Article Text

Abstract
Sexually transmitted infections (STIs) constitute a huge health and economic burden for developing countries: 75–85% of the estimated 340 million annual new cases of curable STIs occur in these countries, and STIs account for 17% economic losses because of ill health. The importance of STIs has been more widely recognised since the advent of the HIV/AIDS epidemic, and there is good evidence that the control of STIs can reduce HIV transmission. The main interventions which could reduce the incidence and prevalence of STIs include primary prevention (information, education and communication campaigns, condom promotion, use of safe microbicides, and vaccines), screening and case finding among vulnerable groups (for example, pregnant women), STI case management using the syndromic approach, targeted interventions for populations at high risk (for example, sex workers), and in some circumstances (targeted) periodic mass treatment. The challenge is not just to develop new interventions, but to identify barriers to the implementation of existing tools, and to devise strategies for ensuring that effective STI control programmes are implemented in the future.
- sexually transmitted infections
- sexually transmitted diseases
- developing countries
- public health
Statistics from Altmetric.com
This paper reviews the extent of the burden of sexually transmitted infections (STIs) in developing countries, with a focus on Africa, and the main strategies that can be used in STI control programmes. We present some of the evidence of the impact and (cost) effectiveness of key STI interventions that have been used in developing countries. We did not intend to perform a systematic review of STI interventions but, rather, decided to include relevant studies and trials that could best illustrate key control strategies in various parts of the world. We first conducted a search of Medline with no date restriction with the key words “sexually transmitted infections” (or diseases) and “interventions” and “developing countries.” We consulted the Cochrane Library for randomised trials on STI and relevant topics (for example, partner notification). We made use of WHO publications on HIV and STI, existing systematic reviews, and our own personal libraries.
STIs IN DEVELOPING COUNTRIES: THE EXTENT OF THE PROBLEM
The World Health Organization (WHO) estimates that approximately 340 million new cases of the four main curable STIs (gonorrhoea, chlamydial infection, syphilis, and trichomoniasis) occur every year, 75–85% of them in developing countries (fig 1).1 STIs impose an enormous burden of morbidity and mortality in developing countries, both directly through their impact on reproductive and child health, and indirectly through their role in facilitating the sexual transmission of HIV infection. The high prevalence of STIs has contributed to the disproportionately high HIV incidence and prevalence in