Article Text

Abstract
Objectives: To evaluate the Neisseria gonorrhoeae Becton Dickinson (BD) ProbeTec strand displacement assay (SDA) on female endocervical swab and male first void urine against culture for Neisseria gonorrhoeae on female endocervical and urethral swab for the diagnosis of N gonorrhoeae infection in genitourinary medicine (GUM) attendees. To determine an algorithm for implementation of N gonorrhoeae infection screening by SDA in these patients taking account of the desirability of having a N gonorrhoeae isolate in people with N gonorrhoeae infection.
Methods: Initially, 1582 patients attending the GUM clinic were tested for N gonorrhoeae infection by SDA and routine microscopy, and culture. On the basis of the results, a protocol for diagnosis of N gonorrhoeae infection by SDA, with culture specimens only from patients with a listed risk factor for acquiring N gonorrhoeae infection, was devised and implemented. A post implementation audit was done to assess the effectiveness of this protocol for routine service use.
Results: There was good concurrence between the N gonorrhoeae SDA and culture results with a N gonorrhoeae infection prevalence rate of 3.4% by both methods. All men and 85% of women with N gonorrhoeae infection had an identifiable risk factor for acquiring infection. Overall, 38% men and 60% women attending the GUM clinic had this listed risk factor for acquiring N gonorrhoeae. Post implementation audit confirmed the initial findings.
Conclusion: Nucleic acid amplification techniques like the SDA are sensitive and specific for diagnosis of N gonorrhoeae. We were able to list certain risk factors, which were predictive of those patients most likely to have N gonorrhoeae infection. To obtain timely sensitivity data, a culture specimen should also be submitted at the same time from patients deemed to have a listed risk factor for acquiring Neisseria gonorrhoeae infection.
- BD, Becton Dickinson
- FVU, first void urine
- GUM, genitourinary medicine
- NAAT, nucleic acid amplification technique
- SDA, strand-displacement assay
Statistics from Altmetric.com
- BD, Becton Dickinson
- FVU, first void urine
- GUM, genitourinary medicine
- NAAT, nucleic acid amplification technique
- SDA, strand-displacement assay
Although there has been a recent downward trend in the incidence of gonorrhoea (infection with Neisseria gonorrhoeae), it remains a significant problem, being the second most common bacterial, sexually transmitted infection (STI) after chlamydia.1N gonorrhoeae infection is easily transmissible, with a short incubation period. It is often asymptomatic in women, leading to delays in treatment, and an increase in the chances of complications such as infertility.1
Rapid diagnosis by direct microscopy for N gonorrhoeae and bacterial culture for N gonorrhoeae still remains the “gold standard” for diagnosis. However, N gonorrhoeae is a fastidious bacterium, that requires a CO2-rich environment and specialised agar growth medium to be grown in the laboratory. The sensitivity of detection by culture may therefore be affected by variations in the quality of the specimen taken, the isolation medium and in the conditions of transport and incubation.
Several commercial nucleic acid amplification technique (NAAT) assays are now being used widely for the diagnosis of genital chlamydial infections,2,3 for example, Becton Dickinson’s (BD) ProbeTec strand displacement assay (SDA; Becton Dickinson, Sparks, Maryland, USA), Gen Probe’s APTIMA COMBO 2 assay based on transcription-mediated amplification technology (Gen-Probe, San Diego, California, USA) and Roche’s Cobas Amplicor PCR assay (Roche Molecular Systems, Branchburg, New Jersey, USA). They are sensitive and specific, and have the added advantage that non-invasive specimens such as first void urine (FVU) and self-taken vulvovaginal swab can be used for diagnosis. Recently, these tests have also become available for the diagnosis of N gonorrhoeae infection. The advantage is that both Chlamydia trachomatis and N gonorrhoeae can be tested for on the same specimen using a common platform, and that the N gonorrhoeae NAAT assay, unlike culture for N gonorrhoeae, is not affected by the fastidiousness of the bacterium. However, further work is still required to determine the sensitivity and specificity of the N gonorrhoeae NAAT assays within different N gonorrhoeae prevalence populations before these assays can be implemented widely for routine screening of N gonorrhoeae infection. Also, the incidence of antibiotic-resistant N gonorrhoeae continues to increase,4 and therefore microscopy and culture, although labour intensive, are still important in providing rapid diagnosis and antibiotic susceptibility data.
