Article Text

Abstract
Background: Genital herpes (GH) is a common sexually transmitted infection. Novel tools for the control of GH (for example, tests and vaccines) are emerging, but optimal assessment of the cost effectiveness of such interventions requires scaled, preference based estimates of the impact of GH on health related quality of life.
Methods: We provided self administered interviews to 39 individuals with recurrent GH recruited from an STD clinic and a GH support group in southern Ontario, Canada. Health preference estimates were generated using visual analogue scales (VAS), a time-tradeoff approach (TTO) and the Health Utilities Index Mark-II (HUI-II). Quality of life was also assessed with the Recurrent Genital Herpes Quality of Life scale (RGHQoL).
Results: Average (SD) health values for asymptomatic and symptomatic genital herpes were 0.89 (0.21) and 0.89 (0.22) using TTO, and 0.76 (0.30) and 0.71 (0.30) using VAS. Health utility estimates generated with HUI-II for transient symptomatic and asymptomatic health states were 0.93 (0.08) and 0.80 (0.16). Log transformed health value estimates exhibited convergent validity when compared to RGHQoL, as did health utility estimates for symptomatic GH. Utility scores for symptomatic GH increased (improved) with increasing age; no other subject characteristic was predictive of preference weights.
Conclusions: Preference based measures of health related quality of life can be elicited with relative ease in the context of genital herpes, and preference weights are correlated with quality of life scores generated using the RGHQoL. Generation of preference weights will permit direct comparison of the economic attractiveness of herpes prevention interventions with that of other commonly available health interventions.
- GH, genital herpes
- HSV, herpes simplex virus
- HUI-II, Health Utilities Index Mark-II
- QALY, quality adjusted life year
- RGHQoL, Recurrent Genital Herpes Quality of Life scale
- TTO, time-tradeoff
- VAS, visual analogue scales
- quality of life
- genital herpes
Statistics from Altmetric.com
- GH, genital herpes
- HSV, herpes simplex virus
- HUI-II, Health Utilities Index Mark-II
- QALY, quality adjusted life year
- RGHQoL, Recurrent Genital Herpes Quality of Life scale
- TTO, time-tradeoff
- VAS, visual analogue scales
Genital herpes (GH) is a relapsing ulcerative genital disease caused by herpes simplex virus type 2 or 1.1 Herpes simplex viruses (HSV) are the most common cause of ulcerative genital disease in the developed world, and are increasingly recognised as important causes of disease in the developing world.1–3 The costs attributable to GH in the United States may be more than $1 billion annually.4
Recent years have seen the introduction of several novel tools for the prevention of GH, including innovative uses of antiviral drugs,5 and inexpensive screening tests that can be used to identify individuals with otherwise unrecognisable infections.6 Evidence now exists to support the use of condoms for prevention of HSV transmission.7 Further, a developmental conjugate HSV-2 vaccine has shown promise as a potential new tool for HSV-2 control.8
However, the decision to adopt disease prevention strategies depends not only on evidence of effectiveness, but on evidence of cost effectiveness (that is, the monetary and resource cost at which gains in health are obtained).9 The ability to directly compare the cost effectiveness of prevention measures requires that health benefits be quantified using a common metric, that captures both quality and quantity of life. Quality of life may be particularly relevant in diseases like GH that are unlikely to cause large reductions in life expectancy.10–12
The use of utilities (scaled, preference based measures of quality of life on a 0 to 1 scale) has been recommended for use in economic analysis of healthcare interventions.13 Utilities may be used as quality “weights” for survival time, and permit estimation of so called “quality adjusted survival.” Our objective in this study was to evaluate the use of several utility based tools for assessment of health related quality of life in a population of individuals with symptomatic GH. Because herpes control programmes may require that individuals with otherwise unrecognised GH be identified through the use of serological testing, we sought to estimate the impact on health related quality of life associated with both symptomatic and asymptomatic GH.14
METHODS
Subjects
Individuals were eligible for study participation if they were adults (>18 years old) with a self identified history of recurrent GH. Potential study participants were identified through a herpes support group in Toronto, Ontario, through a municipal sexually transmitted diseases clinic in Hamilton, Ontario, and through a sexual health information telephone line run by the Hamilton Department of Public Health and Community Services. Subjects who expressed an interest in completing the study instrument provided written informed consent. All subjects completing the study were reimbursed $25 (Canadian funds) for time and travel. The study was approved by the research ethics board of Hamilton Health Sciences and McMaster University.
