Article Text

Abstract
Background: In sub-Saharan Africa, gonococcal and chlamydial infections are usually managed using the syndromic approach. However, many infections are asymptomatic in women, and the syndromic algorithm has poor sensitivity and specificity for infections caused by Neisseria gonorrhoeae (Ng) and Chlamydia trachomatis (Ct). Because of this, rapid point of care (POC) tests for Ct/Ng could improve sexually transmitted infection (STI) management in women. This study uses mathematical modelling to estimate the incremental cost effectiveness of using POC tests to diagnose Ng/Ct instead of the current syndromic approach used by the SIDA2 HIV/STI prevention project for female sex workers in Cotonou, Benin.
Methods: A dynamic mathematical model was used with data from Cotonou to estimate the HIV impact of the existing SIDA2 project (1995–8), and to project how impact would change if POC tests had been used. As observed in test evaluations, the POC tests were assumed to have high specificity, but a range of sensitivities. The incremental economic cost effectiveness of using POC tests was modelled using data on intervention costs and an evaluation of an Ng POC test in Cotonou in 2004. All costs were in 2004 $US.
Results: The model estimated the STI treatment aspect of the intervention averted 18 553 Ng/Ct and 359 HIV infections over 4 years when the syndromic approach was used. In contrast, if Ng/Ct had been diagnosed with a 70–80% sensitive and 95% specific POC test then 24–31% fewer clinic attenders would have been treated, 40–60% more Ng/Ct and HIV infections would have been averted, and the incremental cost effectiveness of using them would have been $107–151 per HIV infection averted if the POC tests cost $2 and $58–$81 if they cost $1.
Conclusions: POC tests can be a cost effective strategy for substantially increasing the impact on HIV transmission, and decreasing the degree of inappropriate treatment of STI treatment interventions that use syndromic management to diagnose Ng/Ct.
- Ct, Chlamydia trachomatis
- FSW, female sex worker
- GUD, genital ulcer disease
- Ng, Neisseria gonorrhoeae
- POC, point of care
- STI, sexually transmitted infections
- Benin
- sexually transmitted infections
- point of care tests
- mathematical modelling
Statistics from Altmetric.com
- Ct, Chlamydia trachomatis
- FSW, female sex worker
- GUD, genital ulcer disease
- Ng, Neisseria gonorrhoeae
- POC, point of care
- STI, sexually transmitted infections
The World Health Organization (WHO) estimates that 150 million Chlamydia trachomatis (Ct) and Neisseria gonorrhoeae (Ng) infections occur annually worldwide, the majority of them in developing countries.1 Untreated infection can cause serious long term complications, especially affecting the reproductive health of women.2,3 Both infections also facilitate HIV transmission.4
Gonococcal and chlamydial infections are usually managed using the syndromic approach in sub-Saharan Africa. However, this is of limited value in women because it is only applicable in the small proportion of women with symptoms,5,6 and even then it has poor sensitivity (30–80%) and specificity (40–80%).5–8 This results in many infected women not being treated, and in excessive overtreatment.5,9 This inappropriate treatment of women is a major concern both as resistance to treatment for Ng has become widespread,10 and because being diagnosed with a sexually transmitted infection (STI) can have serious social implications.11 A possible alternative to the syndromic approach is rapid point of care (POC) tests. Currently available POC tests for Ng and Ct are more specific (>90%) than the syndromic approach, but their sensitivity is variable (25-85%).12–15 Moderately sensitive POC tests could offer a significant improvement on the syndromic approach because of their greater specificity, and because they can be used to screen for asymptomatic infections.
To explore the likely role of POC tests in increasing the impact of targeted STI treatment interventions in sub-Saharan Africa, this study uses mathematical modelling, in combination with site specific data, to estimate the impact on Ng/Ct and HIV transmission of using a combined Ng/Ct POC test, instead of the syndromic approach, in the existing SIDA2 female sex worker (FSW) targeted STI/HIV prevention project in Cotonou, Benin.16 Firstly, the impact of the current intervention is estimated for FSWs, their clients, and the general population in Cotonou for 1995–8. Then further modelling is used to evaluate the likely incremental cost effectiveness of replacing the current syndromic algorithm for POC tests of high specificity, and a range of sensitivities.
