Article Text

Abstract
Objectives: To better understand the sexually transmitted infection (STI)/HIV dynamics in an urban west African setting in order to adapt STI/HIV control efforts accordingly.
Methods: Review of STI and HIV epidemiological studies performed over the past decade in Bobo-Dioulasso, the second city of Burkina Faso. Trends in STI prevalence among commercial sex workers and the general population were assessed over time through studies that used the same recruitment and laboratory diagnostic procedures. Variations in aetiologies of vaginal discharge, urethral discharge, and genital ulcers were also evaluated among patients consulting for genital infection complaints. Antenatal clinic based surveys provided data to assess HIV trend among the general population.
Results: We observed an important decline of classic bacterial STI such as syphilis, Neisseria gonorrhoea, Chlamydia trachomatis, and Haemophilus ducrey infections in all study groups. Trichomoniasis also declined but to a lesser extent. HIV infection followed the same trend at the same time, with a significant decline in the 15–19 year age group of pregnant women, suggesting a possible decrease of HIV incidence. Although no evidence of a causal relation can be drawn from this review, adoption of safer sex behaviour, introduction of the syndromic management (SM) approach, or higher antibiotic use may have contributed to these changes.
Conclusions: Classic bacterial STI declined over the past decade in parallel with a stabilisation of HIV infection. Variations in syndromes aetiology and sexual behaviours should be monitored as part of STI surveillance in order to improve STI syndromic management algorithms and to adapt HIV/STI prevention efforts.
- Africa
- epidemiology
- STI
Statistics from Altmetric.com
Enhancing and optimising the management of sexually transmitted infections (STI) remains one of the most feasible and cost effective interventions to control HIV in sub-Saharan Africa.1–3 The adoption of the syndromic management (SM) approach has provided a simplified and cheap method for this purpose. However, SM performance can vary with many determinants, such as health seeking behaviours, cultural or economic factors, the distribution of major aetiologies of STI syndromes among men and women, or possible changes in STI ecology over time.4 For the latter reasons, the World Health Organization (WHO) has advocated regular assessment of the main aetiologies of STI syndromes in order to adjust management algorithms accordingly.5
The national STI programme of Burkina Faso (west Africa) has adopted SM since 1996 and has commissioned SM aetiological studies nationwide. In 1997, the official HIV prevalence of the country was estimated at 7.2%. In this paper, we present a review of HIV and epidemiological data from Bobo-Dioulasso—the second largest city (about 500 000 inhabitants). Such information is of importance to the national STI programme authorities to improve patients’ management strategies. Furthermore, it should help understand the dynamics of HIV/STI epidemiology in an urban African setting.
METHODS
We performed our review at two levels: firstly we present data on the STI and HIV prevalence trends in various subgroups; secondly, we present studies assessing the aetiological pattern of three major STI syndromes: vaginal discharge syndrome (VDS) in women, urethral discharge syndrome (UDS) in men, and genital ulcer syndrome (GUS) in men. All STI or HIV prevalence studies performed at Centre Muraz were eligible, but only those for which a comprehensive final report was available were selected. Additional information could be obtained from laboratory technicians still working at the centre and involved in the field work of the considered surveys. In order to allow some comparisons over time, selected studies were similar in data collection methods and laboratory procedures. When not strictly identical, populations sampled were as similar as possible. All studies were undertaken by Centre Muraz in the city of Bobo-Dioulasso over the period 1990–2000. Data sources are summarised in table 1.
Study populations and data sources for STI/HIV prevalence and STI aetiologies in Bobo-Dioulasso, Burkina Faso, 1990–2000
Data sources
STI prevalence studies
Studies among female high risk groups
STI rates were assessed among bar waitresses and self defined commercial sex workers (CSW) in 1990 (n = 182)6 and 1994 (n = 215).7 The baseline results of an ongoing cohort study among CSW and bar waitresses were used to get more recent data (1998–2000).8 Participants from all three studies were recruited in the field with the help of peer educators and other key informants connected with the local sex industry. They were asked to go to the Centre Muraz for examination and sampling. All consecutive women presenting at the centre were included in the study until sample size completion.