Study instrument
The study instrument consisted of a four component questionnaire; non-proprietary components of the study instrument may be obtained from the author. The first component consisted of questions related to subject demographics and clinical features of GH (for example, recurrence frequency and medication use). The two subsequent components elicited health preferences using generic measures of health related quality of life as described below,15 while the final component of the instrument consisted of a disease specific quality of life instrument, the Recurrent Genital Herpes Quality of Life scale (RGHQoL)16 (used with kind permission of Dr Steven McKenna, Galen Research, Manchester, UK). The RGHQoL has been demonstrated to be a reliable instrument, with good internal consistency and responsiveness to change in disease severity.16 The instrument was self administered, but either the study investigator or a trained research assistant was available to provide assistance to subjects requiring clarification of questionnaire items.
Assessment of health preferences
Scaled, generic, preference based measures of health related quality of life are useful for comparison of health outcomes across disease states.15 We conceptualised the impact of GH on health related quality of life using two different constructs; health preferences were measured using different approaches for each construct.
In the first construct, GH was considered to be a single continuous health state, characterised by varying frequency of symptomatic outbreaks (causing physical discomfort and emotional distress), as well as anxiety related to potential transmission of disease to sex partners and complications of pregnancy. Gender specific vignettes for symptomatic and asymptomatic GH, based on published descriptions of the natural history of GH, were used to obtain health state values using both TTO and VAS.17,18
In our second construct, GH was conceptualised as two separate health states, both transient in nature: (i) a symptomatic GH health state in which individuals experienced anxiety as a result of anticipation of outbreaks, potential transmission of disease to sex partners, and complications of pregnancy; and (ii) an asymptomatic health state in which individuals acutely experienced the physical discomfort and emotional distress associated with a GH outbreak. Utility estimates for each of these states, and for the subject’s pre-GH health state, were elicited using the Health Utilities Index Mark-II (HUI-II),19 a health state classification system in which societal health preferences are considered to reflect the impact of disease on specific health domains (for example, pain, mobility, emotion). Subjects classify health with respect to each domain, and domain scores are then mathematically transformed to provide approximate societal utility estimates. In this case, repeated estimates were elicited for pain and emotion domains in the pre-GH health state, the symptomatic GH health state, and the asymptomatic GH health state.
Statistical analysis
Between individual differences in preference scores according to the presence or absence of demographic and disease features were assessed using the Wilcoxon rank sum test for categorical predictors, and using linear or log linear regression methods, as appropriate, for continuous predictors. Within individual differences in preference scores derived using different approaches, and according to the presence or absence of symptoms were assessed using the Wilcoxon signed rank test. As visual inspection revealed skewing of utility scores, correlation between scores obtained using different measures was assessed through calculation of Spearman correlation coefficients, and using least squares regression with log transformation of utility scores; convergent validity of preference measures was assessed through comparison of log transformed utilities with RGHQoL scores. In testing whether vignette based health value estimates were significantly different from 1, we used an alpha level of 0.025 and one sided p values. All other p values were two tailed, with an alpha level of 0.05.
RESULTS
Forty one individuals expressed an interest in study participation between July and November 2002. Of these, two individuals (both identified through the sexual health information line) subsequently declined to be interviewed. Characteristics of the 39 study participants are presented in table 1; most were GH support group members, were college educated, and had GH of several years’ duration. Individuals had experienced a wide range of recurrence frequencies in the past year; there was a significant association between ever having used suppressive antiviral therapy and recurrence number (p = 0.04).
Characteristics of the study population (n = 39)
Preference estimates generated using the three approaches described above are presented in table 2. Health values derived by both TTO and VAS scale were significantly less than 1 (that is, represented less than perfect health) for both symptomatic and asymptomatic vignettes (one sided p<0.001 for all comparisons).
Health state utilities and values
Values obtained using TTO and VAS were correlated for both symptomatic (Spearman’s ρ = 0.33, p = 0.04) and asymptomatic GH vignettes (Spearman’s ρ = 0.56, p = 0.003). Health values assigned to symptomatic vignettes were significantly lower than those assigned to asymptomatic vignettes when VAS were used (p = 0.002), but no difference was seen with TTO (p = 0.45).
Utility estimates derived using HUI-II were significantly lower for asymptomatic herpes infection than for the pre-herpes health state (p = 0.02), and were significantly lower for symptomatic GH than for the asymptomatic herpes state (p<0.001). No correlation was seen between utility estimates derived using HUI-II and health values derived using vignette based measures.
Least squares regression models demonstrated statistically significant relations between RGHQoL scores and log transformed health values, and between RGHQoL scores and utility estimates for symptomatic GH (table 3). The strongest correlation was between health values assigned to the symptomatic GH vignette via TTO; approximately one quarter of the variation in log transformed utility scores was explained by variation in RGHQoL scores.