METHODS
This study builds upon a previous analysis that used a dynamic model, Pop 1.0, to estimate the HIV impact of microbicide use in Cotonou and Johannesburg, South Africa.17 The model is described in full elsewhere,18 and this study uses the same model fits from the Cotonou analysis.17
Study population and SIDA2 project
Cotonou is the largest city of Benin, with an adult population of 310 000 in 1998. Nearly all men are circumcised.19 The main data source for the risk behaviour of the Cotonou general population is a population based study undertaken in 1998 (four city study).20,21 According to this study, the general population has few sexual partners.20 However, enumeration studies suggest approximately 1% of women sell sex, and 13–29% of men buy sex.21–23
There is a strong HIV prevention project in Cotonou, started by Project SIDA1 in 1993, and continued by SIDA2 in 1995 and SIDA3 in 2001. The intervention provides STI management for FSWs at a dedicated clinic, outreach services, and condom promotion. Outreach workers regularly visit FSW sites to carry out prevention activities, and to encourage FSWs to come to the project clinic for regular STI check ups, irrespective of symptoms.23 From 1996–8, approximately 200–250 FSWs attended the clinic per month,16,23 and received STI management and screening using a modified syndromic algorithm, based on clinical findings and microscopic examination of vaginal discharge.24 When evaluated among FSWs attending the SIDA2 clinic, the sensitivity and specificity of the algorithm for Ng/Ct was 48% and 75%.8
FSWs attending the intervention reported on average 52 clients per month in 1998, with condom use among clients in the last week increasing from 60% to 81% of sex acts from 1995 to 1998, but remaining low with regular sexual partners.16 Reported condom use in the general population is low (∼15% reported using condoms often with non-spousal partners).20
The overall HIV prevalence among FSWs from Cotonou in the four city study (1997–8) was 55%.21 However, among FSWs reached by the SIDA2 project, the HIV prevalence has been decreasing from 49% in 1995, to 41% in 1998 and 39% in 2002.16,25 The HIV prevalence is low in the general population, with ∼3% of adults being infected.16,26 Other STIs show a similar pattern, with 33% of FSWs attending the SIDA2 project being infected with Ng/Ct in 1995, whereas in 1998, 25% of FSWs and 8% of their clients were infected,16,26 and fewer than 3.5% of adults from the four city study were infected. The prevalence of genital ulcer disease (GUD) in Cotonou is low, with 2% of the clients of FSWs attending the SIDA2 project having GUD in 1998.16
Within the general population, individuals only seek STI treatment if they have symptoms. However, up to 80% of males and females with Ng/Ct do not have symptoms,27,28 and even when they have symptoms surveys suggest only half of men in Cotonou seek treatment from the health sector.28,29 Similar treatment seeking behaviour data does not exist for females from Cotonou. On attending a public STI clinic, symptomatic individuals are treated using syndromic algorithms.7 For Ng/Ct, the syndromic algorithm used at public clinics had a sensitivity and specificity of 91.5% and 60.3% among men, and 86.7% and 41.8% among women in 1993.7
Model description and parameterisation
A deterministic model (POP 1.0)18 was used to estimate the impact of the SIDA2 project on HIV/STI transmission among FSWs, their clients, and the general population. The aspects of the intervention incorporated in the model include STI treatment by the SIDA2 clinic and the increase in condom use reported by FSWs attending the intervention. Further details of the model can be found in the appendix, and a full model description was included in a previous study.18
The model was parameterised using context specific data on the risk behaviour of the Cotonou population and the different types of STI treatment (table 1). Other inputs, including the HIV/STI transmission probabilities,30–34 and STI co-factors4 were obtained from the scientific literature. Uncertainty bounds were estimated around all model inputs with a large degree of uncertainty associated with them.
Model input parameters used to obtain the baseline Cotonou model fits
Model fitting
Before using the model to estimate the impact of SIDA2, the model was fitted to available data on HIV, Ng/Ct, and GUD prevalences among FSWs and the general population from Cotonou for 1995–817 (appendix). Different model fits were obtained by randomly sampling different parameter sets from the parameter uncertainty bounds in table 1, and selecting any model simulation that lay within the uncertainty bounds of the STI and HIV prevalence data from 1995–8. Using least squares, the simulation that best fitted the epidemiological data was compared against available HIV prevalence data in a previous publication.17 All the model simulations that fitted the HIV/STI epidemiological data were used to estimate the likely impact of the SIDA2 project (mean projection from all model fits), and to generate uncertainty bounds around this estimate (shown in parentheses). A multilinear regression analysis of the inputs varied in the uncertainty analysis and resulting outputs of the model fits was used to determine which inputs caused most variation in the impact projections.