Studies among the general male and female population
Trends in STI among the general population were evaluated through three clinic based surveys of pregnant women and a community based survey. In 1990 and 1991, two similar STI surveys were performed among pregnant women (n = 118 and n = 172, respectively) recruited in antenatal clinics (ANC) of the city (unpublished data). More recently, in 2000, a large population based survey was undertaken to assess the HIV/STI situation in both the youth and adult community (unpublished data). A two stage cluster design was used after a mapping update of the selected areas. Data on STI prevalence rates were available for 1004 women and for 1087 men aged 15–49 years.
STI aetiological studies
Vaginal discharge syndrome (VDS)
A first study was conducted in 1992 among 223 consecutive women attending a gynaecological outpatient department at a referral hospital with a vaginal discharge complaint.9 In 1998, a second study was conducted that evaluated the recently adopted national STI treatment algorithms. Overall, 636 adult women consulting at primary healthcare centres for genital complaint underwent a gynaecological examination and sampling for STI diagnosis (unpublished data).
Urethral discharge syndrome (UDS)
A first survey undertaken in 1990–1 enrolled 205 men attending nine health centres and further referred to the Centre Muraz for laboratory tests6: 38% (78/235) of men presented with UDS, 31% (73/205) with GUS, and 9% (21/235) with both syndromes; thus 99 men with UDS were included for analysis. The 1998 aforementioned STI aetiological study conducted among women also recruited 50 male patients complaining of urethral discharge, which will provide our second estimate of the UDS aetiological pattern (unpublished data).
Genital ulcer syndrome (GUS)
Only data for men were available. The 73 (SD 21) men described above in the 1990–1 study were selected for this syndrome. No recent data are available since the 1998 evaluation of the treatment algorithms only found 13 cases of ulcers (six in men and seven in women) over the study period (8 months).
HIV studies
High risk groups
The STI studies described above among CSW and female patients consulting primary health centres for genital complaints provided data to assess variations in HIV prevalence over time in these high risk groups. HIV prevalence data from 1990–1 and 1998 in men consulting for urethral discharge were also used.
General population
HIV prevalence data for 1990 and 1991 were obtained from the two studies of pregnant women described earlier (n = 118 and 172, respectively). Both used an unlinked and anonymous strategy. Between 1995 and 2001, trends in HIV prevalence in the female population were assessed through unlinked anonymous sentinel surveillance surveys conducted among pregnant women recruited in two identical clinics over time.10,11
Additional data were obtained from a national and anonymous HIV prevalence survey carried out in 1994 by the National AIDS Control Programme of Burkina Faso which included 408 pregnant women who consulted an antenatal clinic in Bobo-Dioulasso.12
Laboratory procedures
Most studies used similar microbiological procedures for STI diagnoses. Cultures were done on specific milieux for Neisseria gonorrhoeae (NG), Haemophilus ducreyi (HD), and Candida albicans (CA). Detection of Chlamydia trachomatis (CT) was performed by direct immunofluorescence (DIF) test (Biomérieux SA, France), with the exception of the 1999 study on patients consulting for STI in which laboratory diagnosis was based on a rapid test (Chlamygen Rapid Chlamydia Swab Test, Genelabs diagnostics, Geneva, Switzerland). Diagnoses of Trichomonas vaginalis (TV) and bacterial vaginosis (BV) were made on wet mount direct microscopy by observation of motile flagellated organisms and clue cells, respectively.
The 2000 survey performed on general population employed more recent techniques. A polymerase chain reaction (PCR) technique in urine was used to detect chlamydial and gonococcal infections (Amplicor CT/NG, Roche Diagnostics Inc, Branchburg, NJ, USA), and identification of TV relied on a culture method (Inpouch TV, Biomed Diagnostics, San Jose, CA, USA).
