Article Text

Abstract
Objectives: To determine which of the options available to modernise genitourinary medicine (GUM) clinics in the UK are most acceptable to patients and potential patients; to assess whether the views of a general population sample differ from those of clinic attenders. .
Methods: A questionnaire was used to explore the acceptability of different ways of delivering sexual healthcare including the potential trade-off between convenience/range of services with cost/staffing constraints. Potential differences in responses by age, sex, ethnicity and current attendance at a GUM clinic were evaluated using multivariate analysis.
Results: 542 respondents in the community and 202 clinic attenders provided responses. Delivery of sexual healthcare by specialist nurses and general practitioners was acceptable to 81% and 72% of interviewees, respectively, assuming common protocols were adhered to. The proportion of individuals who would accept a consultation with a nurse increased to 91% if the waiting time for an appointment could be reduced as a result. Men were less likely to accept a consultation with a nurse (odds ratio (OR) 0.52, 95% confidence interval (CI) 0.35 to 0.79), and Asian (OR 0.38, 95% CI 0.23 to 0.64) and other black (OR 0.41, 95% CI 0.2 to 0.87) ethnic groups were less likely to accept a consultation with a general practitioner. 44% of patients preferred walk-in clinics even if waiting times for an appointment were reduced to 48 h.
Conclusion: Delivery of sexual healthcare by nurses and general practitioners was generally found to be acceptable, although this varies by patient sex and ethnicity. Some differences exist between the preferences of a general population sample compared with clinic attenders, but overall there is a high level of concordance. Walk-in clinics remain a popular choice even when appointment waiting times are short.
- GUM, genitourinary medicine
Statistics from Altmetric.com
Rates of sexually transmitted infections and attendances at genitourinary medicine (GUM) clinics have increased over the past 5 years.1,2 Clinics have been encouraged to review how services are delivered and ensure the effective use of available resources. Various initiatives have been suggested, including the introduction of nurse-delivered services, use of telephone follow-up clinics, giving results by mobile phone texting and not contacting patients with results unless they are positive.3–5 It is important that the views of patients are sought as new ways of delivering services are introduced. Several potential factors may make it difficult to obtain patient involvement in sexual healthcare: patient embarrassment, language barriers in patients from ethnic minorities and a highly mobile population base. It may be equally if not more problematic to obtain the views of those who have not used sexual healthcare services but may need to in the future.
The need to increase capacity to cope with rising demand provides an impetus for changing clinic procedures. Historically, the decision to implement change has been largely subjective and made by the staff, not the patients. In other words, when deciding whether clinic procedure should change, do the clinic staff consider whether the proposed change will maintain the quality of the service at an acceptable level while being more efficient, thus allowing more patients to be seen? If this is the case, the change should be made. If, however, a change reduces costs but no longer delivers a satisfactory service, it would not be acceptable. Sometimes the decision needs to balance individual patient convenience or preferences against seeing larger number of patients and offering a shorter waiting time. Little is known about the views of patients on where this balance should lie. For example, would patients rather be seen quickly and see a nurse or general practitioner, or wait longer to see a specialist doctor? Previous studies suggest that the priorities of staff and patients in service provision may not be the same.6
Assessing views on service delivery may need to include the opinions of both service users and potential users. It is not clear whether the views of patients already attending a service accurately reflect those of the general population. Indeed those who attend a sexual healthcare clinic are self selected by finding the service acceptable enough to attend.
The views of two population groups—a sample from the general public and patients attending a GUM clinic—on alternative modes of service delivery were assessed in this study to help inform which aspects of modernisation are most acceptable.
METHODS
We assessed the views of participants on various aspects of sexual healthcare delivery using a questionnaire. Participants compared the acceptability of different options to reflect real-life decisions on balancing convenience/range of services with cost/staffing constraints. We developed the questionnaire in an internal workshop, with inputs from clinic research staff and a market research company. We did not validate the questions formally but piloted the questionnaire for 1 week before the start of the study.