Africa. Conversely, HIV may have contributed to some extent to STI increases, especially of viral agents such as herpes simplex virus (responsible for genital herpes) or human papillomaviruses (some strains being responsible for genital warts, others for cervical, anal, or penile cancers). The greatest impact is on women and infants. The World Bank has estimated that STIs, excluding HIV, are the second commonest cause of healthy life years lost by women in the 15–44 age group in Africa, responsible for some 17% of the total burden of disease.2
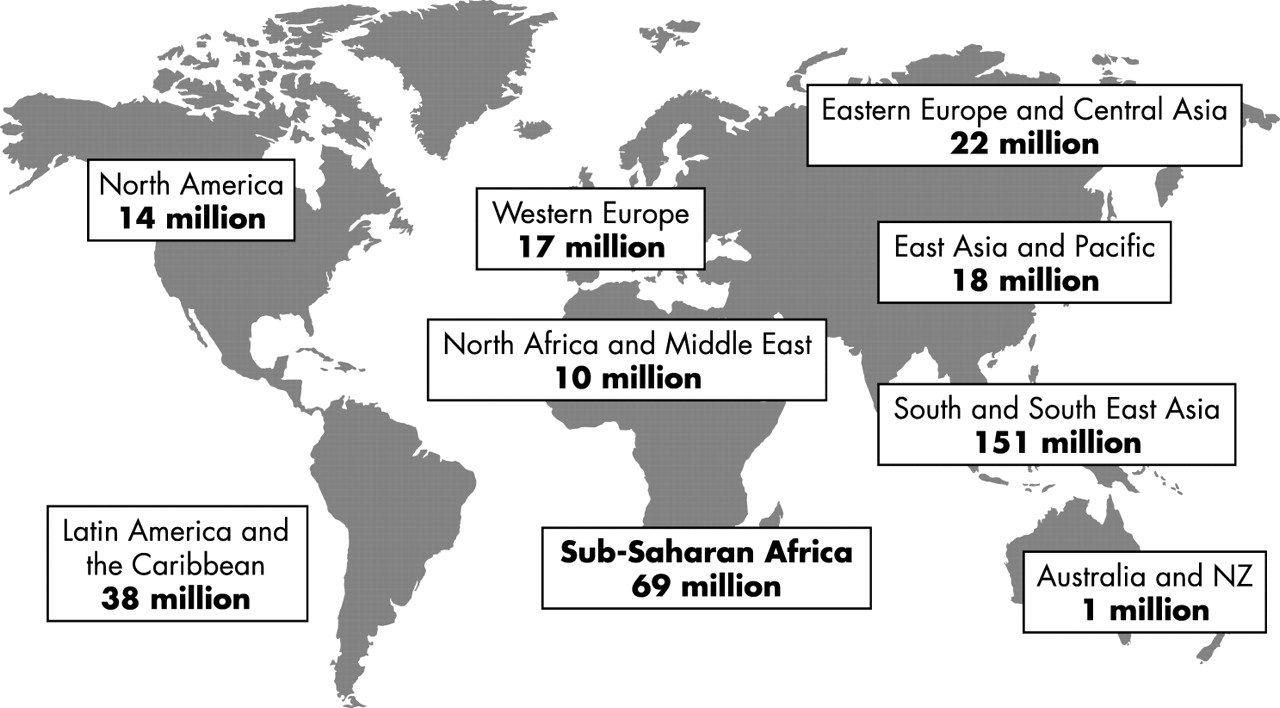
Estimated new cases of curable STIs among adults, 1999. Global total 340 million. (Source: WHO.1)
Systematic and comprehensive STI surveillance is almost non-existent in developing countries. Most epidemiological data have been obtained from prevalence studies, and from sentinel surveillance sites in a few countries. Prevalence surveys suffer from the disparity of population groups surveyed, which have included university students, antenatal clinic attenders, STI clinic attenders, and sex workers. As an example, table 1 summarises the results of a number of prevalence surveys conducted in sub-Saharan Africa. Until the 1990s there were few data from rural communities, but large community based studies conducted in Tanzania and Uganda in recent years have provided a wealth of data on STI incidence and prevalence.3–6 Some reasons for the high prevalence and incidence of STIs in developing countries are shown in box 1
Prevalence of STIs and RTIs (reproductive tract infections) among women in sub-Saharan Africa in the 1980s and 1990s
Box 1 Factors underlying the high prevalence of STIs in developing countries
-
Demographic factors (a large young population which is sexually active)
-
Urban migration with accompanying sociocultural changes
-
Migration and displacement (labour, wars, natural catastrophes)
-
Increase in levels of prostitution through economic hardship
-
Multiple and concurrent sexual partnerships
-
Lack of access to effective and affordable STI services
-
High prevalence of antimicrobial resistance for some pathogens
CONTROL OF STIS
According to the WHO and UNAIDS,7 STI control programmes have three objectives:
-
to interrupt the transmission of STIs;
-
to prevent the development of diseases, complications, and sequelae; and
-
to reduce the transmission of HIV infection.
Health education and condom promotion can modify behaviour, and hence reduce the incidence of STIs. Screening, case finding, improved access to care, and improved case management can prevent complications, and also reduce transmission, by shortening the duration of infection. Mass or targeted presumptive periodic treatments attempt to bypass the need for treatment seeking, since STIs are frequently asymptomatic, with the aim to reduce incidence by reducing the pool of infected individuals, in populations with high STI prevalence or incidence.