BD ProbeTec SDA has been used in the Sheffield laboratory for some years for the diagnosis of genital C trachomatis infection. This study was designed to evaluate the N gonorrhoeae BD ProbeTec SDA on female endocervical swab and male FVU against culture for N gonorrhoeae on female endocervical and urethral swab, and male urethral swab for the diagnosis of N gonorrhoeae infection in genitourinary medicine (GUM) attendees. We also wished to determine an algorithm for implementation of N gonorrhoeae infection screening by SDA in this group of patients, taking account of the desirability of having a N gonorrhoeae isolate in people with N gonorrhoeae infection.
METHOD
During a period of 2 months in 2003, 1582 patients (731 men and 851 women) were tested for N gonorrhoeae infection using the BD ProbeTec ET assay (Becton Dickinson and Company) in addition to routine microscopy and culture. Microscopy and culture was done on both endocervical and urethral swabs for women, and urethral swabs for men.
The routine STI screening swabs were taken at the GUM clinic and inoculated directly onto Phillips agar plates. The plates were pre-incubated at 37°C in 5% CO2 before transportation to the laboratory where the incubation was continued. The plates were read at 24 and 48 h, and any suspect colonies were confirmed both biochemically (Neisseria PET; BioConnections, Leeds, UK) and antigenically (Phadebact; Launch Diagnostic, Longfield, UK). In addition, direct microscopy was performed on patients who either had symptoms or were considered to be at high risk for N gonorrhoeae infection.
The SDA for N gonorrhoeae was done, following the manufacturer’s instructions, on specimens submitted for detection of C trachomatis (ie, endocervical swab from women and FVUs from men). All initially reactive specimens were tested again by SDA, and only those which were positive twice were considered to be N gonorrhoeae SDA positive.
True N gonorrhoeae positive specimens were defined as those which were repeat reactive (ie, reproducibly positive in SDA and/or N gonorrhoeae culture positive and/or direct microscopy positive for N gonorrhoeae).
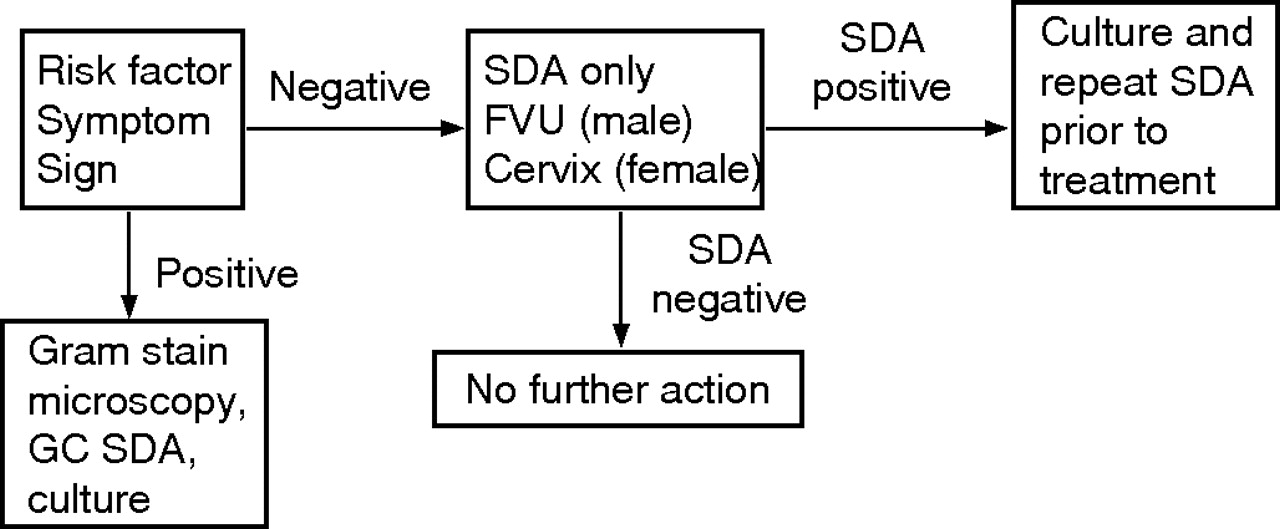
The N gonorrhoeae SDA and culture results were reviewed on a daily basis, and if the results were discrepant the SDA was repeated and the culture plates/organism were re-examined. The notes of the patients found to have N gonorrhoeae infection were reviewed retrospectively to assess risk factors for acquiring infection and these are listed (box 1). To implement the N gonorrhoeae screening by SDA in addition to N gonorrhoeae culture in patients with a listed risk factor, a protocol (fig 1) was then devised for the patients attending the GUM clinic and implemented in February 2005.