STI treatment interventions considered
The model simulations that fitted the epidemiological data from Cotonou were, firstly, used to consider the impact on HIV/STI transmission, over 4 years (1995–8), of the SIDA2 project, and then to estimate the added benefit of the STI treatment aspect of the intervention. This was evaluated by estimating how much the STI treatment component of SIDA2 added to the impact resulting from the observed increase in condom use. Following this, they were used to explore how the impact of the STI treatment aspect of the intervention would change if POC tests had been used to diagnose Ng/Ct, instead of the current syndromic algorithm. A number of scenarios were modelled, with POC tests having a range of sensitivities from 50%-80% but constant specificity of 95% (table 1). Lower sensitivities were not considered because they would have been below the sensitivity of the syndromic approach used by SIDA2 (48%), so resulting in a negative incremental impact. The specificity was not varied because currently available POC tests for Ct and Ng all have high specificity (92–100%12,15,35–37).
Incremental cost effectiveness of using POC tests
To evaluate the incremental cost effectiveness of using POC tests in the SIDA2 project, the additional economic costs of using the tests was modelled and divided by the projected increase in impact as a result of the POC tests. The additional economic cost of using POC tests, instead of the current syndromic algorithm, was modelled from the provider’s perspective. All costs, except test cost, were estimated from data obtained either from SIDA2 in 1998 or a recent evaluation of the PATH GC-Check POC test among FSWs in Cotonou.15 All costs were inflated to 2004 $US. Data from the GC-Check evaluation suggested two clinic staff would need to be trained to use the POC test, and each test would take an extra 15–20 minutes to undertake. Despite the availability of Ng and Ct POC tests,9,15 there is no available combined Ng/Ct POC test and so the incremental cost effectiveness was estimated for the test costing $1–4. Details of the cost model, and cost data are described in the appendix. The impact measures used were the additional number of HIV and Ng/Ct infections averted.
To understand the degree to which the cost parameters affect the incremental cost effectiveness projections, a univariate sensitivity analysis was undertaken with each cost parameter varying within a specified range. For these projections, the mean impact projection from the model fits was used to estimate the impact of a 70% sensitive POC test.
RESULTS
Impact of SIDA2 project
For 1995–8, the model projects SIDA2 resulted in a 17.6% (14.2–20.6%) reduction in HIV incidence among FSWs in Cotonou, and a 21.5% (17.7–24.9%) reduction in HIV incidence in the whole sexually active population. The projected drop in incidence resulted in 1523 (1176–1820) HIV infections averted over 4 years, 76.5% (73.5–81.3%) of which was because of the increase in condom use between FSWs and their clients and the rest was the result of the STI treatment undertaken by SIDA2.
On top of the impact achieved through the reported increase in condom use among FSWs, table 2 summarises the impact projections for the STI treatment aspect of the SIDA2 project. Over 4 years, the model estimated the project treated 3200 FSW clinic attenders for suspected Ng/Ct, of which 1339 (1181–1709) had Ng/Ct resulting in 18 553 (16 871–20 447) Ng/Ct infections averted. Over the same period, this resulted in the prevalence of Ng/Ct decreasing from 29.0% (25.6–36.9%) to 24.4% (20.8–32.3%) among FSWs, 10.2% (8.0–14.0%) to 8.7% (6.6–12.4%) among their clients, and 2.9% (1.9–4.4%) to 2.5% (1.6–3.9%) among the general population. This decrease in STI transmission resulted in a projected 359 (220-464) HIV infections averted—6.1% (3.9–7.8%) of the 5949 (4387–7062) HIV infections that would have occurred over this period without the STI intervention. The majority of HIV infections averted were among clients of FSWs (65%), with 235 (137–323) being averted from a total of 3210 (2212–4070) HIV infections. Lastly, the intervention averted 62 out of 1170 (1064–1228) HIV infections among FSWs.
Projected impact over 4 years (1995–8) of the STI treatment aspect of the SIDA2 HIV prevention intervention, for its current method of syndromic diagnosis and if it had used POC tests
The multilinear regression analysis suggests that 59% of the variation in the projected HIV infections averted by the STI treatment aspect of the project was because of uncertainty in the STI co-factors, mainly the Ng/Ct co-factor. Indeed, for every unit increase in the co-factor (varies from 3.9 to 8 in the different model fits) an estimated 41 extra HIV infections were averted. Parameters such as the HIV transmission probability, the frequency of sex in main partnerships, and the level of condom use in main and casual partnerships played the biggest part in explaining the remainder of the variation.