Key messages
-
STIs constitute a huge health and economic burden for developing countries: 75–85% of the 340 million annual new cases of curable STIs occur in these countries; STIs account for 17% economic losses caused by ill health in 15–44 year old women
-
STI case management using the syndromic approach is a feasible, adaptable, and cost effective approach; it works best for the management of genital ulcer disease and urethral discharge in men
-
Community randomised trials in Uganda and Tanzania have shown that STI case management can reduce STI prevalence and incidence in the community, and this in turn can help reduce HIV incidence in settings where curable STIs are highly prevalent
-
Simpler and cheaper point of care screening tools are urgently required
-
STI control can only be achieved by a combination of interventions, backed by strong political and financial commitment
Primary prevention of STI
Behavioural interventions
Primary prevention aims to modify sexual behaviour in many ways: by encouraging delayed onset of sexual debut, sexual abstinence and mutually faithful sexual relationships, as well as by promoting “safer sex,” which include the reduction of the number of sexual partners, the adoption of “safer” sexual practices such as non-penetrative genital contacts, and finally by promoting the correct use of condoms. This is achieved through information, education and communication (IEC), or peer assisted education programmes. It is particularly important in adolescents, as they often have high rates of STI, but are at the same time more likely to change their behaviour. Interventions targeting individuals often rely on the “rational health belief model,” which is based on the assumption that an individual has the power to make necessary changes. However, in many instances, drugs, poverty, or gender can diminish an individual’s ability to act on his/her intentions.8 Few rigorous studies have evaluated the impact of behavioural interventions on STIs and HIV,9,10 and disappointingly have shown that reported changes in behaviour have not always been reflected in changes in STI incidence or prevalence.11,12 However, changes in sexual behaviour evidenced by increased delays in first sex and reduction of the number of partners account for some of the most impressive reductions in HIV prevalence and incidence rates observed in Uganda, although their concomitant impact on STIs has not been measured.13
Barrier methods
When used properly and consistently, condoms are one of the most effective methods of protection against HIV and STIs.14 They can be made readily available on a large scale through free distribution or social marketing, which uses marketing techniques to make these commodities available at affordable prices. In Thailand, the 100% condom programme, which has been promoting 100% use of condoms in commercial sex establishments, overcame many cultural and logistical barriers traditionally associated with condoms. The programme has been linked to increased adoption of safer sex measures, and concomitant decrease in reported STI rates and HIV prevalence among Thai military recruits15 and a decrease in the number of men attending STI clinics nationwide.16 However, despite considerable efforts by numerous agencies, and an overall increase in condom sales over the past decade, only a small proportion of the sexually active population in many countries use condoms; and those who do may do so irregularly and only with selected partners. Barriers to consistent use of condoms include high price, low availability, and inadequate marketing.14 Women may also be forced into unprotected intercourse as a result of unequal power relations between sexes.
Female controlled methods of STI prevention
STIs disproportionately affect women and, in particular, adolescent women are at increased risk, because of ignorance of appropriate preventative measures, and unplanned or forced sexual intercourse where it may be difficult or impractical to negotiate safer sex. Female controlled methods of protection are therefore badly needed. These could include female condoms and vaginal microbicide compounds. Unfortunately, both types of methods have proved rather disappointing or of limited use. The female condom has important advantages such as efficacy, safety and, in some areas, increasing acceptance by women. However, disadvantages include high cost, lack of visual and auditory appeal, difficulty of use, pre-planning of intercourse, and mixed reactions among male partners.17 Vaginal microbicides have been under development since the early 1990s. A detergent based chemical (nonoxynol 9, or N-9) with virucidal and bactericidal activity raised initial hopes, but eventually proved disappointing for HIV prevention.18 Some compounds are not always reliably effective against STIs, and there is also concern that repeated use can disrupt the vaginal epithelium and actually make users more susceptible to infections. However, a number of new and safer compounds are currently under development and should be carefully evaluated.19
Vaccines
Safe and effective vaccines would potentially considerably simplify the task of STI control programme managers. Unfortunately, hepatitis B is the only potentially sexually transmissible pathogen for which an effective vaccine is currently available,20 although recent report of an efficacious vaccine against human papillomavirus (HPV) is good news.21 The repeated failure to develop protective vaccines against herpes simplex virus has been particularly disappointing, although one large US study has shown protective efficacy against HSV-2 acquisition in the subgroup of women who were initially HSV-1 seronegative.22 A larger trial purposely targeting this population subgroup is under way, although the relevance for developing countries where HSV-1 infection is quasi-universal at young age is uncertain. Even assuming availability of good products, the practicalities of implementing vaccination programmes in the developing world would be formidable, not to mention the acceptability to the target populations and the issue of parental consent, in cases of vaccines that should be provided before entry into sexual life. Moreover, it could be feared that post-immunisation behaviour change, fuelled by a feeling of perceived invulnerability, could paradoxically increase the prevalence of STI for which a vaccine would not be readily available—for example, HIV.