Active or recent syphilis was defined as dual seroreactivity to rapid plasma reagin (RPR, Human GmbH, Wiesbaden, Germany) and Treponema pallidum haemaglutination assay tests (TPHA, Newmarket Laboratories Ltd, Kentford, UK). The technique chosen for diagnosing HIV-1 infection changed over time but was always based on a two test combination: either ELISA and western blot or two complementary ELISA as described.13 Serological herpes simplex virus (HSV-2) infection was diagnosed by means of type specific HSV-2 IgG ELISA tests (Gull Meridian Laboratories, Homberg, Germany).
Statistical procedures
The χ2 tests and χ2 tests for linear trends were used for statistical significance between proportions. Confidence intervals were calculated when necessary in order to provide information on the precision of results.
Ethical issues
All studies mentioned in this paper received the approval of the Ministry of Health of Burkina Faso. Informed verbal consent was obtained from all participants in their respective languages. All patients diagnosed with genital infections received free treatment from the medical study team. HIV testing was done anonymously. Voluntary counselling and testing (VCT) services were offered from 1998 onwards.
RESULTS
STI trends (figs 1 and 2)

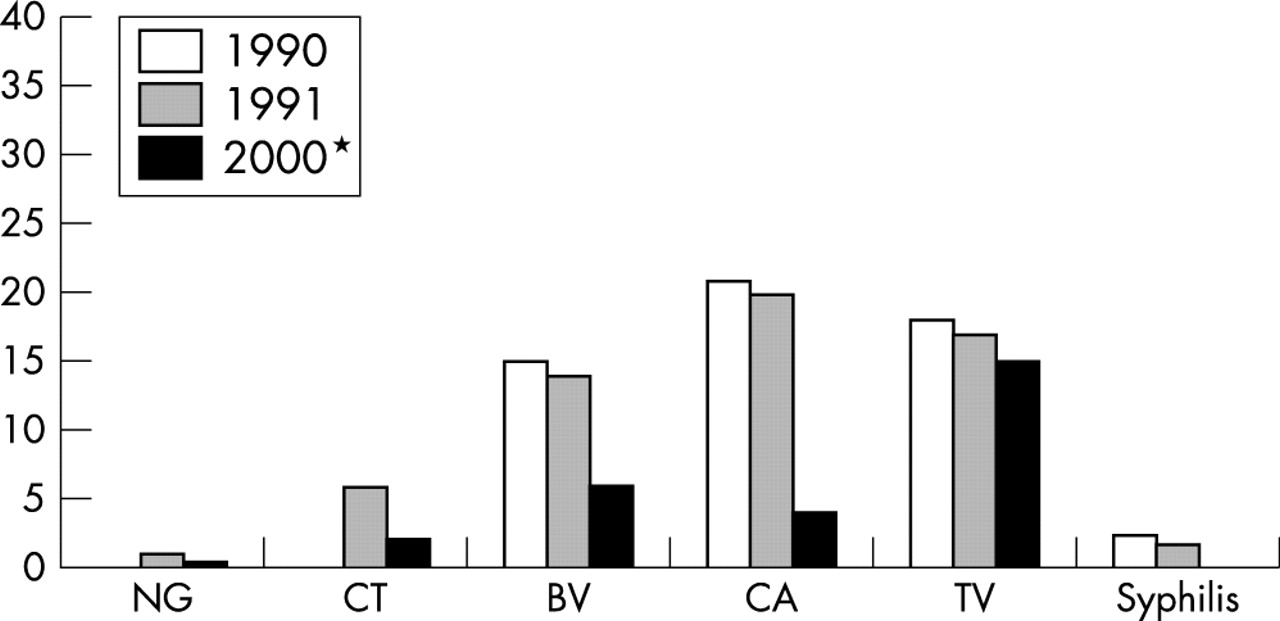
Genital infections trends among CSW in Bobo-Dioulasso, Burkina Faso, 1990–2000.
