Article Text

Abstract
Background: Sexually transmitted infections (STI) and unprotected anal intercourse (UAI) have been increasing among men who have sex with men (MSM) in San Francisco. However, HIV incidence has stabilised.
Objectives: To describe recent trends in sexual risk behaviour, STI, and HIV incidence among MSM in San Francisco and to assess whether increases in HIV serosorting (that is, selective unprotected sex with partners of the same HIV status) may contribute to preventing further expansion of the epidemic.
Methods: The study applies an ecological approach and follows the principles of second generation HIV surveillance. Temporal trends in biological and behavioural measures among MSM were assessed using multiple pre-existing data sources: STI case reporting, prevention outreach programmatic data, and voluntary HIV counselling and testing data.
Results: Reported STI cases among MSM rose from 1998 through 2004, although the rate of increase slowed between 2002 and 2004. Rectal gonorrhoea cases increased from 157 to 389 while early syphilis increased from nine to 492. UAI increased overall from 1998 to 2004 (p<0.001) in community based surveys; however, UAI with partners of unknown HIV serostatus decreased overall (p<0.001) among HIV negative MSM, and among HIV positive MSM it declined from 30.7% in 2001 to a low of 21.0% in 2004 (p<0.001). Any UAI, receptive UAI, and insertive UAI with a known HIV positive partner decreased overall from 1998 to 2004 (p<0.001) among MSM seeking anonymous HIV testing and at the STI clinic testing programme. HIV incidence using the serological testing algorithm for recent HIV seroconversion (STARHS) peaked in 1999 at 4.1% at the anonymous testing sites and 4.8% at the STI clinic voluntary testing programme, with rates levelling off through 2004.
Conclusions: HIV incidence among MSM appears to have stabilised at a plateau following several years of resurgence. Increases in the selection of sexual partners of concordant HIV serostatus may be contributing to the stabilisation of the epidemic. However, current incidence rates of STI and HIV remain high. Moreover, a strategy of risk reduction by HIV serosorting can be severely limited by imperfect knowledge of one’s own and one’s partners’ serostatus.
- ATS, anonymous testing sites
- EIA, enzyme linked immunoassays
- MSM, men who have sex with men
- SAP, STOP AIDS Project
- SFDPH, San Francisco Department of Public Health
- STARHS, serological testing algorithm for recent HIV seroconversion
- STI, sexually transmitted infections
- UAI, unprotected anal intercourse
- men who have sex with men
- sexual risk behaviour
- sexually transmitted infections
- HIV
Statistics from Altmetric.com
- ATS, anonymous testing sites
- EIA, enzyme linked immunoassays
- MSM, men who have sex with men
- SAP, STOP AIDS Project
- SFDPH, San Francisco Department of Public Health
- STARHS, serological testing algorithm for recent HIV seroconversion
- STI, sexually transmitted infections
- UAI, unprotected anal intercourse
Data from communities of men who have sex with men (MSM) worldwide found increasing rates of sexual risk behaviour, sexually transmitted infections (STI), and HIV incidence during the late 1990s.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17 In San Francisco, we found concurrent rises in sexual risk behaviour, male rectal gonorrhoea, and HIV incidence among MSM.1–4
More recently, syphilis among MSM in San Francisco increased between 1997 and 2002, without a concomitant increase in recent HIV seroconversion.9 These paradoxical findings prompted further investigation of possible changes in the HIV epidemic, particularly whether a rise in STI transmission without a rise in HIV transmission might be explained by partner selection by HIV serostatus—that is, an increase in HIV serosorting.