Screening and case finding
Universal serological testing of antenatal clinic attenders for syphilis is recommended by the WHO and is one of the most cost effective health interventions available, although programmes are poorly implemented in many countries.23,24 Simple, point of care tests for syphilis, in a dipstick format, are now commercially available. Although currently more expensive than the rapid plasma regain (RPR) test, they are simpler to perform, and some do not require separation of serum. They have been shown to be highly sensitive and specific.25
Blood donors should be screened for at least hepatitis, syphilis, and HIV to protect recipients, and it may be possible to screen populations such as military recruits and company employees. In all cases, careful attention should be paid to patient confidentiality, counselling, and treatment.
There is an urgent need for simple and cheap diagnostic tests to identify women with asymptomatic or poorly symptomatic cervical infections, in order to avoid sequelae and reduce transmission. These should include women undergoing transcervical procedures (such as insertion of intrauterine devices in family planning, or uterine curettage in abortion clinics), or pregnant women, at risk of transmitting infections to their babies. Other vulnerable or high frequency transmitter groups such as adolescents and sex workers might also benefit from regular screening or case detection.26 A WHO advocated simple sociodemographic risk score which identifies women at greater risk of infection has been tried but it has a poor sensitivity and predictive value.27,28 The STD Diagnostic Initiative led by the WHO is promoting the development of rapid point of care (POC) tests and their evaluation in developing country settings.26 A recent modelling exercise supports the use of POC tests with even moderate performance in terms of sensitivity and specificity (around 50%) in situations where the delay in treatment would result in significant STI transmission.29
Promotion of appropriate treatment seeking behaviour and the role of the private sector
Surveys of health seeking behaviour in developing countries indicate that a substantial proportion of people with symptomatic STIs seek treatment in the informal or private sector, from traditional healers, unqualified practitioners, street drug vendors, and from pharmacists and private practitioners, and they will only attend formal public health services after alternative treatments have failed.30 Self medication is also popular in many settings.30–32 Patients seek care in the private sector for many reasons, including their greater accessibility and convenience, and the more confidential, less judgmental, and less stigmatising nature of the services.
Objective quality of care in the private sector is however difficult to assess because of the range of services offered and the difficulty in accessing practitioners for researchers. A study of private doctors in South Africa showed that fewer than one in 10 patients received adequate doses of antibiotics and in 75% of cases an incorrect drug was prescribed.33 Likewise, only 11% of pharmacy workers in the Gambia correctly cited the appropriate management of urethral discharge according to national guidelines, and less than 5% provided adequate treatment to “mystery shoppers,” despite stocking some of the required drugs. None of the cases of pelvic inflammatory disease or genital ulcers was adequately treated.34
It is possible to improve private sector management of STIs in developing countries. In Jamaica, seminars for public and private physicians and nurses led to an increase in knowledge concerning STI diagnosis. Most practitioners reported an increase in risk reduction counselling.35 Similar training for pharmacists in Nepal showed an increase of 45% in the correct syndromic treatment of urethritis. This figure dropped to 26% 9 months after the training, indicating the need for continued training and supervision.36 A study in Lima, Peru, using “mystery shoppers” for the evaluation of an intervention targeting pharmacists, showed improved recognition of male STI syndromes and a significant increase in counselling, but trained pharmacists still failed to recognise syndromes in women and provided ineffective treatment regimens.37
Another strategy to increase effective treatment of STIs is the use of pre-packaged therapy for syndromic treatment. A team in Uganda developed the “Clear Seven” kit for the management of men with urethral discharge. The kit contains ciprofloxacin, doxycycline, condoms, partner referral cards and an instruction leaflet, and was socially marketed at clinics, pharmacies, and retail drug shops. The study found that “Clear Seven” users versus controls had significantly higher self reported cure rates (84% v 47%), greater compliance (93% v 87%), and increased condom use during treatment (36% v 18%). Partner referral rates were similar for both groups (39 and 37%).38
The private sector should be viewed as a complement to, and not a replacement for, effective and accessible public services. The views of government health authorities and the medical community should be considered when attempting to stimulate effective collaboration between the two sectors.