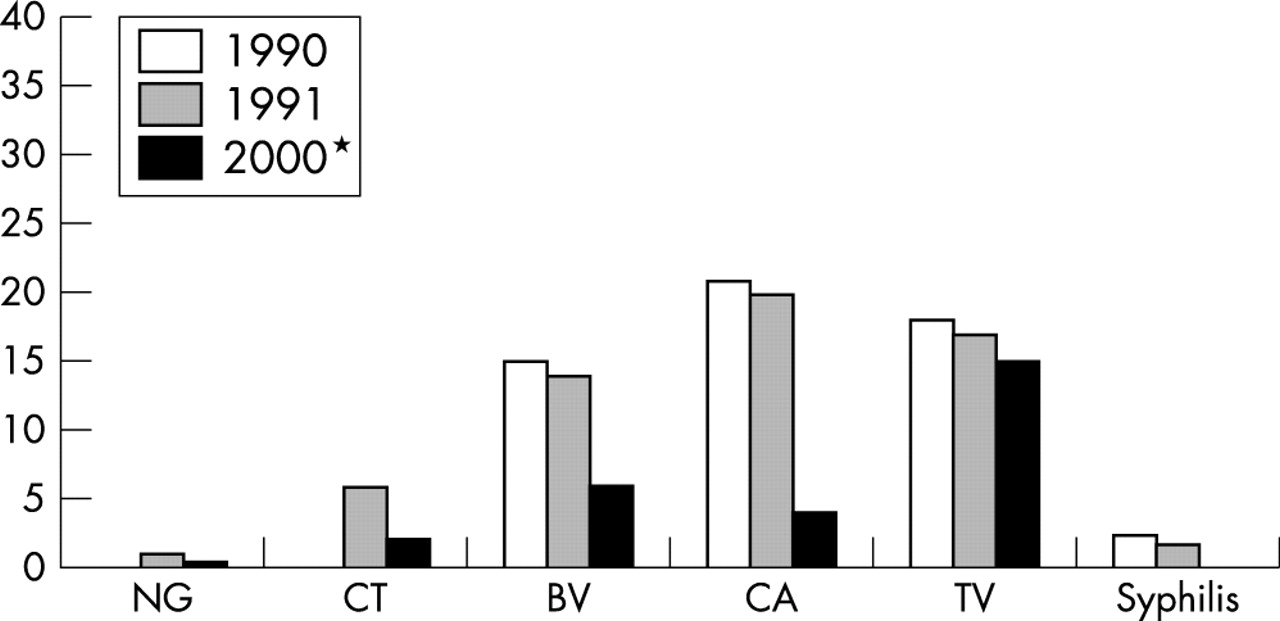
STI trends among pregnant women (1990–1) and the general population (2000) in Bobo-Dioulasso, Burkina Faso, 1990–2000. *General population based survey.
Acute or recent serological syphilis decreased dramatically in any study groups. This fact was particularly obvious among CSW in whom a sharp decline occurred between 1991 and 1998–2000 (from 12.5% to 0.8%, p<0.001) (fig 1).
No cases of HD infection were recorded in GUS studies performed between 1998 and 2000.
Data on HSV-2 seroprevalence are scanty in the region. Only the population based survey performed in 2000 in Bobo-Dioulasso found a HSV-2 prevalence of 24% (95% CI 21.6 to 26.4) in women and 12.5% (95% CI 10.6 to 14.4) in men.
Levels of gonococcal infection significantly declined since 1994. Less than 1% of CSW were infected with NG in 1998–2000, in contrast with the 13% prevalence recorded in 1994 (p<0.001). The low prevalence recorded in 1991 among pregnant women (1%) was halved in 2000 in the population based survey (0.5%) without reaching statistical significance.
CT prevalence also declined by almost 50% among CSW and the general population between 1990–1 and 2000, with infection rates dropping from 10.0% to 6.6% (p = 0.16), and from 6% to 2% (p = 0.02), respectively, even though a more sensitive test was used for CT detection in 2000.
