold limit. M-PCR amplifications were performed in 25μl reaction vials (Cepheid) using 10μl of sample DNA. A final concentration of 1X PCR Gold buffer (Applied Biosystems); 5 mM MgCl2; 200 μM each of dATP, dGTP, dCTP, and dUTP; 250 nM of primers; and 100 nM of TaqMan probes were used. Three units of AmpliTaq Gold DNA polymerase (Applied Biosystems) and 0.5 units of uracil-N-glycosylase (UNG, Applied Biosystems) were used per 25μl reaction. The specific target sequences of TaqMan probes and primers for HSV-1 and HSV-2 were chosen from the dissimilar regions in the glycoprotein G region and are shown in table 1. Amplification was performed using the following parameters: 50°C for 2 minutes to allow UNG inactivation of any carryover product, 95°C for 10 minutes to inactivate UNG and to activate AmpliTaq Gold DNA polymerase, and 45 cycles at 95°C for 15 seconds and 60°C for 60 seconds. Positive control templates using purified genomic DNA from strains HSV-1(F) and HSV-2(G) were kindly provided by Felicia Stamey of the Herpes Virus Branch, Division of Viral and Rickettsial Diseases, CDC. To validate this typing assay, lymphocyte cell lysates prepared from 18 previously characterised clinical isolates (11 HSV-1 and seven HSV-2) and two additional laboratory HSV-1 strains provided by the Herpes Research Branch, CDC, were assayed blindly. The real time M-PCR typing results obtained from the Smart Cycler were 100% concordant with the previous typing results using culture and indirect immunofluorescence testing (data not shown).
TaqMan probes and primers for HSV typing
Statistical analysis
Demographics, clinical data, and results of laboratory tests were abstracted onto a standardised form and analysed using epi-info, Version 6.04b (CDC, Atlanta, GA, USA).
RESULTS
Study population characteristics
A total of 418 GUD patients (232 from 1993–94 and 186 from 1998) were enrolled in this study. All patients were African men. The mean ages were 31.9 years (range 20–58 years) and 32.8 years (range 20–55 years) for 1993–4 and 1998, respectively. The HIV seroprevalence rate was similar for the study periods: 54.3% (126/232) in 1993–4 and 58.8% (107/182) in 1998 (p >0.4). Among HIV seropositive patients, 73.6% (92/125) in 1993–4 and 67.6% (71/105) in 1998 were between the ages of 25 and 39 years. The overall FTA-ABS seropositivity rate was 44% (165/375), with no significant difference between 1993–4 (47.5%) and 1998 (39.9%). The RPR seropositivity rate was 19% (44/232) in 1993–4 compared with 12% (22/183) in 1998 (p >0.07).
Aetiology of GUD
The aetiology of GUD was determined by M-PCR followed by fragment analysis of amplicons using the ABI 310 genetic analyser. Representative M-PCR test results using genomic DNA prepared from each organism are shown in figure 1. The specific amplicons of T pallidum, HSV, and H ducreyi were 255 bp, 423 bp, and 431 bp, respectively, and are represented as coloured peaks on the ABI 310 graph. Owing to the different fluorescent labelled primers used for the amplification of each target, peaks indicative of each amplification product can be differentiated. Size standards are labelled with an asterisk in figure 1A. Non-specific amplification products, most likely the result of the impurity of templates and the frequent use of the capillary, could be observed in some runs; however, the size(s) and the signal strengths of non-specific products did not correspond to those of the expected amplicons. The detection limit of the ABI 310 for each target was approximately 10 genomic copies (data not shown).

Fragment analysis of M-PCR amplicons by ABI 310. (A)–(E) Show representative results of M-PCR amplification products using a combination of 1000–1500 copies of genomic DNA from T pallidum (TP), H ducreyi (HD), and HSV. (A) TP DNA alone; (B) TP and HD; (C) TP and HSV; (D) HD and HSV; (E) TP, HD, and HSV. Internal size standards are labelled with an asterisk. The x axis shows amplicon size in base pairs; the y axis shows relative fluorescence.