We approached two population groups to participate in the study.
-
Community sample: We approached individual households in the Birmingham area, and a quota sample of those aged 16–25 years were invited to take part in the study at home. No more than one person participated in each household. The quota design increased recruitment of black Caribbean participants to 15–20% in order to adequately sample the views of this ethnic group which has historically higher rates of sexually transmitted infections.
-
Clinic sample: We approached a random selection of patients at a city centre GUM clinic aged 16–25 years after their registration but before being seen by medical or nursing staff. The interview took place in a side room away from the main waiting area to ensure privacy. We asked two additional questions of clinic patients (compared with the community sample) regarding previous attendance at the clinic (questionnaire available online at http://www.stijournals.com/supplemental).
All participants provided informed consent. We interviewed participants using a standardised questionnaire to assess the acceptability of different models of delivery of sexual healthcare services, including:
-
nurse-delivered GUM clinics (working to common protocols) compared with a specialist doctor clinic;
-
general practitioner-delivered services (working to common protocols) compared with a specialist doctor clinic;
-
patient charges for a rapid-access sexual healthcare clinic versus free care with longer waiting times; and
-
preferences for walk-in versus appointment-based sexual healthcare services.
Additional details on the methods are available online at http://www.stijournals.com/supplemental.
Analysis
We compared the response to each question between the two samples (clinic and community). Both are reported where they differed significantly, otherwise the overall values are reported. More generally, χ2 tests were used for univariate testing and multivariate analysis was based on multiple logistic regression. Adjusted odds ratios (ORs) are reported.
Minimum sample sizes of 500 community and 200 clinic interviews were set to ensure adequate precision, which allowed a population prevalence of 50% or 10% to be estimated within 5% or 3% in the community and within 7% or 5% in the clinic, respectively. For a binary risk factor with 50% prevalence, these sample sizes when combined for analysis also provide 80% power to detect ORs of 1.55 or 2.15 as significant when the prevalence of the outcome measure is 50% or 10%, respectively.
RESULTS
The community sample comprised 542 interviewees and the clinic sample 202 interviewees recruited between January and July 2005. In the community sample, 622 people invited to participate refused. However, accounting for the small proportion of interviews where a record of refusal was not taken, we estimate that around 707 people may have refused, leading to an overall response rate of 43%. In addition, 89 potential participants were identified as ineligible as they were unable to speak English. In the clinic sample, a total of 6417 patients were potentially eligible for the study. The exact acceptance rate was not recorded, but interviewers estimated that 220 patients were approached, giving a response rate of 92%.
Table 1 shows the demographics of the study population. Additional data are available online at http://www.stijournals.com/supplemental.
Demographics of the study population
We performed analyses with and without weighting the community sample for unequal selection probabilities (see Methods). No important differences in our findings were found and therefore only the unweighted results are reported.
Preferences between sexual healthcare delivered by specialist doctor and nurse
More than half (54% (n = 404), 95% CI 51% to 58%) of the respondents were happy to see either a doctor or nurse to receive their sexual healthcare, 29% (n = 217, 95% CI 26% to 33%) preferred to see a nurse within a sexual healthcare clinic and 17% (n = 123, 95% CI 14% to 19%) preferred a doctor. These figures were similar between the two samples. In multivariate analysis (fig 1), men were less likely to accept being seen by a nurse compared with women (OR 0.52, 95% CI 0.35 to 0.79). Among the clinic sample, first attenders were more likely to accept a consultation with a nurse than those attending for a follow-up appointment (OR 2.32, 95% CI 0.99 to 5.41).

Reported acceptance of sexual healthcare provided by a nurse (adjusted ORs). Bl, black; FU, follow-up.