Impact of using POC tests
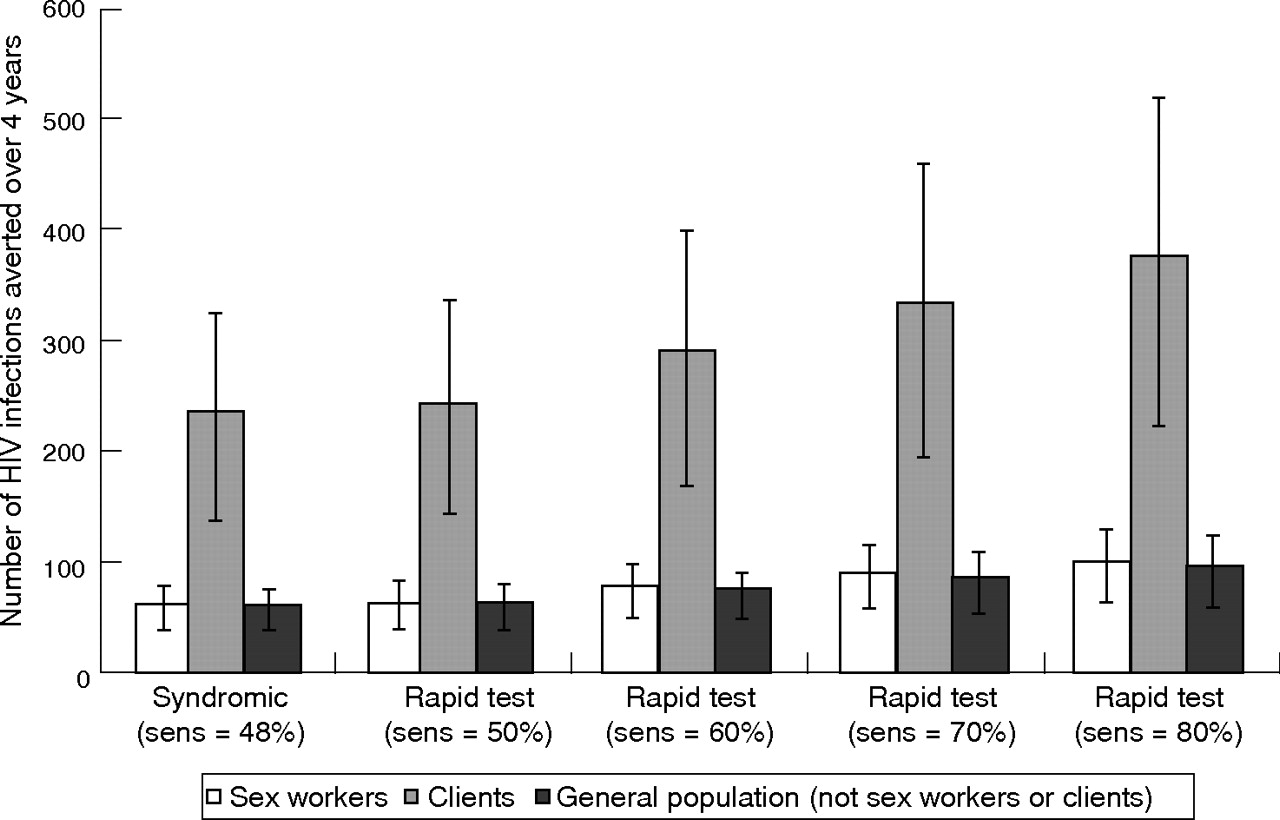
If SIDA2 had used POC tests to diagnose Ng/Ct, the increase in impact would have depended on the relative sensitivity of the test compared to the syndromic algorithm. This is shown in figure 1 and table 2 for the impact of the STI treatment component of SIDA2. For example, if the POC test had been 70% sensitive then 37.3% (35.9–39.0%) more Ng/Ct infections would have been treated and 42.0% (41.0–43.1%) more HIV infections would have been averted. In addition, the Ng/Ct prevalence would have decreased further, to 22.4% (18.8–30.4%) among FSWs, 8.0% (6.0–11.7%) among their clients, and 2.3% (1.5–3.7%) in the general population.