The aetiology of GUD determined in the two cross sectional surveys is shown in table 2. DNA from T pallidum, HSV, and H ducreyi was detected in 10.3%, 17.2%, and 69.4% of the 232 patients during 1993–4 and in 12.4%, 36.0%, and 50.5% of the 186 patients in 1998, respectively. Overall, chancroid remained the leading cause of GUD in this population in both studies; however, the proportion of GUD patients with chancroid infection declined by approximately 20% in 1998. This decline was mainly a result of the decrease in the number of patients with single H ducreyi infections (62.9% in 1993–4 v 36.0% in 1998, p <0.0001). In contrast, the relative prevalence of genital herpes infection increased significantly in 1998 (17.2% v 36.0%, p <0.0001). An increase was observed in both single HSV infections (12.1% v 21.0%, p <0.02) and in cases where HSV was found in combination with other aetiological agents (5.2% v 15.1%, p <0.002). Overall, the proportion of GUD patients with more than one aetiological agent increased significantly from 7.3% in 1993–4 to 16.7% in 1998 (p <0.01), with co-infection with H ducreyi and HSV being the most common (6.5%). Syphilis was the least common cause of GUD, and its relative prevalence did not change significantly when comparing the two cross sectional surveys (10.3% v 12.4%).
Aetiology of GUD by M-PCR
Relation between GUD aetiology and HIV infection
HSV DNA was detected by M-PCR in a higher proportion of ulcer specimens from HIV positive patients than from HIV negative patients during both cross sectional studies (1993–4: 26.2% v 6.7%, p <0.001; 1998: 42.1% v 29.6%, p >0.09), whereas T pallidum and H ducreyi DNA were detected less frequently in ulcer specimens from HIV seropositive patients than from HIV seronegative patients (T pallidum: 8.7% v 12.3% in 1993–4, 11.2% v 14.7% in 1998; H ducreyi: 64.3% v 75.5% in 1993–4, 46.7% v 57.3% in 1998) (table 3). The higher proportion of cases where HSV-2 DNA was detected from HIV positive patients in 1998 did not achieve statistical significance (p <0.1); nevertheless, single infections of HSV alone were significantly more prevalent in GUD patients infected with HIV than in patients not infected with HIV in both series (1993–4: 20.6% v 1.9%; 1998: 28.0% v 10.7%).
Relation between GUD aetiology and HIV infection
Typing of HSV-1 and HIV-2
HSV typing was performed retroactively after the Smart Cycler became commercially available; it was performed on previously stored DNA specimens that were tested positive for HSV by M-PCR assay and ABI 310 fragment analysis. Owing to prolonged storage and DNA degradation in some of the specimens, only 14 of 40 (35%) HSV positive specimens from 1993–4 and 57 of 67 (85%) HSV positive specimens from 1998 were typable. All of the typable specimens contained HSV-2 DNA; however, there were two specimens from 1998 also contained HSV-1 DNA.