Preferences between sexual healthcare delivered by a specialist doctor and a general practitioner
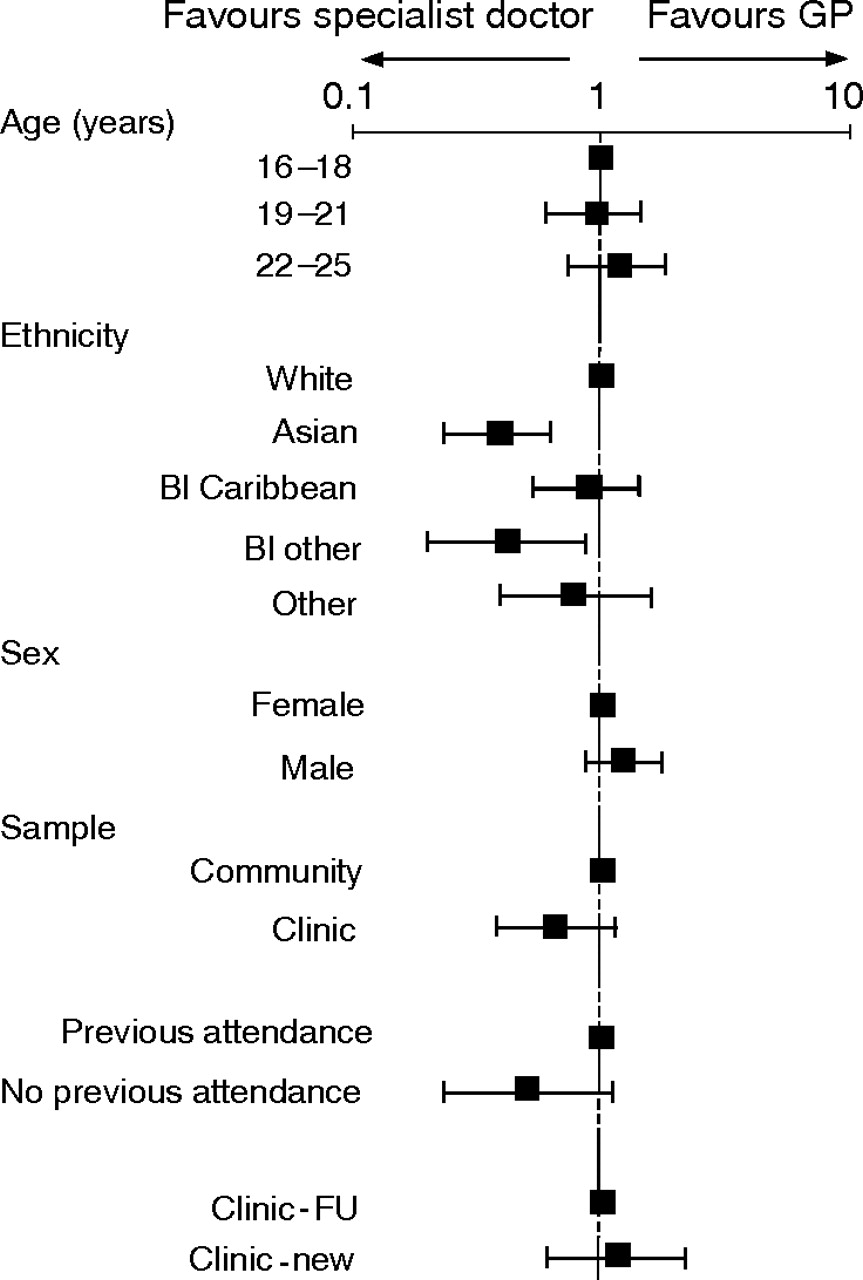
A similar proportion of respondents (54% (n = 402), 95% CI 50% to 58%) had no preference between seeing a general practitioner in their surgery for their sexual healthcare consultation compared with seeing a specialist doctor at a sexual healthcare clinic, and again these figures differed little between samples. A total of 18% (n = 136, 95% CI 16% to 21%) preferred to see their general practitioner whereas 28% (n = 206, 95% CI 24% to 31%) preferred a specialist. Those of Asian ethnicity (OR 0.38, 95% CI 0.23 to 0.61) and black other ethnicity (0.41, 95% CI 0.2 to 0.87) were less likely to wish to see their general practitioner (fig 2).