{kind=link}
Projected number of HIV infections averted in different population subgroups (over 4 years) resulting from using syndromic management or POC tests to diagnose and treat FSWs for Ng/Ct
Importantly, because the POC test has higher specificity than the current syndromic approach, the model projects it would have reduced the number of FSWs treated incorrectly by over 75% (table 2), and the total number treated by up to 45%. This decrease in inappropriate treatment results in a twofold increase in the number of Ng/Ct or HIV infections averted per clinic attender treated.
Incremental cost effectiveness of using POC tests
Assuming each test takes an extra 0.3 hours to undertake, the modelled incremental cost of using Ng/Ct POC tests for 4 years is $13 399 if the test cost $1 and $34 621 if the test cost $3 (in 2004 $US). The staff costs were estimated to be $2778, and the test costs varied from $10 550–$31 650 for the test costing $1–3. For different POC test costs and sensitivities table 3 shows the projected incremental cost effectiveness per HIV or Ng/Ct infection averted of using POC tests. The incremental cost effectiveness is highly dependent on the cost and sensitivity of the test. Specifically, an 80% sensitive POC test has a twofold to threefold improved cost effectiveness ratio than a 60% sensitive test, and the cost effectiveness ratio of a $2 test is about twofold worse than a $1 test.
Projected incremental cost effectiveness per Ng/Ct or HIV infection averted (for 1995–8 and in 2004 $US) of using POC tests (of different sensitivities) instead of the syndromic approach in the SIDA2 project in Cotonou
Table 4 shows the variations made in the cost parameters for the sensitivity analysis. All parameters, except salary costs, were varied to reflect the degree of uncertainty in those parameters. Salary costs were varied to show how the results might vary in a setting with different personnel costs. Compared to varying the test cost, other cost parameters have little effect on the projected incremental cost per HIV infection averted.
Model parameters varied in sensitivity analysis with resulting effect on the incremental cost per HIV infection averted (for 1995–8 and in 2004 $US) of using POC tests (70% sensitive POC test costing $2 per test) in the SIDA2 project in Cotonou
DISCUSSION
Previous studies have shown that rapid POC tests can have great public health impact in settings where gold standard laboratory tests are used to diagnose Ng/Ct.9,13 This is because patients can be treated at the first visit, so resolving the problem of patients not returning for treatment and the possibility of STI transmission during the treatment delay.
To explore the possible benefits of using POC tests in resource poor settings, this analysis used modelling to estimate the additional impact that could have been achieved by using POC tests to diagnose Ng/Ct in the SIDA2 HIV prevention project in Cotonou, Benin. The analysis showed that Ng/Ct POC tests of moderate sensitivity (>60%) could reduce Ng/Ct and HIV transmission significantly compared with the current SIDA2 protocol that uses a modified syndromic algorithm.
In addition, our projections also show that using POC tests would have dramatically decreased the number of women inappropriately treated—by over 75% if a 95% specific POC test had been used. This is an important advantage to using POC tests because they would substantially reduce the level of social harm resulting from incorrect STI diagnosis, and may reduce the rate of emergence of resistant Ng strains. The decrease in overtreatment would have also resulted in a dramatic increase in the intervention’s efficiency, as reflected in the projected incremental cost effectiveness of using POC tests in Cotonou. If the POC test cost $2 per test (2004 $US), and was 70% sensitive, then the model predicts the incremental cost effectiveness of using the POC test would have been $152 per additional HIV infection averted. This is as cost effective or more so than many other accepted STI/HIV prevention interventions in sub-Saharan Africa, including STI treatment for FSWs ($2300 per HIV infection averted in 2004 $US) and other populations ($298 per HIV infection averted), the prevention of mother to child transmission ($22–375 per HIV infection averted), and voluntary counselling and testing ($432–530 per HIV infection averted).18,38 If the cost of the POC test was $1 and the sensitivity was 80%, the cost per HIV infection averted would have been $58. This falls far below the suggested upper bound of cost effective interventions given by the World Development Report ($70 per DALY (disability adjusted life years) saved or ∼$1300 per HIV infection averted18).39 Indeed, only when the POC test has a low sensitivity, of 50%, is the intervention not cost effective when judged against these thresholds.
Importantly, the analysis shows that POC tests can be a cost effective strategy for increasing the impact of STI treatment interventions. Indeed, using an 80% sensitive POC test is equivalent to increasing the monthly coverage of the SIDA2 STI clinic by 77% (analysis not shown). This emphasises the importance of comparing the additional cost of using POC tests with the likely cost of increasing the intervention’s impact in other ways.