On an individual level, the sexual practice of negotiated safety may directly impact HIV transmission.18,19 HIV seronegative concordant partners in a regular relationship agree to have unprotected anal intercourse (UAI), while negotiating condom use outside the relationship. On a community level, if a sufficient number of MSM select seroconcordant partners, there may be enough separation between unprotected sexual networks of HIV positive and HIV negative MSM to affect HIV incidence. Risk of STI transmission, however, might be greater in both sexual networks. The present study uses secondary analysis of multiple data sources to assess whether increases in HIV serosorting may contribute to preventing further expansion of the epidemic. In doing so, we update several trends in indicators used to monitor the HIV epidemic in San Francisco.1,20
METHODS
Study design
This report brings together pre-existing data from multiple sources. Findings are not the result of a single, purposefully designed study to answer a specific hypothesis but rather comprehensive interpretation of data collected for other purposes, including STI case reporting, voluntary HIV testing, and outreach education. Our approach is consistent with UNAIDS/WHO guidelines for second generation HIV surveillance in its use of multiple data sources to strengthen interpretation.21 The approach combines biological and behavioural measures with greater reliance on behavioural data to better understand factors driving the epidemic. We focus more on temporal trends and changes than on absolute levels of measures. Methods and data sources are similar to a previous publication.1
Data sources
STI surveillance
Annual numbers of rectal gonorrhoea and early syphilis cases among MSM originated from the San Francisco Department of Public Health (SFDPH) STI registry.3,22 Gonorrhoea and syphilis cases are reportable by law; however, negative test results are not, making it difficult to assess how changes in screening might affect case numbers. The municipal STI clinic accounts for the most cases citywide. Sexual orientation among syphilis cases was determined by medical history; male rectal gonorrhoea was considered a marker of male-male receptive UAI.1,3
Behavioural data from STOP AIDS Project
The STOP AIDS Project (SAP), a San Francisco community based organisation, conducts serial cross sectional surveys of MSM as part of outreach activities. Details of the methods have been described previously.1,2,22,23 Briefly, convenience samples were recruited at gay identified venues from July 1998 through December 2004 (n = 16 331: 2544 in 1998; 4102 in 1999; 2441 in 2000; 2252 in 2001; 1624 in 2002; 1792 in 2003; 1592 in 2004). The survey asks about sexual behaviours in the preceding 6 months, including UAI, HIV serostatus, and partners’ HIV serostatus. The main purpose is to identify potentially risky sex; therefore, respondents were only asked about UAI with partners of unknown serostatus. Sample questions include: “In the last six months, how many sexual partners did you have anal intercourse with?”; “Of these, how many did you have UAI with?”; and “Of these UAI partners, how many did you know their HIV status?”
This report focuses on UAI overall and UAI with one or more partners of unknown HIV serostatus (potentially serodiscordant UAI). Our definition of potentially serodiscordant UAI does not include situations where respondents knowingly had unprotected sex with people of opposite HIV serostatus, a possible felony in California.23 The exclusion of partner serostatus to avoid self incrimination would likely underestimate serodiscordant UAI.24
Behavioural data from HIV testing programmes
Data from all anonymous testing sites (ATS) in San Francisco and the municipal STI clinic’s voluntary HIV testing programme also provide risk behaviour measures which are routinely asked at pretest counselling. We tracked the proportion reporting UAI (any, insertive, and receptive) with a known HIV positive partner within the past 12 months. There were 20,589 MSM testers at ATS (2779 in 1998; 2681 in 1999; 3202 in 2000; 2949 in 2001; 2853 in 2002; 2852 in 2003; 3273 in 2004) and 8821 MSM testers at the STI clinic (725 in 1998; 1017 in 1999; 1360 in 2000; 977 in 2001; 1316 in 2002; 1519 in 2003; 1907 in 2004).