Microorganisms causing vaginal infections showed a more mixed picture. TV infection fell among CSW from 32.0% to 9.7% (p<0.001), whereas the decline in the general female population was not significant and stabilised at around 15.0%. Prevalence of BV (14–16%, p<0.001) and CA (20 to 4%, p<0.001) dropped significantly between 1991 and 2000 in the general female population, although CA prevalence rose among CSW over the same period.
A striking feature is that all these changes occurred after 1994. Studies from 1990, 1991, and 1994 showed a remarkable consistency and stability in infection rates across populations, whereas later studies conducted in 1998, 1999, and 2000 showed much lower rates in general, despite the use of more sensitive detection techniques.
STI syndrome aetiologies
Vaginal discharge syndrome
Among female patients consulting for a complaint of vaginal discharge, the prevalence of gonococcal infection decreased from 11% in 1992 to 1% in 1999 (p<0.001), whereas the prevalence of CT decreased from 27% in 1992 to 1.5% in 1999 (p<0.001). However, the latter prevalence may be artificially low, as CT diagnosis was done using a rapid ELISA test (Chlamygen), which replaced our own previous DIF test, without prior evaluation in our laboratory.
The prevalence of TV, CA, and BV in this syndrome also declined from 28% to 15% (p<0.001) for TV, 17% to 14% (p = 0.6) for CA, and 20% to 15% (p = 0.5) for BV.
Urethral discharge syndrome (UDS)
The classic major role of NG in male UDS declined remarkably from 63.6% in 1991 to 26% in 1998 (p<0.001). The identification of CT in this syndrome remained steadily low at 3.4% in 1990 and 4.1% in 1998.
Genital ulcer syndrome (GUS)
In 1991, HD was isolated in 25/82 (30%) of GUS. No recent data could be obtained because of the rarity of this syndrome in our practice as highlighted by the recent GUS algorithm evaluation study conducted in 1999 which could not reach the required sample size for this syndrome.
HIV infection
The situation of HIV infection (table 2) was somewhat similar to that of STI. HIV prevalence among CSW decreased significantly over the period 1994–2000 (from 57% to 41%, p<0.001), whereas among female patients with STI the same trend was observed between 1992 and 1998 (from 42% to 17%, p<0.001). A significant decline was also observed in the female general population over time between 1990 and 2001 (from 7.0% to 5.7%, p for trend <0.001) after reaching a peak (12.7%) in 1994.
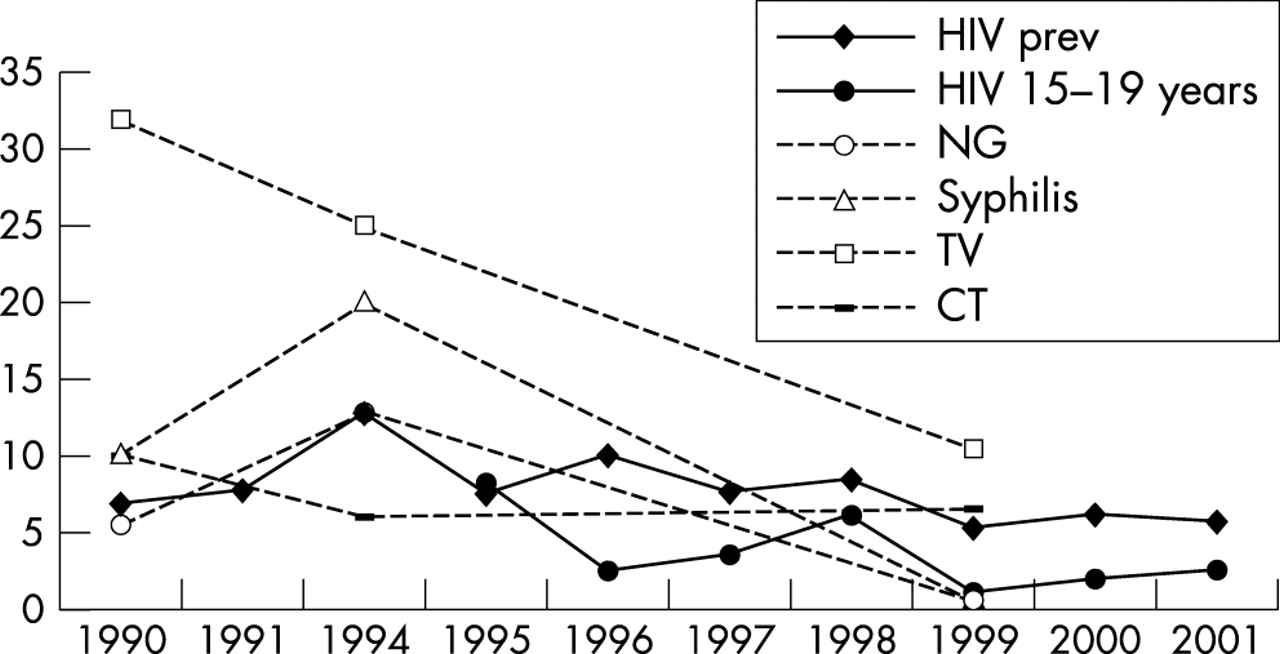
HIV trends among pregnant women, 15–19 year old pregnant women, and CSW over the past decade
We used HIV prevalence rates in the youngest group of sexually active surveyed population in Bobo-Dioulasso as a proxy for HIV incidence (table 2). This method has proved to be reliable in Thailand.14 Whereas a downward trend appears throughout the period (p for trend = 0.003), a sharp decrease occurred between 1998 and 1999 (from 6.2% to 1.2%, p = 0.02), with confirmation in 2000 and 2001, suggesting a recent marked decline of HIV incidence.