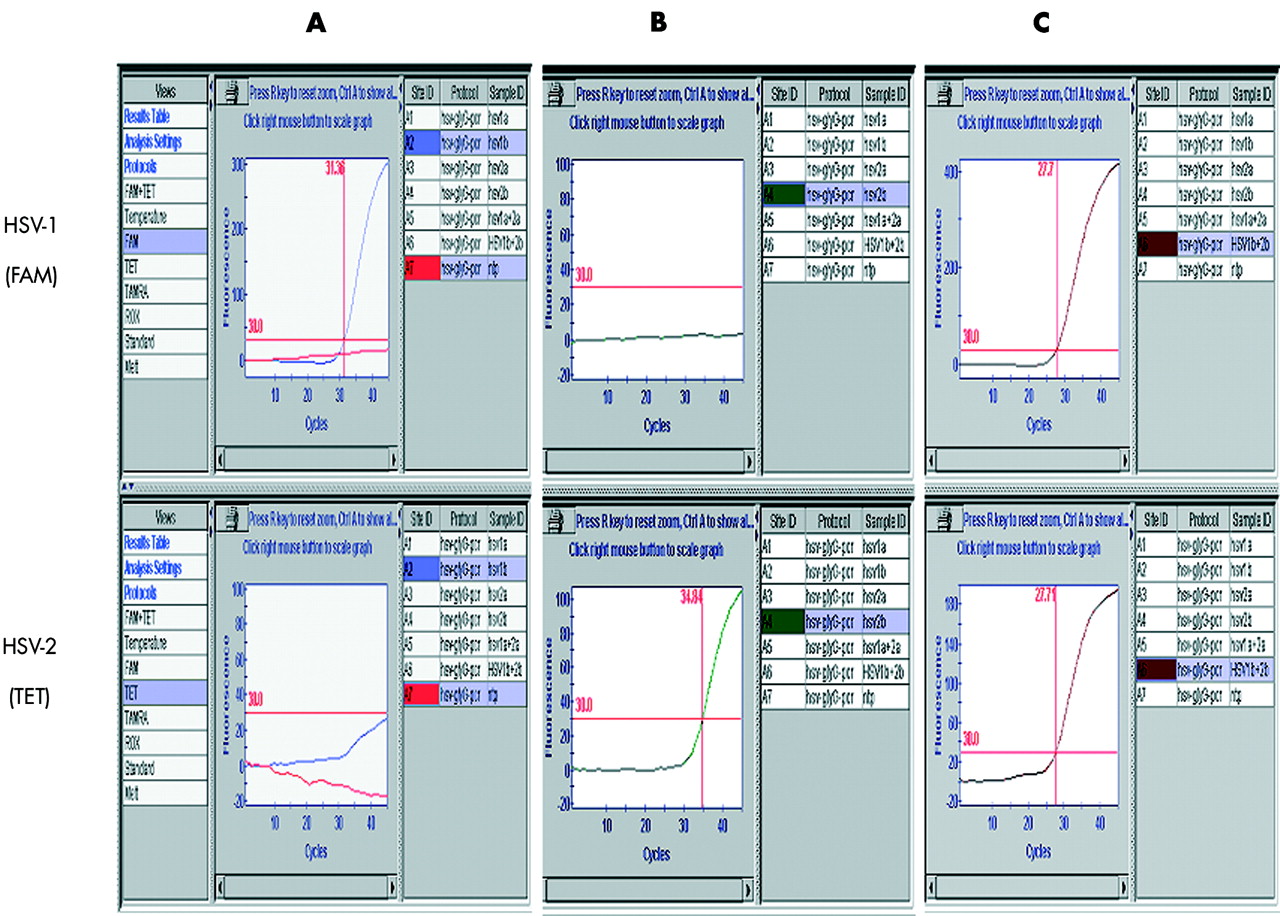
Representative results obtained when typing HSV positive specimens using the Smart Cycler are shown in figure 2. Specimens containing only HSV-1 DNA gave a positive amplification signal only on the FAM channel, which crossed the threshold level. Similarly, specimens with HSV-2 DNA alone gave a positive amplification signal only on the TET channel. Specimens containing both HSV-1 and HSV-2 DNA exhibited positive amplification signals on both channels. The sensitivity of HSV-1 or HSV-2 detection using the Smart Cycler was 1–5 genomic copies (data not shown).

{kind=link}
{kind=link}
HSV typing using the Smart Cycler. Real time M-PCR was performed using 100–500 copies of purified genomic DNA from HSV-1 and HSV-2. (A) HSV-1 DNA and no template negative control (ntp); (B) HSV-2 DNA; (C) HSV-1 plus HSV-2 DNA. FAM channel plots primary curve fluorescence v cycle number for HSV-1 and TET channel for HSV-2. Threshold limit was set at 30 fluorescence units (horizontal line). Numbers on the vertical lines represent threshold cycle values.