HIV incidence from HIV testing programmes
HIV incidence was estimated by the serological testing algorithm for recent HIV seroconversion (STARHS) following Centers for Disease Control and Prevention (CDC) protocols.25,26 STARHS identifies recent HIV seroconversions using two enzyme linked immunoassays (EIA), one sensitive to low HIV antibody levels and one made less sensitive by increasing specimen dilution and decreasing sample and conjugate incubation times. Serological specimens non-reactive by STARHS but reactive by standard EIA were classified as recently seroconverted, on average within the last 170 days (95% CI 145 to 200 days). Crude HIV incidence is estimated by dividing the number of people with recent infection by individuals at risk (recently infected plus uninfected). HIV incidence is annualised by the formula: crude incidence × ([365 days/170 days] × 100%].27
Specimens originated from the STI clinic (n = 8821, as above) and ATS (blood only; n = 11 772; 2180 in 1998; 1431 in 1999; 1804 in 2000; 1513 in 2001; 1626 in 2002; 1611 in 2003; 1607 in 2004). These sites account for two thirds of all tests performed from 2001 to 2004 by SFDPH. Of note, STARHS cannot be done using oral fluid specimens, which accounted for 13.6% of ATS specimens in 1998, 37.6% in 1999, 40.3% in 2000, 44.3% in 2001, 39.0% in 2002, 39.5% in 2003, and 48.0% in 2004. Even though oral fluid testers were less likely to be HIV positive (2.5% v 4.4%, p<0.001), the ratio of HIV positive blood to oral fluid specimens did not change significantly from 1998 to 2004 (p = 0.453).
Analysis
Our analytic approach involves inductive reasoning rather than statistical testing; that is the process of developing a hypothesis and searching for information that confirms, refutes, or modifies the hypothesis. The presentation and interpretation is descriptive of trends. Where applicable, we report p values for temporal trends using the Cochran-Armitage test.
RESULTS
Table 1 shows demographic characteristics of subjects from SAP and MSM seeking testing. A greater percentage of MSM testers were white and residents of San Francisco compared to SAP participants.
Demographic characteristics from the STOP AIDS project and HIV testing programmes in San Francisco, 1998–2004
From 1998 to 2004, there was an overall increase in subjects ages 40 and over (p<0.001) and a decrease in white MSM (p<0.001) at ATS, STI clinic, and SAP. Asian-American MSM increased at ATS and the STI clinic (p<0.001), while Hispanics increased at the STI clinic (p<0.001). African-American MSM increased at ATS (p<0.001) but decreased at the STI clinic (p = 0.02) and SAP (p = 0.002).
STI cases increased among MSM, as shown in table 2. Male rectal gonorrhoea and early syphilis cases increased from 1998 to 2004, though the increase slowed for syphilis from 2002 to 2004 (fig 1).
Trends in behavioural and biological measures of HIV risk, men who have sex with men, San Francisco, 1998 to 2004
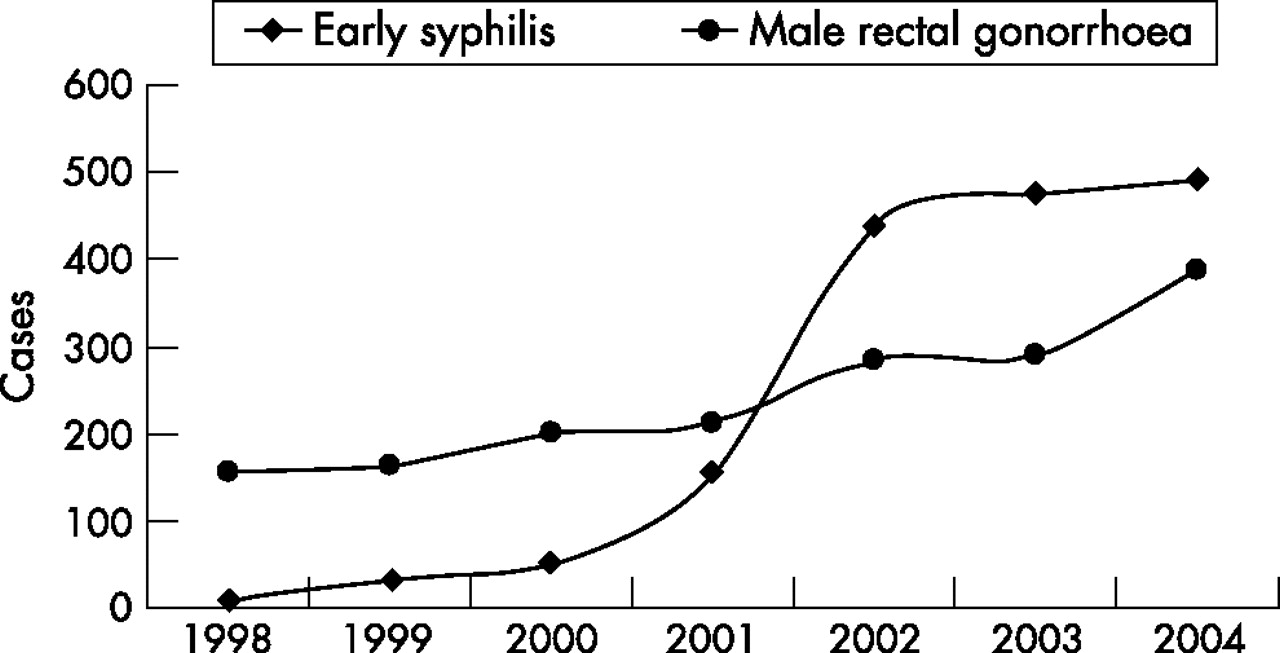
Early syphilis and rectal gonorrhoea among men who have sex with men, San Francisco, 1998–2003.