In order to provide the reader with a global view of the situation, HIV prevalence data from antenatal clinics, as well as STI data from CSW, were plotted over time in figure 3.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The review of studies performed in Bobo-Dioulasso over the past decade suggested a substantial change in STI ecology and epidemiology. In women, the prevalence of ulcerative STI such as chancroid and syphilis have become extremely rare in low and high risk groups. The prevalence of NG and, to a lesser extent, that of TV and CT followed a similar decline. Furthermore, the role of CT and NG in the aetiology of VDS and urethral discharge in men also markedly declined, suggesting a global and sharp decrease of CT and NG load in the community.
Beside these classic STIs, the prevalence of other genital infections, such as BV and CA, tended also to decline in the general population but not among CSW.
Similarly, HIV prevalence and probably HIV incidence curved down in both high risk groups and the general population over the same period of observation.
There is no doubt that the interpretation of these ecological trends has a few limitations. Firstly, the studies selected for this work were not specifically designed to assess variations over time. However, within each of the study populations (in particular CSW), the selected studies used the same recruitment procedures. Overall, the same biological procedures were applied for STI diagnosis over our study period, with only more sensitive tests used recently.
Whether study populations are similar enough to be compared over time is another point of concern that appears particularly relevant for CSW. Although the commercial sex profile changed during the period 1990–2000 with increased clandestine activity,8 the subgroups of true professionals and bar waitresses did not vary much according to our experience. There has been, however, a shift in the origin of CSW—with a predominance of Ghanaian women in the early 1990s and of Nigerians nowadays—as recently found in Benin.15 It is feasible that shifts in STI ecology in these women may reflect similar patterns in their country of origin.
It is also noteworthy that no specific STI or HIV related interventions targeting CSW took place in Bobo-Dioulasso before the end of 1998. About three quarters of the 1998–2000 sample size consisted of baseline data from women enrolled in the cohort study. Furthermore, it is very unlikely that some individuals were recruited in more than one study considering the high mobility and turnover of women entering sex work. Therefore, any intervention effect is unlikely to have dramatically distorted results.
The small sample sizes of some of the studies may give rise to imprecise prevalence rates with large confidence intervals. However, this is less of a problem when analysing trends rather than point estimates.