STI case management
Early diagnosis and effective treatment of STIs is an essential component of STI control programmes.7 Syndromic case management is an approach based on the recognition of STI associated syndromes (easily identifiable group of symptoms and clinical findings), followed by treatment targeting the common causes of the syndrome. Management is simplified by the use of clinical flowcharts and standardised prescriptions. The approach is particularly suited to settings where diagnostic facilities will be either lacking or unreliable. Moreover, syndromic management leads to immediate treatment, and does not rely on the patient returning for results. It has proved generally to be cost effective, except for the management of women with cervical infections, in whom this simplified approach is neither sensitive nor specific.39,40 The advantages and disadvantages of syndromic management are shown in table 2.
Advantages and disadvantages of syndromic management of STIs
Syndromic management guidelines need to be adapted for local use, depending on the prevalent causes of the common syndromes, and the antimicrobial susceptibility of local isolates of Neisseria gonorrhoeae and Haemophilus ducreyi. A laboratory is needed to monitor these parameters, which may change rapidly.41
Partner notification and management
Partner notification and management “comprises those public health activities in which sexual partners of individuals with STI are notified, informed of their exposure and offered treatment and support services.”7 Partner management aims to reduce the prevalence of asymptomatic infection, and to shorten the average period of infectiousness. This in turn is expected to reduce disease transmission. However, while bacterial STIs can be identified and cured, thus breaking the chain of transmission, viral STIs such as HSV-2 and HIV are incurable, and the rationale for partner management is less clear. In the context of syndromic management, it is even more difficult to decide which partners should be treated, and for what. The most practical approach has been to give the same treatment as for the index case, but this will obviously result in over-prescription of antibiotics, especially in the case of partners of women with vaginal discharge, most of whom do not have an STI. In such circumstances, partner notification could potentially lead to serious social and physical consequences for the female index case.42
Partners may be reached actively (or “traced”) by health providers, or invited to clinics through provision of a “notification” slip to be remitted by the index case. While strongly recommended by STI experts as an integral component of STI control,7 little work has been done to assess the effectiveness of partner notification strategies,43 and their impact on reducing the prevalence and incidence of STIs in developing countries has never been properly demonstrated.42,43
Targeted interventions and periodic presumptive treatment
Targeted interventions are based on the concept of “core groups”—that is, groups of individuals who have much higher rates of sexual partnerships, and thus may be more likely to acquire and transmit STIs. These core groups and their sexual partners—who form “bridging populations” with the general population—have been shown to be epidemiologically important in driving the STI and HIV epidemics in many parts of the world.44,45 Core groups are context specific and when designing interventions it is important to take account of the social and economic forces creating the groups, and to balance disease control measures against the potential for victimisation. Several comprehensive sexual health interventions targeted at core groups have been conducted in developing countries and have demonstrated good impact on the STI and HIV rates among the target populations,46–49 and sometimes among their partners.15,45
A successful core group intervention in a South African mining community provided STI treatment services, including periodic (monthly) presumptive treatment with azithromycin, and prevention education to a group of female sex workers living around the mine. The intervention significantly reduced the prevalence of N gonorrhoeae and C trachomatis and genital ulcer disease (GUD) among the high risk women in the short term. Symptomatic STIs were also reduced among the miners in the intervention area compared to miners living further away.50 It is not clear, however, how long such interventions should be sustained, as STIs get quickly re-established in these highly exposed populations.51 Interestingly, a targeted mass treatment programme with azithromycin during a syphilis outbreak in Vancouver, Canada, resulted in a transient decrease of cases for 6 months followed by a rebound effect,52 a reminder that, even though feasible, such interventions should not be done routinely and only with caution.