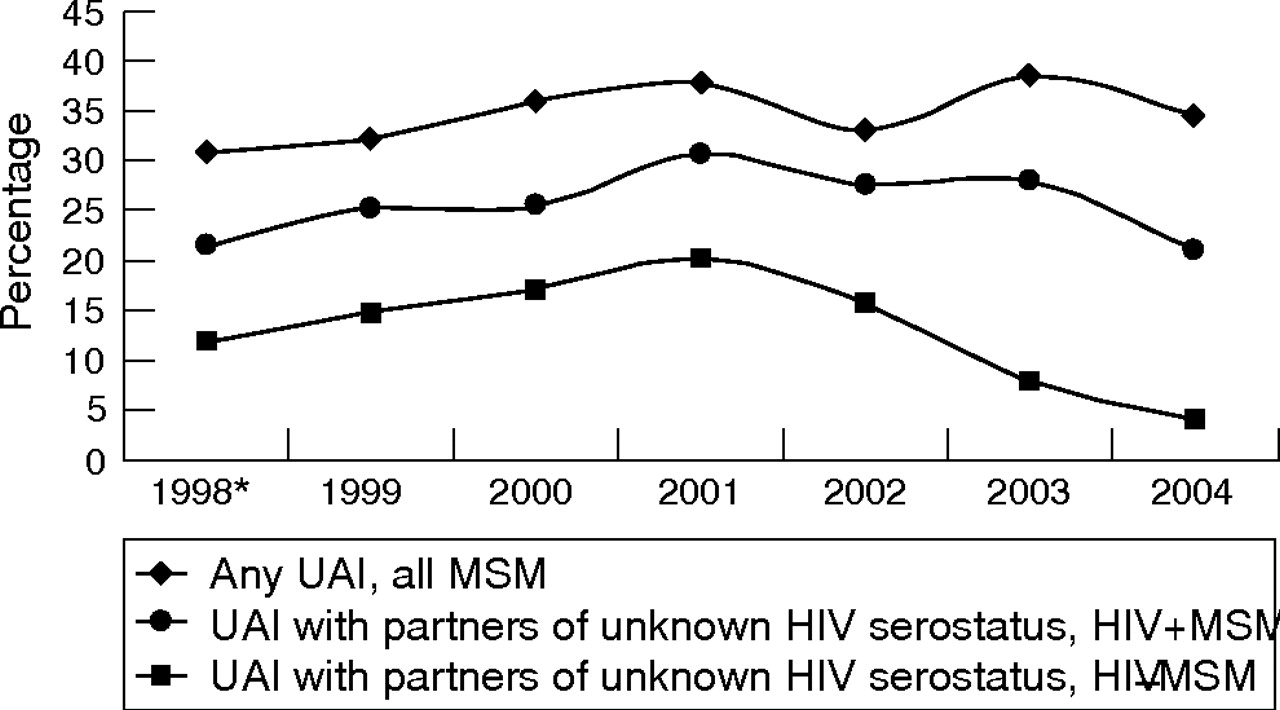
SAP data showed any UAI increased overall from 1998 through 2004 (p<0.001) (fig 2 and table 2). However, among HIV negative MSM, UAI with partners of unknown HIV serostatus decreased from 1998 to 2004 (p<0.001). Among HIV positive MSM, UAI with partners of unknown HIV serostatus declined from a peak of 30.7% in 2001 to a low of 21.0% in 2004 (p<0.001).