{kind=link}
{kind=link}
Reported acceptance of sexual healthcare provided by a general practitioner (adjusted ORs). Bl, black, FU, follow-up; GP, general practitioner.
Charging patients to be seen at sexual healthcare clinics
About 80% of clinic and 60% of community participants reported that a charge of £5 was acceptable if it led to being offered an appointment within 48 h. There was no difference in the acceptance of payment on whether the consultation was with a doctor (64% (n = 346) from community v 82% (n = 166) in clinic participants) or nurse (59% (n = 317) v 78% (n = 157)). This difference in reporting between clinic and community participants was not sustained in multivariate analysis. In all, 90% (n = 111) of those attending the clinic for the first time reported that paying £5 for a more rapid appointment with a doctor would be acceptable (OR 3.08, 95% CI 1.36 to 6.98). No differences in willingness to pay for a more rapid sexual healthcare consultation were found according to age, ethnicity or sex on multivariate analysis (data not shown).
Preferences between walk-in clinics and appointment-based clinics
A substantial minority of patients (44% (n = 326), 95% CI 40% to 47%) preferred a walk-in clinic, with a wait of up to 2 h to be seen, even when the alternative was an appointment within 48 h. The preference for a walk-in clinic increased as the wait for an appointment lengthened—61% (n = 454, 95% CI 57% to 65%) for a 1-week wait and 76% (n = 565, 95% CI 73% to 79%) for a 3-week wait. If the respondent had genital symptoms (pain or genital discharge) then 85% (n = 635) preferred a walk-in clinic rather than a wait of 48 h for an appointment. We found no significant differences in responses between the community and clinic interviewees—46% (n = 247) of the community sample versus 39% (n = 79) of the clinic sample preferred a walk-in service even if a 48-h appointment was available (p = 0.11).
Differences in responses between community and clinic interviewees
Those interviewed in the community or in the clinic showed no difference in their preferences for being seen by a doctor, nurse or general practitioner (figs 1, 2). Community respondents, however, preferred to see a doctor even if waiting times were shorter for a consultation with a nurse—if waiting times could be reduced from 2 weeks to 1 week then 75% (n = 152) of the clinic sample preferred to see a nurse and only 5% (n = 9) would wait a longer time to see a doctor, compared with 48% (n = 260) and 11% (n = 57) of the community respondents, respectively (p<0.001).
DISCUSSION
Through a large community-based and clinic-based study we found that the delivery of sexual healthcare by nursing staff and general practitioners was acceptable to most existing patients and potential patients, assuming that common protocols are adhered to.
Much sexual healthcare is already delivered by nurses7–9 with high levels of patient satisfaction,10,11 and this proportion is likely to continue increasing. Men were less happy with nurse-delivered services than women, which may reflect a preference to be examined by a healthcare professional of the same sex and the high proportion of female nursing staff. Alternatively, it may reflect inaccurate male preconceptions regarding nursing expertise which this study was not designed to explore.8
Although most interviewees reported a consultation with a general practitioner to be an acceptable alternative to seeing a sexual healthcare specialist, those from Asian or other black ethnic groups were less likely to do so. Smaller social and ethnic groupings may have particular concerns about stigma, discrimination and confidentiality,12 which could reduce the perceived acceptability of a consultation with a general practitioner. It has also been reported that Asian women prefer to obtain sexual healthcare from outside their Asian community,13 which could result in reluctance to see a local general practitioner. Patients were given the option of seeing their general practitioner rather than a general practitioner. The current healthcare service reforms in the UK will result in specialist general practitioners seeing patients who may be referred from other general practitioners.14 This may be more acceptable to those with concerns about confidentiality or who feel embarrassed about seeing their own general practitioner. Our findings reinforce the need to consider particular concerns about confidentiality and the perceived relevance of services to particular ethnic groups, taking into account their cultural, social and economic circumstances.15
Even if access to GUM clinics were available in 48 h, a large number of patients (44%) preferred a walk-in service with a wait of up to 2 h to be seen. Others have also suggested that patients are willing to spend longer in a clinic to obtain the service they want.16 GUM clinics in the UK have found it more and more difficult to offer a walk-in service following increasing patient demand, and the number of walk-in services has declined.17,18 These results suggest that the option of a walk-in service is valued by patients and should be reviewed if overall national service provision can be increased to cope with demand.