Protocol for use of the combined strand displacement asssay (SDA) test in clinical practice. FVU, first void urine; GC Neisseria gonorrhoeae.
Box 1 Risk factors associated with increased risk of Neisseria gonorrhoea infection
-
Known sexual contact of someone with N gonorrhoeae infection
-
Symptoms of possible N gonorrhoeae infection. (Uurethral discharge or dysuria in men; vaginal discharge, pelvic pain, dyspareunia or irregular vaginal bleeding in women).
-
Men who have sex with men
-
Previous N gonorrhoeae infection
-
Commercial sex workers
-
Sexual partners of commercial sex workers
A post-implementation audit was performed to validate the effectiveness of the protocol. A retrospective case note review of all patients diagnosed with N gonorrhoeae infection on any test (at all sites) from 1st February 2005 to 30th April 2005 was performed. Data were collected on sex, age, risk factors, symptoms, otherSTIs, consort data and tests performed along with the results.
RESULTS
N gonorrhoeae SDA and culture
Specimens from 64 patients were SDA positive on initial test, 11 (four FVUs from men and seven endocervical swabs from women) were initially SDA positive, but not confirmed as positive on repeat testing, all these results were obtained during a defined period of few days, during a cross-contamination incident in the laboratory. As the repeat SDA test was negative on these specimens, they did not meet the methodological criterion of a positive SDA result. In all, 53 patient specimens were repeat reactive in the SDA and considered as true SDA positive according to the methodological criteria. In all, 48 specimens were N gonorrhoeae culture positive and 46 specimens were positive by both culture and SDA results. Table 1 shows the comparative results of N gonorrhoeae SDA and culture.
Results of comparison of BD ProbeTec strand displacement assay with culture
Using the methodological criteria, 53 (3.4%) patients were diagnosed with N gonorrhoeae infection, 26 men and 27 women. The sensitivities of the SDA and culture were 98.1% (SD 3.8%) and 90.1% (SD 8.1%), respectively; however, on review of the culture results, the N gonorrhoeae culture sensitivity rose to 98.1% and was comparable to that of SDA (table 1). The specificity of the SDA was 99.2% for the initially reactive samples, rising to 100% for repeat reactive specimens in the assay, while the specificity for culture was 99.9%.
Risk factors in patients with N gonorrhoeae infection
All 26 (100%) men and 23 (85%) of women with N gonorrhoeae infection had at least one listed risk factor, and 15 (58%) men and 10 (37%) women with N gonorrhoeae infection had more than one listed risk factor (box 1) for acquisition. The most common listed risk factor was the presence of symptoms, 25 of the 26 (96%) positive men and 15 of the 27 (56%) women reported symptoms; 4 (15%) women with N gonorrhoeae infection were found to have had no listed risk factors for acquiring the infection.
Of the 27 women with N gonorrhoeae infection, 2 (7%) were found to be culture positive at the urethral site only, with a negative culture from the endocervical site. One of these women had a positive SDA on the endocervical swab. However, the endocervical swab from the other was N gonorrhoeae SDA negative. The second patient was asymptomatic and did not have any of the listed risk factors for N gonorrhoeae infection.