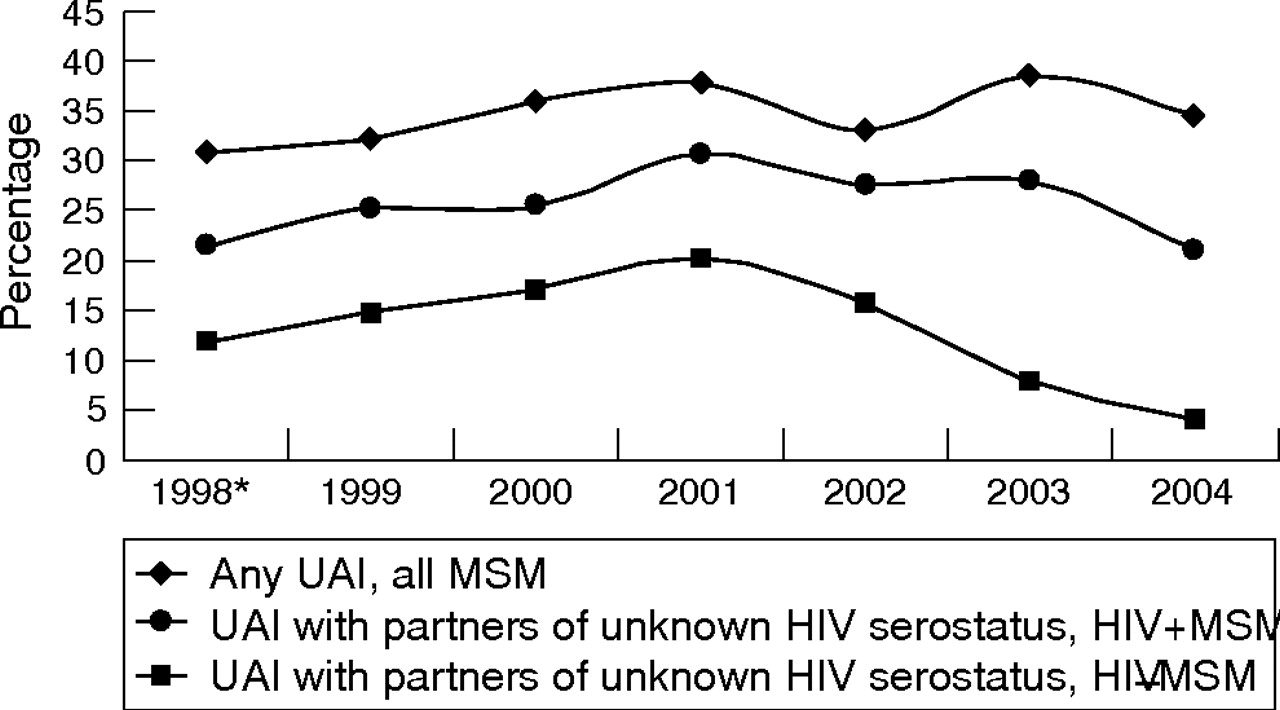
Men who have sex with men reporting unprotected anal intercourse (UAI) and UAI with any partner of unknown HIV serostatus by self reported HIV serostatus, The STOP AIDS Project, San Francisco, 1998–2004.