Mass treatment
Mass treatment with penicillin was highly successful in the control of non-venereal treponematoses in the 1950s and 1960s.53 It has proved less effective in controlling STIs among the more mobile populations of developing countries in the 1990s.
A community randomised trial in the Rakai District of Uganda5 assessed the impact on prevalence and incidence of HIV and STI of single dose oral treatment of all adult community members with azithromycin, ciprofloxacin and metronidazole, combined with a single intramuscular penicillin injection for all participants with serological syphilis. Mass treatment was delivered every 10 months at the household level. After two rounds, the prevalence of serological syphilis was significantly lower in the intervention communities (5.6%) than in the comparison communities (6.8%). The prevalence of Trichomonas vaginalis infection in women was also significantly lower in the intervention communities (9.3% v 14.4%). There was, however, no significant difference in the prevalence of other STIs.5
Mathematical modelling suggests, however, that single or multiple rounds of mass treatment combined with continuous availability of syndromic management could be an effective STI and HIV control strategy for many countries.54 The comparative advantages of mass treatment and continuous provision of syndromic treatment could be determined through randomised controlled trials with STI services as standard provision in the control group.55
Individual, community and targeted intervention strategies, and structural approaches
An important consideration in STI control is to decide on strategies that target the individual, the community, or special groups of individuals at higher risk of, or more vulnerable to, STIs. Clearly, a number of strategies target the individual such as screening, case management, and partner notification; while community strategies will include mostly primary prevention activities, such as behavioural change and communication (BCC) campaigns, or vaccination programmes. Interventions targeted at individuals may fail to identify or influence behaviours of people who do not identify themselves with the target group. On the other hand, although general population or community measures deliver a less intensive dose of intervention to each individual, it is distributed across a large population that includes many individuals at low risk56 Clearly, HIV/STI control programmes need a mix of individual and general population interventions.8,56–58 The challenge is how best to use and combine them and how to make sure policy and political support help to change the social or physical environment in which risk takes place.
Structural factors relating to the economic, social, policy, organisational, or other aspects of the environment may act as barriers or facilitators of HIV/STI prevention.58,59 For example, restrictive policies about prostitution will hamper interventions targeting sex workers; sociocultural environments which promote homophobia or deny sexual health information to adolescents will prevent access of these vulnerable populations to appropriate sexual health services, or may encourage clandestine risk taking. On the other hand, economic empowerment of women, or other structural interventions may provide a more sustainable means of HIV/STI control by strengthening the ability of communities to help individuals reduce their risk.8,58,59
Impact of community based interventions on STI rates, including HIV, in developing countries
Three large scale randomised community based STI intervention trials have been conducted in east Africa. They provide some of the best empirical evidence of the impact of various STI intervention strategies in developing countries. A summary of STI incidence or prevalence outcomes in these trials is presented in table 3. Improved STI case management using the syndromic approach offered at primary healthcare facilities in Mwanza, Tanzania, reduced the incidence of HIV in the surrounding populations by nearly 40%,60 as well as reducing the prevalence and incidence of some key STIs.4 However, this effect was not seen in Rakai, Uganda, where periodic mass treatment did not impact on HIV acquisition rates, and only moderately on some of the STI rates.5 Initially it was thought that perhaps the difference in findings from these two trials was related in some way to differences in intervention type.55 However, recent findings from a three arm community based intervention trial in Masaka, Uganda, found that intensive information, education, and counselling (IEC) with (arm A) or without (arm B) improved STI syndromic management at primary healthcare centres also did not have an effect on HIV seroconversion rates compared to control communities (arm C). However, this trial demonstrated significant reductions in the prevalence and incidence of bacterial STIs in the syndromic treatment arm6 (table 3). These contrasting findings led to confusion over the role of STI control for HIV prevention. A detailed re analysis of the data from these three trials confirmed that it was differences in the populations rather than differences in the interventions which led to the different outcomes. The populations differed in sexual behaviour as well as in the prevalence of curable STIs, with much higher rates of bacterial infections in Tanzania.61
Summary of HIV and STI results in the three east African STI randomised community trials (differences in risk ratios (Rakai), rate ratios (Masaka) or relative risks (Mwanza) between intervention and comparison groups at follow up)
CHALLENGES IN STI CONTROL
Integration of STI prevention and care in reproductive health services and in HIV/AIDS control programmes