Log-linear regression models evaluating the relation between health preference estimates and Recurrent Genital Herpes Quality of Life Scale scores
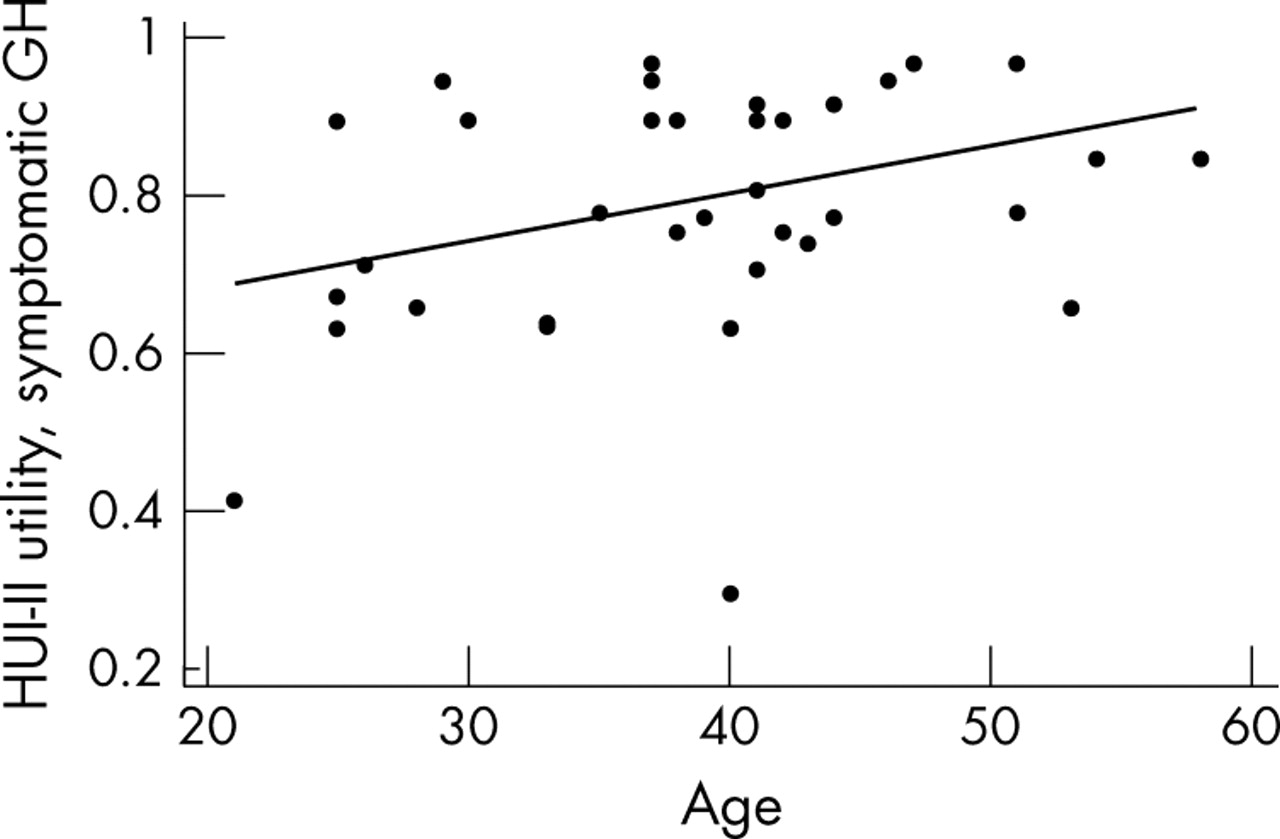
Subject characteristics were of limited value in predicting utility scores. Utility scores for symptomatic GH generated using the HUI-II were correlated with age, with less reduction in health related quality of life seen in older individuals (fig 1). A least squares regression model predicted an increase in utility score of 0.005 (95% CI 0.0004 to 0.011, p = 0.04) for each year increase in age. A trend towards higher utility scores generated using TTO with symptomatic GH vignettes was seen in individuals whose partners had herpes (p = 0.06 by Wilcoxon rank sum test). No other subject characteristic was predictive of utility scores.

{kind=link}
Scatter plot and least squares regression line illustrate the apparent improvement in utility of a transient symptomatic GH health state (estimated using a modified Health Utilities Index Mark-II) with increasing age.