UAI with a known HIV positive partner among MSM testers is shown in figure 3 and table 2. At ATS from 1998 to 2004, there was an overall decrease in any, receptive, and insertive UAI (p<0.001), with the peak in 1999 and the low in 2002 for all three measures. A similar pattern is seen at the STI clinic where there was an overall decrease in any, receptive, and insertive UAI with a known HIV positive partner (p<0.001), with the peak in 1998 and the low in 2004 for all three measures.

(A) Men who have sex with men seeking HIV testing who report having unprotected anal intercourse (UAI) with a partner known to be HIV positive, anonymous testing sites (ATS), San Francisco, 1998–2004. (B) Men who have sex with men seeking HIV testing who report having unprotected anal intercourse (UAI) with a partner known to be HIV positive, STI clinic testing site, San Francisco, 1998–2004.
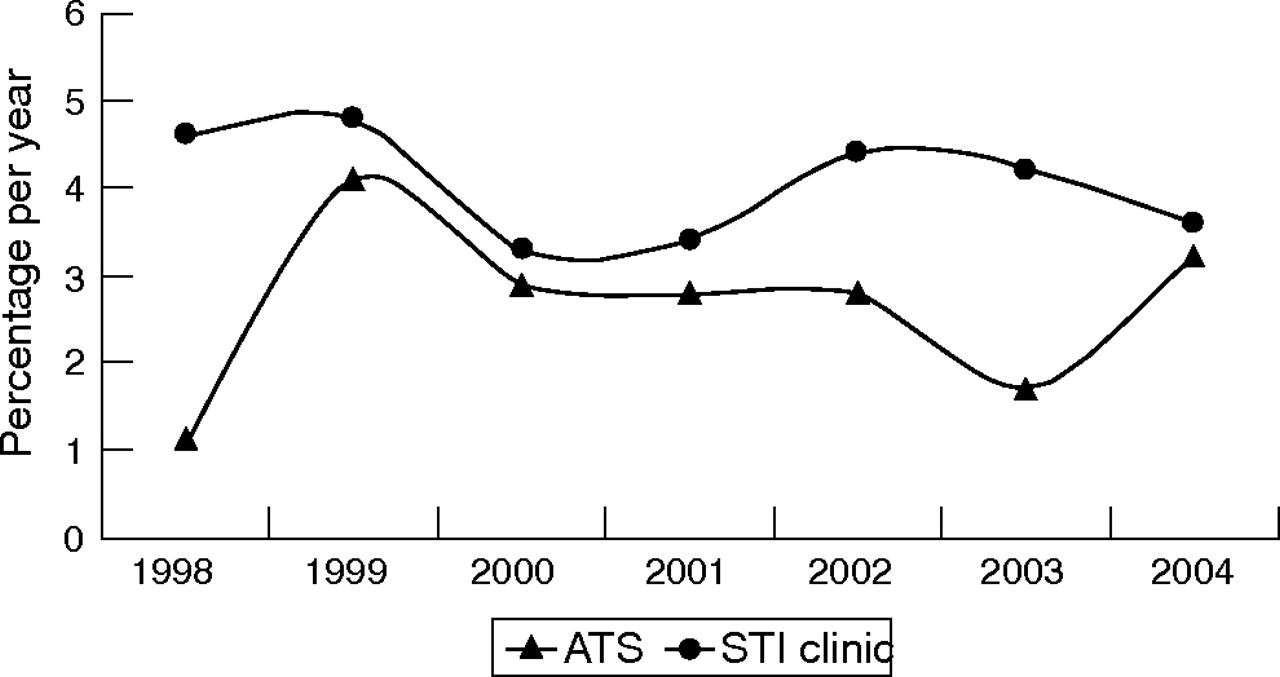
Based on STARHS testing, HIV incidence peaked in 1999 at 4.1% among MSM testers at ATS in San Francisco, then stabilised through 2004. HIV incidence also peaked in 1999 at 4.8% at the STI clinic (table 2 and fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
HIV incidence among men who have sex with men seeking testing, STI clinic and anonymous testing sites (ATS), San Francisco, 1998–2004.