Finally, the quality of the Centre Muraz laboratory can be questioned. However, because the same biological tests were used for STI diagnosis, any potential bias introduced by deficient biological procedures is likely to be of minor importance for comparison purposes. The recent use of molecular biology for NG and CT diagnosis confirmed the previous results found in CSW with standard microbiological tests. Prevalence of 2% and 1% for NG and CT, respectively, was found during the follow up of the ongoing CSW cohort by use of PCR (PCR NG/CT, Roche Diagnostics Inc, Branchburg, NJ, USA). These PCR tests were performed by the “laboratoire de l’Unité de recherche en santé des populations, Centre hospitalier affilié universitaire de Québec.”
Several factors already implicated in the decline of STI in previous studies may have also been involved in our setting, although no causal relation can be drawn from our data.
Adoption of safer sex behaviour is an obvious factor to consider. Lessons learned from Uganda suggest a long term decline of HIV prevalence in parallel with changes in sexual behaviour.16 Similar data come from Rwanda17 and Thailand18 where a decline in STI and HIV incidence was observed in a cohort of male conscripts with a parallel increase in condom use. In former Zaire, identical findings were found among CSW.19 Because no comprehensive data were available in our context, we used surrogate indicators, such as condom availability, which significantly increased during the study period. Owing to the development of a condom social marketing programme since 1991, the average number of condom available per person per year in the sexually active population increased sharply from 0.6 in 1992 to 6.0 in 1999.11 Therefore, we believe that increased condom use may be implicated to some extent in the observed changes in STI ecology and HIV prevalence.
The SM approach was reported to increase treatment seeking behaviour and to improve STI case management.20 The same consequences may possibly applied in Bobo-Dioulasso after its introduction in 1996. It is striking that the decrease in STI originated after 1994 whereas no real change was recorded beforehand. However, the SM approach is far from perfect4,21 for syndromes such as vaginal discharge. In addition, it is unable to tackle asymptomatic STI.
Self medication may also be implicated in the change of STI ecology. Among CSW, preventive self medication for STI is a common practice since 14% (n = 447) of women taking part in our cohort admitted taking antibiotics every month for this purpose (unpublished data). This particular aspect might also be involved in the increase of CA prevalence among this high risk group, although no data are available for antibiotic use for the studies performed in 1989–91 and 1994.
We can confidently suggest that the HIV epidemic is now at least stabilised11 and possibly declining in Bobo-Dioulasso. The recent decrease of prevalence among the 15–19 year age group of pregnant women, which closely mimics HIV incidence, would support this hypothesis.
However, it is noteworthy that the 1990 and 1991 studies were performed in four identical antenatal clinics whereas only two of them were used in the latter studies. The two additional antenatal clinics were public ones located in the city centre thus providing a somewhat similar level of service to the general population. Therefore, we believe that this potential bias was unlikely to dramatically distort the HIV trend.
Moreover, our small sample size yielded volatile data, which prevent us from drawing definite conclusions.
The similar variation of HIV infection among the different population groups cannot be dissociated from the trends observed in genital infections over the same period. This situation may suggest a “reverse causation” mechanism by which various factors (SM, HIV prevention efforts, etc) reduced HIV prevalence and incidence that in turn changed prevalence of STI, but also altered vaginal flora.
There are limited data on STI ecology trends over time from other African countries. Recent data originated from Cote d’Ivoire22 and Benin15 where an STI management and prevention strategy dedicated to CSW contributed to a remarkable decrease in the prevalence of HIV and other STI (much remarkable for ulcerative STI) in this high risk group. There is now increasing evidence that the epidemiology of the GUS syndrome is also changing in east and South Africa where genital herpes is becoming the most frequent infection,23–25 with a decline of bacterial infections such as chancroid.26 Lower seroprevalence rates of syphilis were also reported in Kenya among pregnant women from 1995 onwards.27 Other data are available through trials or intervention studies that were successful in reducing the STI burden by introducing a specific intervention as demonstrated in a South African mining site28 and on a larger scale in the general population of Mwanza, Tanzania. In the latter trial, improved STI treatment services at the community level resulted in decreased prevalence of STI at follow up, most remarkably seen with male urethritis and active serological syphilis.20
Our data can hardly be compared with these findings, but we observed changes in genital infections other than syphilis and NG. Moreover, concomitant stabilised HIV prevalence with a probable declining incidence is described for the first time in a public health context in west Africa.