DISCUSSION
M-PCR results obtained from the two cross sectional surveys indicated that in each case, H ducreyi was the most frequent cause of GUD, followed by HSV-2, among men attending the STD clinic in Carletonville. However, the proportion of GUD patients with chancroid infection decreased by approximately 20% between 1993–4 and 1998, whereas the proportion of GUD due to HSV infection more than doubled. The relative prevalence of primary syphilis was similar in both surveys and was the least common cause of GUD detected in this population. The proportion of ulcer specimens containing more than one aetiological agent more than doubled (7.3% v 16.7%) from 1993–4 to 1998, with co-infections of H ducreyi with HSV being the most common. The HIV seroprevalence among the Carletonville patients has been steadily increasing, from 8% in 1991 to 52% in 1998 (Htun Ye, personal communication). The two cross sectional surveys showed a persistently high HIV seropositivity rate of 54.3% in 1993–4 and 58.8% in 1998 in this mining community. The declining rate of chancroid infection is most likely the result of widely implemented syndromic treatment for bacterial STDs in South Africa. In addition, awareness of HIV infection, success of STD control programmes, and adoption of safer sexual practices all might have contributed to the more efficient prevention of bacterial than viral STDs.
Our findings support earlier predictions that the rates of HSV infection would increase considerably as the HIV epidemic in southern Africa evolved.10 This increase has been reflected both in the prevalence of HSV-2 antibodies and in the detection of HSV-2 DNA from genital ulcer specimens. A high relative seroprevalence rate of genital herpes (49%) was detected among STD clinic patients with GUD in Uganda in 1990–1,18 while an aetiological study of GUD in Lesotho using M-PCR showed that HSV DNA was detected in 47% of ulcer specimens from HIV infected patients but in only 16% from HIV uninfected patients (p <0.001) and suggested that genital herpes may be emerging as a more frequent cause of GUD.19 Cross sectional studies of the aetiology of GUD in Johannesburg, Cape Town, and Durban, South Africa during 1993–4 indicated that, overall, HSV-2 (35.9%) was the most common agent identified in ulcer specimens and, similarly, was detected in a significantly higher proportion of ulcer specimens from HIV infected patients than from specimens from HIV uninfected patients.20 Our results demonstrated that genital HSV-2 infection was significantly correlated with HIV infection in both series and further add to the growing body of evidence in implicating the major role of HSV-2 in HIV transmission in Africa. Biological and epidemiological studies suggest potential bidirectional interactions between HSV-2 and HIV; however, the mechanism is not fully delineated. Several possibilities have been suggested including genital ulcers provide a portal of entry for HIV,21 and facilitate the transmission of HIV-1 as a result of increased HIV-1 viral load in the blood, plasma, semen, and ulcers of those with genital ulcers due to HSV-2,22–24 while HIV infection can lead to enhanced recurrences of HSV-2 infection19 and increased genital shedding.25
The limitations of the current study are that sexual behaviour factors were not addressed, and data reflect relative prevalence of STD clinic population not true population prevalence. In addition, the study was cross sectional in design and cannot imply causal association between prevalent or incident HSV-2 infection and the incidence of HIV seroconversion from the results. Recently, a longitudinal and general population based study conducted in rural Tanzania was able to quantify the causation between HSV-2 and HIV infection, and indicated that the incidence of HIV seroconversion attributable to HSV-2 infection were estimated as 74% in men and 22% in women.26 Another study conducted by performing systematic review and data synthesis from the available literature at on the effect of HSV-2 infection on HIV also reported that among HSV-2 seropositive people, 52% of sexually transmitted HIV infections can be attributed to HSV-2 infection.27 Both articles concluded that serologically documented HSV-2 infection is a significant risk factor for HIV acquisition, and there is an urgent need to identify effective HSV-2 control measures in order to reduce HIV incidence in Africa.