Irrespective of the diagnostic method used, over 80% of Ng/Ct and HIV infections averted by the STI treatment component of SIDA2 were among the clients of FSWs and the general population. The decrease in infections occurring in these populations is likely to have resulted in fewer people seeking treatment for HIV and Ng/Ct at public/private health clinics. Indeed, our model projects 7000 fewer people would have sought treatment from 1995–8 if an 80% sensitive POC test had been used. These wider savings are not featured in our cost effectiveness estimates.
The analysis has several limitations. The model projections are dependent upon the reliability of available epidemiological data, reported behavioural data, HIV/STI transmission and STI cofactor data. This uncertainty was factored into the analysis, and is reflected in the final conclusions. The model simulated the transmission of Ng/Ct together and so did not have separate cofactors for each STI. This may have reduced the accuracy of our projections. The model also assumed that all FSWs are equally likely to attend the intervention, and so the possibility that some FSWs were not reached by the intervention may have affected our projections. The effect of these limitations and parameter uncertainty is minimised by fitting and validating the model against available HIV/STI prevalence data from Cotonou. Lastly, the compartmental structure of the model may have resulted in it underestimating the effects of re-infection from untreated partners. However, considering most STI transmission occurs within transient commercial partnerships, this is likely to have a small effect on our projections.
The impact projections from this analysis are likely to apply to other communities with concentrated HIV epidemics—for example, India and China. If the intervention had been undertaken in a more generalised epidemic the intervention may have resulted in a smaller relative reduction in HIV incidence,40,41 and reduced the incremental cost effectiveness of using POC tests.18 The projected incremental cost effectiveness of POC tests is also dependent on the sensitivity of the syndromic algorithm used in a particular setting. This can vary widely depending on the algorithm and setting.5,18,42
The model projects the existing SIDA2 intervention reduced the HIV incidence in Cotonou by 21.5% (17.7–24.9%) from 1995–8. With an 80% sensitive POC test, this would have increased to 25.4% (19.7–28.7%). Although these impact projections are large compared to other HIV prevention interventions, it is less than the 40% reduction in HIV incidence recorded by the STI intervention trial in Mwanza.43 For the SIDA2 intervention to attain this level of impact, other strategies, in addition to using POC tests, need to be developed. These could include increasing the monthly coverage of the SIDA2 STI clinic, supplying STI treatment to their clients, or increasing condom use by FSWs. Indeed, a previous study has shown that the impact of FSW targeted STI treatment interventions can be substantially increased if they reach more FSWs per month, or supply STI treatment to their clients.18 Some of these strategies have been initiated by SIDA2 and SIDA3. Since 2000, FSW clients have been treated for STIs44 and condom use has increased further.45
CONCLUSION
Our findings add to the increasing evidence that moderately sensitive (>60%) POC tests can increase the impact of STI treatment interventions. Our study shows that POC tests can substantially increase the HIV impact and decrease the inappropriate treatment resulting from STI treatment interventions that use syndromic management to diagnose Ng/Ct. Indeed, our findings show that even if they cost up to $4 per test, they could be a cost effective use of resources for increasing the impact of STI treatment interventions in resource poor settings. This highlights the importance of evaluating currently available POC tests, of exploring the feasibility of using them in different settings, and of developing new POC tests.
Key messages
-
Compared to syndromic management (48% sensitivity), a moderately sensitive (>60%) POC test can substantially increase the impact on HIV and Ng/Ct transmission of STI treatment interventions focused towards sex workers. Most of the additional impact is among the clients of sex workers and the general population
-
Compared to syndromic management, POC tests can dramatically decrease the number of women inappropriately treated for Ng/Ct by over 75% if a 95% specific POC test is used instead of a 75% specific syndromic algorithm
-
Even at $4 per test, moderately sensitive (>60%) POC tests may be a highly cost effective strategy for increasing the impact of STI treatment interventions in resource poor settings. The additional cost of using POC tests should be compared against the likely cost of increasing the intervention’s impact in other ways
-
Even when highly sensitive POC tests are being used, sex worker targeted STI treatment interventions are only likely to result in large decreases in HIV incidence if high coverage levels among sex workers are achieved and STI treatment is also provided to clients
APPENDIX
MODEL DESCRIPTION
POP 1.0 is a deterministic compartmental model that can be used to simulate the transmission of HIV in different settings, and to estimate the impact of different HIV and STI prevention interventions on HIV/STI transmission among FSWs, their clients and the general population. The model divides the population into subgroups by level of sexual behaviour, condom use, and HIV/STI status, and simulates the transmission of HIV infection in the presence and absence of the SIDA2 project. Comparisons between the simulations are used to estimate the intervention’s impact in terms of Ng/Ct and HIV infections averted.