The main genital infections currently affecting both high risk groups and the general population of Bobo-Dioulasso are likely to be genital herpes and BV. Given the increasing evidence of epidemiological and biological synergy between HSV-2 and HIV,29,30 we would expect an increase of GUS caused by HSV-2 or increased shedding. Further studies should be conducted to assess the importance of HSV-2 infection in our context. A low HSV-2 seroprevalence or incidence in younger age groups may signify a lower exposure to HIV and changes in sexual behaviour.
Similarly, BV is probably of major importance with respect to HIV infection in our context. Despite a low association with HIV acquisition,31 the high frequency of BV in all study groups probably results in a high attributable risk of HIV acquisition in the general population.32
Unfortunately, these two infections are generally not captured through the SM approach. There is no cost effective treatment available for genital herpes and the 2 week metronidazole treatment regimen recommended for BV in Burkina Faso leads to poor compliance and recurrences.33
CONCLUSION
We observed an important drop of bacterial STI over the past decade in this urban west African setting in parallel with a stabilisation of HIV infection.
These changes in genital infections ecology highlight the need to strengthen surveillance to be able to adjust the syndromic approach according to the epidemiological situation and the needs of the population. This surveillance should not only consist of the quantification of syndromic cases, but it should also be able to monitor changes in sexual behavioural as well as aetiological aspects of syndromes. Ideally, this global surveillance should target both “high risk groups” and the general population. The current introduction of the second generation surveillance for HIV in Burkina Faso will partly enable the achievement of these objectives.
Finally, the specific STI ecology in Bobo-Dioulasso drives future research efforts towards non-bacterial causes of genital infection such as BV and genital herpes.
Key messages
-
In this urban African setting, classic bacterial STI dropped dramatically over the past decade in parallel with a stabilisation (if not a decline) of HIV infection to about 5% of prevalence, although no direct link can be established between these trends
-
Althouth much focus was given to classic bacterial STI for HIV control purposes so far, there should now be a switch in public health policy towards other genital infections, such as genital herpes and bacterial vaginosis
-
These observations stress the need for a good STI and HIV surveillance system (including sexual behaviours), which is rarely given a high priority in west Africa
Acknowledgments
Sources of funding include the Agence National de Recherche sur le SIDA (ANRS, France) for the studies on CSW, UNFPA and UNAIDS for the study in the general population of Bobo-Dioulasso (2000), FHI and the World Bank for the studies performed by Lankoande Salif and colleagues.
Some financial support was also provided by the Knowledge Programme on HIV/AIDS and STI of the London School of Hygiene and Tropical Medicine (LSHTM), which is funded by the Department for International Development (DFID), UK.
The authors thank Philippe Mayaud (LSHTM) for his support and critical review of the manuscript, Michel Alary and Danielle Fortin for the performance of NG/CT PCR in Quebec, and the Secretariat Permanent of the Comité National de Lutte contre le SIDA for the provision of the HIV surveillance data.
CONTRIBUTORS NN led the data analysis and wrote the first draft of the manuscript; NM participated in the data analysis and the writing; AO, AO, and MCD were actively involved in the CSW studies data collection and they all contributed to the writing; HB assisted with the analysis; SY and IS coordinated the field work for the 2000 study among the general population and reviewed the manuscript; PVP directed all studies performed from 1998 and contributed to the writing.
REFERENCES
Footnotes
-
↵* STI data from the 1998–2000 study among CSW plotted as from 1999. Similarly, 1989–91 data were plotted as from 1990. HIV prev=HIV prevalence; HIV 15–19 years=HIV prevalence in the 15–19 years age group from HIV sentinel surveillance among pregnant women.