There is broad agreement on the need to integrate STI services into reproductive health services. The rationale is that, in some settings, reproductive health programmes are already high profile, and well attended, and could attract additional funds necessary for STI treatment. Moreover, integrated services could reach a wide female population. It has been suggested that at a minimum, STI/HIV risk assessment and prevention services should be provided in all maternal and family planning clinics, and that integrated services should also include syphilis testing and treatment for all pregnant women attending antenatal services.23 Integration of STI and reproductive health services can miss a key target group—men. This is important as men, because of sexual behaviour and increased mobility, are at higher risk, initially, of contracting STIs; and, once infected, their clinical management is simpler than that of women. Investigators in Bangladesh found that there was a substantial unmet need for STI services for men and that in addition there was a demand for other reproductive and psychosexual services.62
At the programme level, however, experience from several countries suggests that STI control programmes are probably best integrated within HIV/AIDS programmes to provide greater synergy, since both programmes share a number of control strategies from behavioural interventions to condom programming, and interventions targeted at high risk groups which would not usually be reached by conventional reproductive health services.
The changing epidemiology of STI
Additional challenges to STI control include the capacity of pathogens to develop resistance to antimicrobials, and the rapid emergence of some pathogens—for example, herpes simplex virus type 2 (HSV-2), as significant causes of morbidity and important cofactors of HIV transmission.
Global antimicrobial resistance of Neisseria gonorrhoeae
In most developing countries, a high proportion of isolates of Neisseria gonorrhoeae are resistant to common antibiotics such as penicillin, tetracycline or cotrimoxazole (fig 2).63 In order to provide effective treatment and prevent the transmission of resistant isolates, regimens need to be tailored to the prevalence of antimicrobial resistance in the locality. This in turn requires information on patterns of antimicrobial susceptibility. Many industrialised countries have programmes for N gonorrhoeae surveillance, but continuous susceptibility data have been lacking in most developing countries. This problem has been approached by the establishment of a global surveillance network—the gonococcal antimicrobial susceptibility programme (GASP), coordinated by WHO.63

Antimicrobial resistance of N gonorrhoeae in selected countries in the 1990s. (Source: Mayaud and McCormick.76)
The emergence of HSV-2 and the changing pattern of genital ulcer aetiologies
In countries where syphilis and chancroid were endemic, HSV-2 has traditionally been thought to be relatively less important as an aetiological agent of genital ulcer disease (GUD). This pattern is changing however.64 Recent studies have found that, while GUD attributable to HSV-2 infection is increasing, that caused by bacteria is decreasing in many areas. HSV-2 now typically represents 40–50% of detectable GUD aetiologies (fig 3). One consequence is that it may be necessary to revise the WHO guidelines for syndromic management of GUD to include anti-HSV treatment. Furthermore, prospective studies have shown that antecedent HSV-2 infection markedly increases the rate of HIV acquisition65–67 and/or transmission in serodiscordant couples.68 Because of the high incidence and prevalence of HSV-2 in many developing countries, effective interventions targeting HSV-2 are urgently needed. Several trials evaluating the feasibility and impact of episodic or suppressive treatment with acyclovir in terms of HIV acquisition and/or transmission are planned.69

{kind=link}
{kind=link}
{kind=link}
Proportion of genital herpes, or HSV-2 isolation, over time among patients with genital ulcers in selected sub-Saharan African settings. (Source Mayaud and McCormick.)76
Mobilising policy, priority setting, capacity building, and multisectoral approaches
The failure to control STIs in the past was not solely the result of antibiotic resistance or any emergent organisms, but simply the result of lack of political will to invest in appropriate control measures, scaling them up, and/or sustaining them. Many governments are reluctant to confront the STI and HIV epidemics and in many instances countries fail to prioritise activities in the face of severe financial and administrative constraints.70 There are problems in the effective implementation of control programmes because STIs are not just biological and medical problems, but also behavioural, social, political, and economic problems—many facets that have not been adequately addressed in the past. This realisation is slowly translating into more comprehensive approaches to STI control involving several disciplines and will require a multisectoral approach. However, there is an inherent contradiction with this approach, since spreading resources across programmes in many sectors risks stretching already scarce resources with negligible or even negative impact. An alternative approach for policy makers would be to implement a smaller, core set of interventions on a national scale and in this way provide a foundation for expansion of activities.70 It is also essential to build national capacity in areas that interact synergistically with STI case management to create an effective and sustainable approach to STI control. Training in all areas is essential and this needs to take place in a policy environment which enables managers to advocate policy changes which can improve and sustain the national capacity to implement an effective STI control programme.