DISCUSSION
Scaled, preference based measures of health related quality of life are commonly used to “quality adjust” survival estimates,15 and are useful in the context of economic analyses, where gains in health can be framed in terms of cost per quality adjusted life year (QALY) gained. We obtained estimates of health values (preference measures obtained under conditions of certainty) and utilities using three commonly utilised methodologies: TTO, VAS, and the use of a health state classification system (HUI-II).
These preference weights permit direct comparison of survival time in different health states, and of the economic attractiveness of interventions aimed at herpes control with the attractiveness of other disease control programmes. For example, our elicitation of preferences with TTO resulted in a value of 0.89 for symptomatic GH, higher than the weight of 0.81 previously assigned to symptomatic early HIV infection, but equal to the utility assigned to diabetes by a cohort of individuals living with that disease.20,21
In a previously published cost effectiveness analysis of screening for asymptomatic HSV-2 infection in asymptomatic, monogamous couples, we estimated that the cost per case of GH averted through screening would be $8200.14 Incorporating the HUI-II derived weights presented here into the same analysis, we would estimate the cost effectiveness ratio for serological screening in this context to be approximately $140 000 per quality adjusted life year gained. This ratio is higher than the $50 000–$100 000 per quality adjusted life year gained commonly cited as a cost effectiveness threshold in the North American context.22
In eliciting health values through the use of standardised vignettes, we found that respondents had a clear preference for asymptomatic health states, relative to symptomatic health states, when VAS were used. We were unable to find such a difference with TTO. Failure to find a meaningful difference between values assigned symptomatic and asymptomatic vignettes might suggest limitations in construct validity,23 or could reflect the impact of “time preference” on preference elicitation when TTO is used.24 However, the absence of a difference in health values might also indicate that, over the course of a lifelong infection, individuals focus more heavily on potential infection of partners and children than they do on their own intermittent symptoms.
We estimated utilities associated with transient symptomatic and asymptomatic GH health states using the HUI-II. This approach permits estimation of preference weights that incorporate the impact of relapse frequency on quality of life. The use such a health classification scheme provided preference weights higher than those obtained using VAS and TTO measures, even in individuals with high rates of GH recurrence. The generic nature of the HUI-II may limit the ability of this instrument to capture such herpes specific sources of disutility as fear of sexual intimacy or shame (that is, so called “construct under representation”).25
Given the abstract nature of health related quality of life, validation of measures may be problematic, at least in terms of establishing validity relative to a “gold standard” measure.26 None the less, we were able to demonstrate convergent validity between several of the preference based tools used here, and the RGHQoL, a disease specific instrument commonly used to assess the impact of GH on health related quality of life.16 Correlation between these measurements supports the credibility of preference based measures in GH, and also suggests that it may be possible to develop a schema that would permit conversion of RGHQoL scores into health value or utility weights, which would permit incorporation of previously collected RGHQoL data into cost utility analyses.27
Our finding that older individuals assigned higher utilities to symptomatic GH states that younger individuals could represent an instance of habituation to a chronic health state, a phenomenon that has been well described in the context of HIV infection.28 However, we found no differences in preference measures based on time since first diagnosis or outbreak frequency.
This study has several limitations, including its status as a pilot study with a limited sample size, and the fact that most participants were recruited from a GH support group. Additional work is needed to assess health preferences in individuals outside the context of support groups, and in individuals who have truly asymptomatic GH virus infection identified through serological testing.14 Finally, while some authors advocate the use of standard gamble as the method of choice for elicitation of health preferences, we avoided standard gamble because of difficulties in incorporating this cognitively complex technique into a self administered instrument.25
In summary, we have explored several possible methods for the elicitation of preference based measures of health related quality of life. Despite the complexities of the GH health state, elicitation of health preferences is feasible, and most measures used here displayed convergent validity with the current standard instrument for measurement of health related quality of life in individuals with GH. Further refinement of the methods presented here will provide insights into the impact of GH on quality of life, and will facilitate the economic evaluation of emerging tools for herpes prevention.
Acknowledgments
This project was conducted with the support of the Ontario Public Health Research, Education, and Development Program. The author wishes to express his gratitude to Supriya Mehta, Joe Mrus, Peter Sklar, Anne Davis, Galit Kleiner-Fisman, Jamie Jordan, Jennifer Warf, and an anonymous reviewer for their many useful insights related to this manuscript. The author thanks the City of Hamilton Sexually Transmitted Diseases Control Program, the Toronto Phoenix Group, Ms Lydia Napper, and Ms Miriam Kleiner, for their invaluable assistance in the conduct of this study.
CONTRIBUTOR DF developed the study instrument, obtained funding for this study, was responsible for the conduct of this research, performed all statistical analyses, and wrote and revised the manuscript.