The model incorporates the effect of STIs in facilitating HIV transmission.1 If either partner has an STI then the HIV transmission probability per sex act is multiplied by the corresponding STI co-factor. For individuals with more than one STI, the STI cofactors are summed together. Owing to data limitations, specific STIs were not modelled but Ng/Ct and symptomatic ulcerative STIs were modelled as two separate STIs.2 When a susceptible individual becomes infected with an STI they remain infectious for an average number of days, with a constant daily probability of recovering, and then become susceptible and non-infectious once more.
The aspects of the intervention incorporated in to the model include STI treatment by the SIDA2 clinic and the increase in condom use reported by FSWs attending the intervention. The baseline level of condom use was assumed to be the level recorded by the intervention in 1993 and 1995 (60% of client acts protected with a condom) and then the model estimated the impact of the subsequent increase in condom use that occurred from 1995–8. This changed the level of condom use to 81% of client acts protected with a condom, and because of a lack of other data was assumed to occur from 1995 among all reached FSWs.
Different types of STI treatment are incorporated in the model. These include the SIDA clinic for symptomatic and asymptomatic FSWs and public/private STI clinics for individuals with STI symptoms. The treatment of STIs by the SIDA intervention (SIDA1 from 1993 and SIDA2 from 1995) started in 1993 but at a very low coverage (20 SWs seen per month). This increased to about 75 SWs per month later that year, but did not reach 200-250 FSWs per month until 1995-6. The model assumed that the SIDA1 STI treatment intervention started in 1993 but at a low coverage until 1995 (about 75 FSWs per month). For the SIDA2 clinic, 200–250 FSWs were assumed to attend per month from 1995 to 19983 and were diagnosed using a modified syndromic approach or POC tests. At the public/private STI clinics, about 50% of individuals with STI symptoms are assumed to seek treatment4,5 and these are managed using a syndromic algorithm. Along with the increase in condom use among FSWs, only the STI treatment undertaken at the SIDA2 clinic between 1995 and 1998 were included in our intervention impact projections.
METHODS USED TO FIT MODEL TO AVAILABLE EPIDEMIOLOGICAL DATA
For Cotonou, HIV prevalence data from 1995–8 for adult females from the four city study,4 antenatal clinic attenders,6 and from the SIDA2 project3,6 for FSWs and clients were used to fit the model. The model was also fitted to the STI prevalence data described in the study population sections. This amounted to four data points for the prevalence of Ng/Ct (1995 and 1998 for FSWs, 1998 for clients and 1998 for the general population), five data points for the prevalence of HIV (1995 and two data points for 1998 for FSWs, 1998 for clients, and 1998 for the general population), and two data points for the prevalence of GUD (1998 for clients and FSWs). The number of FSWs screened for STIs in the model was calibrated to agree with observed numbers of FSWs attending the SIDA2 clinic from 1995–8 (∼10 5006). HIV prevalence data for post-19987 and pre-19953,6,8 were compared against model projections.