CONCLUSIONS
The importance of STIs has been more widely recognised since the advent of the HIV/AIDS epidemic, and there is good evidence that their control can reduce HIV transmission. Although many cost effective tools such as condoms, effective drugs, and the syndromic approach to case management are already available for STI control, there is an urgent need for research into more interventions such as vaginal microbicides, vaccines, and behaviour change.
The essential components of the public health package recommended by the WHO for STI prevention and care71 are presented in box 2.
Box 2 Public health package for STI control: the key elements
-
Promotion of safer sexual behaviour and primary prevention
-
Condom programming—full range of activities from condom promotion to supply and distribution
-
Promotion of appropriate healthcare seeking behaviour
-
Integration of STI prevention and care into primary health care, reproductive healthcare facilities, private clinics, and others
-
Comprehensive STI case management (using syndromic approach)
-
Specific services for populations at high risk—such as female and male sex workers, adolescents, migrant populations, uniformed forces, and prisoners
-
Prevention and care of congenital syphilis and neonatal conjunctivitis
-
Early detection of symptomatic and asymptomatic infections
(Adapted from UNAIDS71)
These recommendations remain valid several years after such a package was first promoted, as few developing countries widely implement even the minimum component of comprehensive STI case management. Possible reasons for this are shown in box 3.
Box 3 Reasons why STI control programmes often fail in developing countries
-
Low priority for policy makers and planners in allocating resources because STI are perceived to result from discreditable behaviour
-
Failure to recognise the magnitude of the problem in the population
-
Failure to associate the diseases with serious complications and sequelae
-
Control efforts concentrated on symptomatic patients (usually men) and failing to identify asymptomatic individuals (commonly women) until complications develop
-
Lack of simple screening tests for cervical infections that could be used to screen women attending family planning, antenatal, or maternal and child health clinics
-
Service delivery through specialised STI healthcare facilities which provide inadequate coverage and tend to confer stigma
-
Treatment strategies focused on unrealistic requirements for definitive diagnosis rather than on practical decision making
-
Ineffective low cost antibiotics continuing to be used for reasons of economy
-
Little emphasis on educational and other efforts to prevent infection occurring in the first place, especially among adolescents in and out of school
-
Absence of authoritative guidance on a rational, practical, and well defined package of activities for prevention and care programmes
-
Lack of attention to structural issues which impact on STI transmission: poverty, literacy, conflict, repression of homosexuality and prostitution, societal attitudes to marginalised communities
The most pressing need now is to discover the reasons behind the failure to act on these recommendations, and to devise strategies for ensuring that effective STI control programmes are implemented in future. More information is also required on the cost effectiveness of the various activities recommended, to enable programme managers to set evidence based priorities; and operational research is needed to establish the best way to implement many of them on a large enough scale to help make a difference.
CONTRIBUTORS
Both authors have contributed entirely to the preparation of this manuscript.
REFERENCES
Footnotes
-
Conflict of interest: none declared.
-
Series editor: David Lewis
Linked Articles
- Brief Encounters