DISCUSSION
Syphilis and male rectal gonorrhoea continued to rise even as HIV incidence levelled off among MSM. Our data support the hypothesis that MSM are increasingly selecting HIV seroconcordant partners when engaging in UAI. In the SAP data, although any UAI increased overall, UAI with partners of unknown serostatus declined among both HIV positive and HIV negative MSM. Behavioural data from ATS and the STI clinic showed an overall decrease in any UAI with known HIV positive partners during the same period. Overall prevalence of UAI with known HIV positive partners was similar between ATS (11.6%) and the STI clinic (11.0%). The decrease in UAI with HIV positive partners in recent years reflected a decline in both receptive and insertive UAI. Receptive UAI is thought to impart a higher HIV acquisition risk compared to insertive UAI, and the choice of HIV negative people as the insertive partner, referred to as strategic positioning (or “seropositioning”), may reflect a second strategy to decrease HIV risk.28,29
In aggregate, our data suggest the role of serosorting in preventing further increases in HIV transmission among MSM in San Francisco following a period of resurgent risk behaviour, STI, and HIV incidence.1–4,9,22 HIV incidence from two MSM populations seeking HIV testing remained at a relative plateau through 2004. While any UAI continued to increase overall, UAI with partners of unknown HIV serostatus has decreased since 2001. Our findings may be compared to data from Sydney where after 6 years of increases, HIV negative MSM reported decreases in UAI in 2003.30
Decreases in serodiscordant UAI suggest a recent shift in San Francisco’s prevention efforts may be working. The late 1990s saw initiation of “prevention for positives” programmes targeting secondary transmission.31,32 Prevention for positives activities included media campaigns, prevention messages integrated into HIV care, and support groups.
Other factors may contribute to the increase in serosorting. The internet may facilitate partner selection according to HIV serostatus by providing a semi-anonymous environment for disclosure.33–40 The internet has become the most common place where MSM diagnosed with STIs met their partners.41,42 Internet use was associated with a recent syphilis epidemic in San Francisco, where in 2002, 37.4% of MSM with early syphilis reported meeting partners on the internet compared to 12.2% in 2000.43
Widespread use of highly active antiretroviral therapy (HAART) may also contribute to the levelling off in HIV incidence by reducing the per contact probability of transmission.1,44–49 Mathematical models suggest a reduction in infectivity by HAART is in dynamic balance with risk behaviour.44,45,47 One model predicted if approximately 50% of HIV infected individuals receive HAART, a 20% or more increase in risky behaviour is likely to increase incidence of infection in the population.44 The model predicted population level HIV incidence would rise with HAART uptake in the San Francisco MSM community, but would subsequently fall as more HIV infected people received treatment or as risk behaviour decreased. A model to assess HIV infection among MSM in Amsterdam predicted even a 100% increase in risky behaviour with steady partners would not outweigh the protective effect of HAART if there were concurrent increases in HIV testing from 42% to 80%, and HAART coverage from 70% to 85%.48 The present study presents empirical data fulfilling these forecasts. HAART use rose rapidly from 1995 to 2001 but since has levelled off at a high coverage.1,49–51
We acknowledge alternative hypotheses could explain the current trends in STI, UAI, and HIV incidence. One possible explanation for the apparent discrepancy in STI and HIV incidence is that HAART has suppressed HIV transmission but not bacterial STI transmission.52 Another hypothesis is that transmission largely occurs immediately following HIV acquisition when viral loads are high and people unaware of their infection are in sexual networks of concurrent partnerships.53 In this hypothesis, serosorting by known HIV positive people would not have an important role in the epidemic. We believe these hypotheses are not mutually exclusive. HIV serosorting may account for some of the current trends in HIV and STI incidence or act in synergy with other causes.