To obtain different model fits, random sampling9 was used to obtain 1000 parameter sets from the model parameter uncertainty ranges. The model simulations that lay within the 95% confidence intervals of the model fitting data were selected. This produced 23 different model fits to the 11 HIV and STI data points used in the fitting process. The low number of model fits is to be expected because of the large uncertainty ranges associated with many of the model input parameters, and because of the large number of data points used in the model fitting. The input parameters for these model fits were mostly spread over the full uncertainty ranges for the model parameters. However, exceptions included the Ng/Ct co-factor (3.9–8.0) and GUD co-factor (4–13) for HIV transmission, the Ng/Ct transmission probability (0.15–0.35), the HIV transmission probability for males to females (0.0010–0.0018) and females to males (0.0006–0.0011), the high viraemia co-factor (11.4–18.6), the monthly number of clients per sex worker (41–51), the duration of sex work (40–53 months), the percentage of males that are clients (19–29%) and, lastly, the duration of Ng/Ct in the general population with treatment (2.3–6 months). In addition, despite the small number of fits some of the model inputs were significantly correlated with each other and the model impact projections. These included significant correlations between the HIV transmission probability for males to females and the FSW HIV prevalence; the HIV transmission probability for females to males and the proportion of males that do not use condoms with their casual partners; the Ng/Ct cofactor and the HIV infections averted; the proportion of women that use condoms all of the time with their casual partners and the FSW HIV prevalence; and the monthly number of clients per FSW and the proportion of males that have casual and/or commercial partnerships. Using least squares, the simulation that best fit the epidemiological data from Cotonou was obtained and compared against available epidemiological data in a previous study.10
METHODS USED TO ESTIMATE THE INCREMENTAL COST OF USING POC TESTS
The modelled costs of using POC tests included the possible cost of each test (Ctest per test), the estimated economic cost for the extra staff time needed to undertake each test (Δt in hours), and the projected training needs for the clinic staff using the tests (total cost Ctrain). The costs did not include the costs of buildings, resources, or staff that were already paid for by the intervention. In addition, any cost savings as a result of reduced treatment among FSWs attending the SIDA2 clinic (ΔN − FSWs treated) was also incorporated. However, only the cost of the drugs (Ctreat per person treated) were taken into account in estimating these savings. The formula for estimating the incremental cost (ΔC) was:
ΔC = n[Ctest + ΔtCstaff] + Ctrain − CtreatΔN
where n is the number of FSWs visiting the clinic from 1995 to 1998, and Cstaff is the hourly economic cost of the staff undertaking the POC tests. The training costs include the cost of the trainers, the time of the clinic staff, and the cost of materials used in the training. However, because the training for the PATH GC-Check POC test only took about 3 hours and was undertaken in the SIDA2 clinic, no costs for building rental, per diems, or refreshments were included in the training costs. Using a discount rate of 3%, all training costs were annualised over 1995–8. All salary costs were estimated using full salary cost data obtained from SIDA2 for 1998, and all costs except the estimated cost of the POC test were inflation corrected to 2004 $US using an average inflation rate of 3.2% per year.11
Between 1995 and 1998, there were approximately 10 500 visits to the SIDA2 clinic (n∼10 500 visits). The recent evaluation of the PATH GC-Check POC test in Cotonou estimated an extra 15–20 minutes would be needed to test each FSW when compared to the current syndromic algorithm (Δt = 0.25–0.33 hours). The full monthly cost to SIDA2 of the clinic staff that would undertake the POC testing was $118.6 per month in 1998, for a 37.5 hour week (Cstaff = $0.88 per hour in 2004 $US). If the combined Ng/Ct POC test was similar to the PATH GC-Check POC test, two clinic staff would need to be trained for about 3 hours to provide continuous testing over a 4 year period. The person undertaking the training for the PATH GC-Check POC test received the same wages as other clinic staff, and 50 POC tests were used during the training session (Ctrain = $70.7 to $253.8 depending on whether the test cost is $1 or $4). The training costs also includes the wage cost for the two clinic staff being trained. Possible cost savings to SIDA2 from using POC tests include the reduction in the number of STI clinic attenders receiving treatment (table 2). The cost of treatment for Ng/Ct in Cotonou was $1 per case in 1998 (Ctreat). Although no combined Ng/Ct POC test currently exists, POC tests for Ng and Ct do exist and currently cost between $2–7 (2004 $US). A lower cost range of $1–4 per test was used for the cost of a combined Ng/Ct POC test (Ctest) because tests of higher cost were not cost effective.
Acknowledgments
This research was funded by WHO/TDR. DM, CW, and PV also receive funding from the DFID funded AIDS Knowledge Programme. MA is a National Researcher of the Fonds de la Recherche en Santé du Québec (grant #8722). The views expressed are those of the authors and cannot be taken to reflect the official opinion of the London School of Hygiene and Tropical Medicine. The SIDA2 HIV/STI prevention project in Cotonou, Benin was funded by the Canadian International Development Agency.
CONTRIBUTORS PV participated in the planning of the analysis, collated already published and unpublished behavioural and epidemiological data for Cotonou, programmed the model, performed simulations and sensitivity analysis, analysed data, interpreted results and wrote the manuscript; MA, RWP, DM, and CW all helped in planning the analysis, interpreting the model results, and contributed to the manuscript. In addition, CW aided in the modeling analysis, RWP and DM had the initial idea for the study and gave continual expert advice, and MA collated published data from Cotonou, provided unpublished data and invaluable expertise.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.
- 32.
- 33.
- 34.↵
- 35.↵
- 36.
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.↵
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