Infections with HSV-2 typically affect the genital area, and transmission is usually sexual. In contrast, HSV-1 commonly causes oropharyngeal lesions, and transmission is primarily by non-genital personal contact. However, both viruses are capable of causing either genital or oropharyngeal infection and can produce mucosal lesions that are clinically indistinguishable. The increasing importance of genital HSV-1 infections seen in other parts of the world was not observed in the current study; however, the steady increase of genital herpes infection among GUD patients and its strong correlation with HIV infection warrant a rapid identification as well as a typing system to clearly distinguish between genital HSV-1 and HSV-2 infections. Differentiation of HSV-1 and HSV-2 using either PCR or serology based assays have been reported in several studies.28–30 Most recently, real time PCR using the LightCycler (Roche Diagnostics Corp, Indianapolis, IN, USA) has been used to diagnose HSV infections and to type HSV-1 and HSV-2 by melting curve analysis.31 Our HSV typing system using the Smart Cycler also employed the fluorescence resonance energy transfer (FRET) technology to detect PCR products; in addition, a M-PCR assay using different fluorescent reporter molecules on the TaqMan probes was used to differentiate HSV-1 and HSV-2.
The application of rapid amplification and real time detection in conjunction with HSV serology could become a very useful tool to aid the classification of herpes infections as primary, initial non-primary, and recurrent. Based on the four channel detection capability of the Smart Cycler, the development of a single fluorescent M-PCR assay to simultaneously detect four GUD targets (H ducreyi, T pallidum, HSV-1, and HSV-2) is currently under way.
GUD diagnosis based on clinical symptoms alone is often insufficient and inaccurate.19 Conventional laboratory tests such as culture and serology improve the diagnostic accuracy in individual cases of GUD, but overall, nucleic acid amplification assays have emerged as the most sensitive methods for the diagnosis of this disease syndrome. Additional applications of the M-PCR assay include evaluating syndromic algorithms for GUD, investigating the epidemiology of GUD, assessing the accuracy of a clinical diagnosis, assessing the performance of conventional laboratory tests, assessing the appropriateness of therapy, and identifying new agents of GUD.
The use of the ABI 310 genetic analyser to detect PCR amplification products is more efficient, more sensitive, and less laborious than traditional agarose gel electrophoresis. A previous M-PCR assay for the diagnosis of GUD (Roche Molecular Systems) uses an ELISA format to detect PCR amplicons.15 We have not compared the sensitivity of target detection between the ABI 310 and ELISA methods directly, but the two methods should be comparable since both have similar target detection limits of 1–10 genomic copies. The disadvantages of using ELISA detection of PCR amplicons include the fact that the ELISA method is not able to rule out non-specific reactions as well as the fact that it is both labour intensive and time consuming.
The high relative prevalence of HSV-2 infection in GUD patients demonstrated here may limit the effectiveness of interventions using antibiotics alone as a means of controlling GUD and preventing HIV infection. The identification of men with HSV-2 infection, subsequent counselling on the nature of the disease, the importance of avoiding unprotected sexual contact during disease episodes and avoiding contact with sex workers may be appropriate measures required to reduce the incidence of HIV infection. The demonstration of increasing relative prevalence of HSV-2 infection among GUD patients from the mining community of Carletonville strengthens the need to evaluate the effectiveness of specific anti-herpes chemotherapy in reducing the incidence of HIV infection when planning future STD control programmes in this population.
CONTRIBUTORS
WL, M-PCR assay performance and manuscript preparation; CYC, laboratory supervision, data analysis and manuscript preparation; SAM, interpretation of results and commented on the manuscript; YH, HGF, on-site project coordination, implementation, and data collection; HL, assisted in genetic analyser setup and performance; RCB, principal investigator, project design and supervision.