Many surveys have assessed patient preferences for the delivery of their healthcare. Their major limitation is the exclusion of people who have not accessed the service—that is, potential patients. In designing or modifying a clinical service, it is not known whether the views of current patients reflect those of the population who may wish to access the service in the future, and indeed patients are self-selected by their attendance at a clinic. Our study suggests that the experience of being a patient may have altered the views of interviewees. Attendance at the clinic was associated with greater acceptance of a nurse-based consultation compared to the general population sample, assuming the waiting time could be reduced as a result. Patients also reported paying for quicker access to care to be more acceptable than the community sample, although this was not sustained on multivariate analysis.
Key messages
-
Sexual healthcare delivered by nurses and general practitioners is generally acceptable to patients and potential future patients.
-
Nurse-delivered sexual healthcare is less acceptable to men.
-
General practitioner-delivered sexual healthcare is less acceptable to Asian and other black ethnic groups.
-
Walk-in sexual healthcare services are in high demand even if appointment waiting times are reduced to 48 h.
The strengths of our study are its large sample size and inclusion of samples from both patients and the community. The results are therefore likely to be generalisable to a wide population base. The presentation of alternative scenarios to patients, rather than just asking what services they wanted, more truly reflects the choices which those running a service have to make and provides realistic patient input into service design.
The weaknesses of the study include the need to make several assumptions to provide a quantitative measurement of patient preferences. The relative reduction in waiting times that would result from the increased use of nurse or general practitioner clinics is likely to vary in different clinical settings, as will the length of time waiting to be seen at a walk-in clinic. Thus the scenarios presented to respondents may not be representative of all clinic settings. Respondents from both the clinic and the community had fewer Asian respondents compared with the general population in the region. This may reflect a lower attendance rate at GUM clinics of Asian patients,[19] and in the community this could in part reflect a higher refusal rate. No formal record of refusals by ethnic group was made, but anecdotally interviewers suggested a possibly higher refusal rate among Asian women. We acknowledge the possibility of some bias arising as a result of these refusals and the ineligibility of those unable to speak English, particularly in the community sample where the response rate was only 43%. Only a small number of clinic patients were sampled, but their sex, ethnicity and type of clinic appointment did not differ from non-study patients attending the clinic over the same period. It is also not known whether expressed preferences of respondents will accurately reflect their actual behaviour.
We have shown a high level of acceptance from existing patients and from a general population sample for sexual healthcare delivered by nurses and general practitioners, assuming that common standards of practice can be delivered. The creation of common guidelines and protocols, the appropriate education of healthcare professionals and the introduction of a clinical governance framework to maintain agreed standards would therefore be appropriate next steps to facilitate the diversification of sexual healthcare delivery. The high demand for walk-in services should also influence the future design of clinics. Future questions include identifying the optimal proportion of patients that should be seen by the different healthcare professionals, assessing the cost effectiveness of sexual healthcare services delivered by nurses and general practitioners, and estimating the effect on waiting times at the GUM clinic.
Acknowledgments
We thank Rebecca Newson, Debbie Goddard and Charlotte Gough for their assistance in recruiting patients for this study.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 6 June 2006
-
Funding: This study was supported by Heart of Birmingham tPCT.
-
Competing interests: JDCR and AC are associate editors of Sexually Transmitted Infections.
-
Ethics approval: Ethical approval was obtained for the study from South Birmingham LREC.
Contributors: JDCR: study concept, design, study management, manuscript preparation; AC: design, data analysis, manuscript preparation; JS: design, manuscript preparation; LF: data collection, study management; GG: data collection, study management.