We recognise limitations in our study. Firstly, the ecological nature of the analysis makes causal inferences uncertain. A limitation of the second generation HIV surveillance approach of using multiple data sources is that the temporal sequence of changes in trends is uncertain because of differences in the way data are collected across studies. Ideally, one would expect to observe decreases in sexual risk behaviour before declines in STI and HIV incidence. In our different datasets, however, HIV incidence peaked in 1999, UAI with a known HIV positive partner peaked in 1999 at ATS and in 1998 at the STI clinic, and UAI with unknown serostatus partners peaked in 2001. Another limitation is the data do not record biological and behavioural information from the same individuals, but rather from incompletely overlapping samples of MSM. A longitudinal cohort study of the same individuals would address this limitation; however, such studies have other potential biases and generalisation is problematic.54–56 None the less, evidence of a rise in STI, but not HIV, in an Amsterdam cohort of young MSM complements our findings.55
The potential biases of each data source must be considered separately. Part of our data include people seeking HIV testing.1,2 SAP data include MSM conveniently sampled at selected gay identified venues.1,2 HIV testing sites and gay bars may attract people at relatively higher risk for HIV. As with other serial cross sectional studies, we assume selection biases operating at the same locations remain relatively stable over time and therefore have less impact on interpreting trends over time than interpreting data at one point in time. A strength of our analysis is that we have several years of data collected consistently at the same locations. This is the basis for HIV sentinel surveillance as well as a principle of second generation HIV surveillance.21
Behavioural data rely on self report of sensitive information through brief public interviews. Moreover, there is great uncertainty around knowledge of partners’ HIV serostatus. Another limitation is in the interpretation of statistical tests, where an unknown proportion of subjects may be repeatedly included. When we excluded subjects known to be repeat observations, the main trends and findings did not change. The issues of under-diagnosis, under-reporting of cases, reporting delays, and changes in screening practices pose limitations to STI surveillance data. STARHS may not provide accurate estimates of HIV incidence because of severe immunosuppression, HAART use, or laboratory error.25,26 Finally, because data were collected during the course of clinical care or prevention activities, the level of detail on risk behaviour from all sources is limited.
On the other hand, drawing inference from multiple studies using different methods and populations may mitigate some of the limitations in interpreting each study separately. This is a primary strength of the second generation HIV surveillance approach.21 The same approach was quick to detect a rise in HIV risk in San Francisco several years ago, a trend corroborated by studies of MSM elsewhere in North America, Europe, and Australia.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17
The present data suggest a new phase of the epidemic where increased HIV serosorting may offset further expansion of HIV incidence. However, serosorting is vulnerable to imperfect knowledge of one’s own and one’s partners’ HIV serostatus and the transmission probabilities of sexual practices.28 A serosorting strategy may be more feasible in San Francisco because of the high level of HIV testing among MSM. A recent survey found 97% of MSM in San Francisco had ever tested and 34% had tested in the past 6 months.57 Although the data indicate HIV serosorting is a possible prevention strategy, it remains a hypothesis that needs validation in a specifically designed study. Such a study would need to measure true intentions to engage in HIV serosorting as a deliberate prevention strategy and longitudinal follow up would be needed to establish causality. While the findings of our analysis may point to potential further decreases in HIV transmission, HIV incidence among MSM in San Francisco has yet to decline to the point where the epidemic will be extinguished in the near future.
Key messages
-
Sexually transmitted infections are increasing among men who have sex with men (MSM)
-
Sexual risk behaviour—that is, unprotected anal intercourse is increasing among MSM
-
HIV incidence has levelled off among MSM
-
These findings may be explained by the increasing practice of “HIV serosorting”—that is, MSM are selecting sexual partners of the same HIV serostatus
CONTRIBUTORS
HMT participated in the development and design of the concept, analysis and interpretation of data, and drafting and revision of the manuscript; TK performed the statistical analysis and participated in the revision of the manuscript; JDK, JD, and BL participated in the collection and analysis of data and in the revision of the manuscript; MHK participated in the interpretation of data and revision of the manuscript; KK participated in the collection of data; SC and RP performed the statistical analysis; RMG contributed to the interpretation of data; WM contributed to the development and design of the concept, interpretation of data, and drafting and revision of the manuscript.
REFERENCES
Linked Articles
- Correction