In a sample of 200 consecutive case notes (100 each from men and women) of GUM attendees, it was found that 38% of men and 60% of women had a specific listed risk factor or symptoms that would require specimens to be submitted for N gonorrhoeae culture at presentation, thus applying the devised protocol (fig 1) would halve the number of N gonorrhoeae cultures.
Post-implementation audit
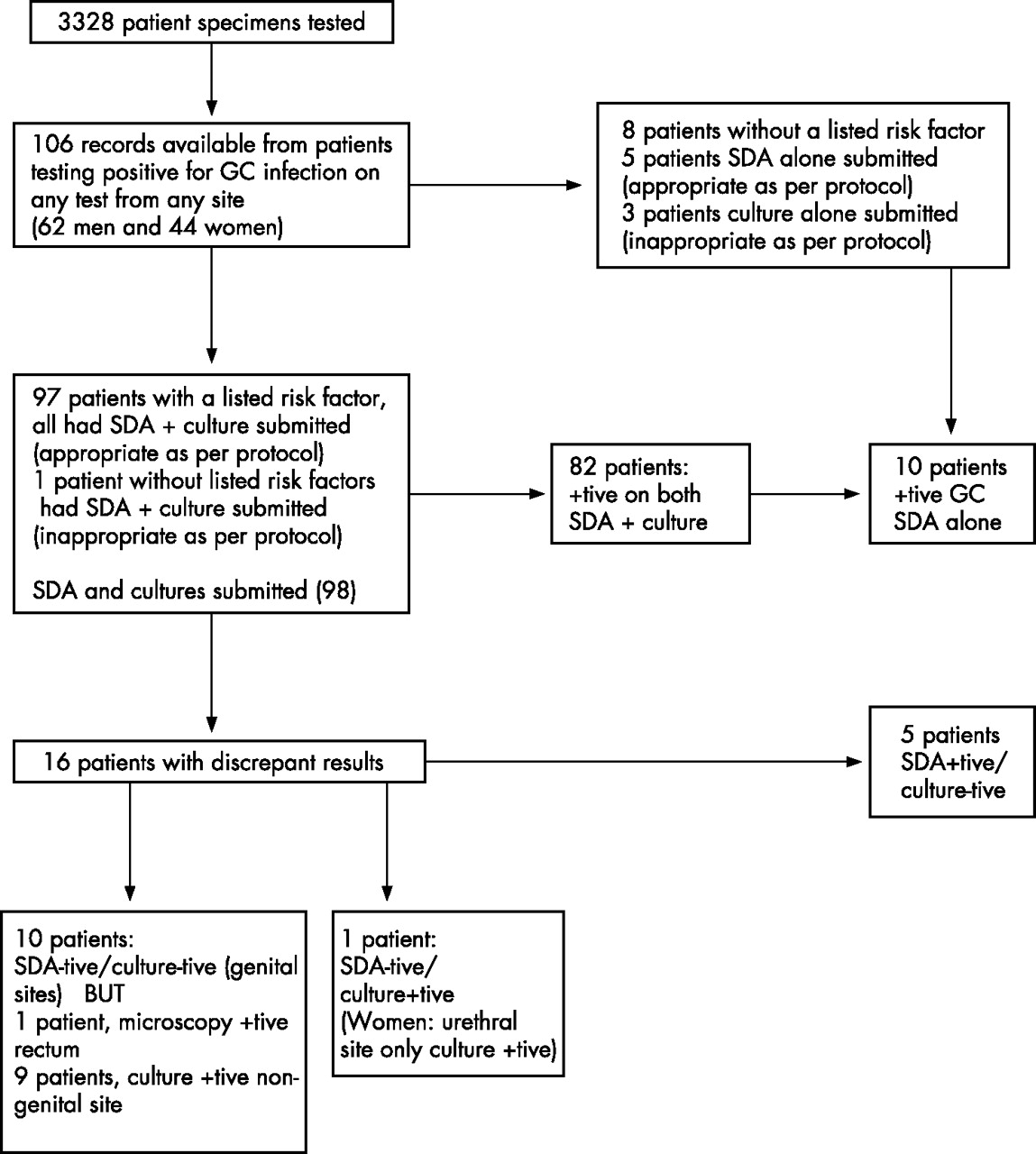
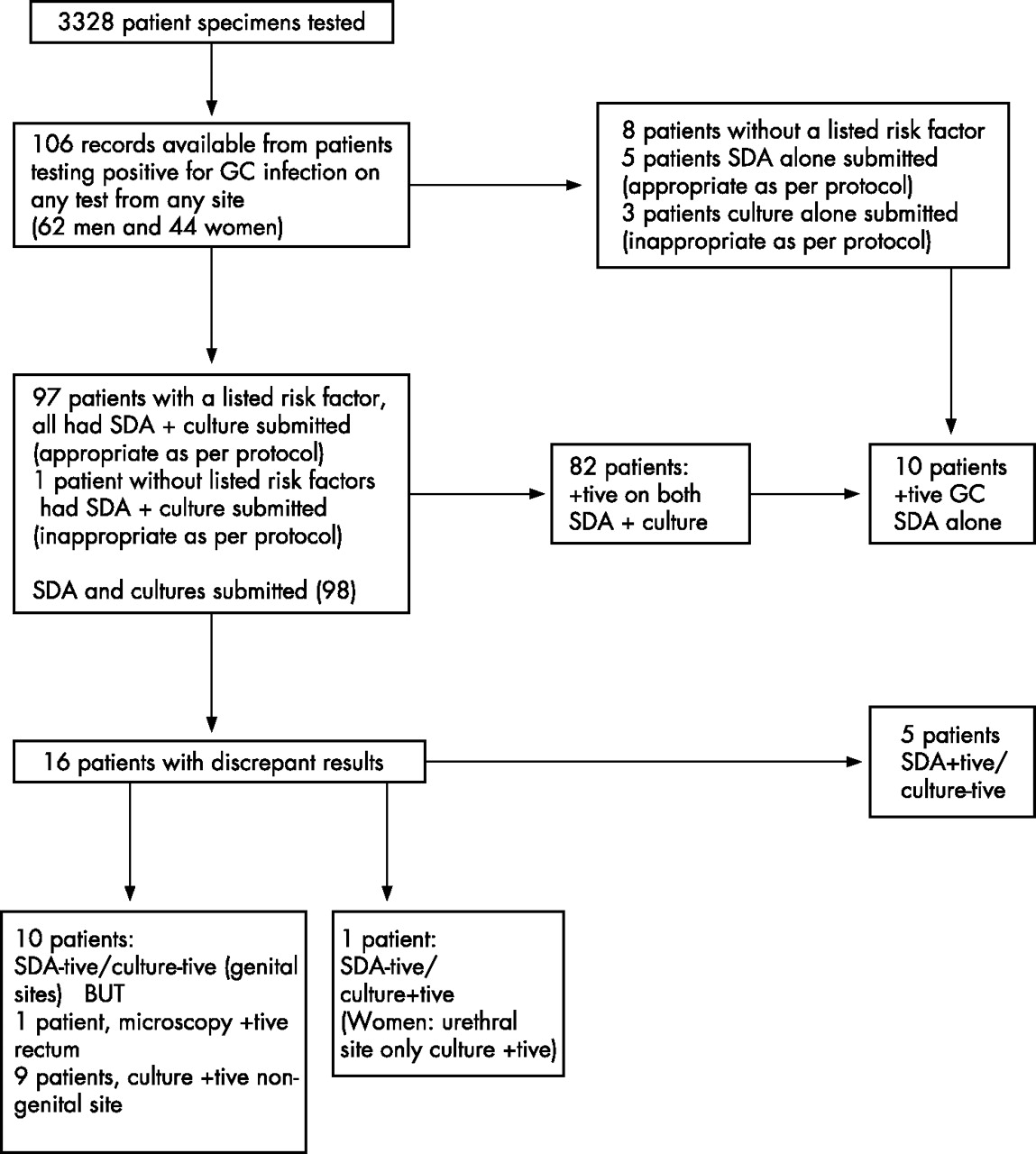
Between 1st February 2005 and 30th April 2005, 3328 patient samples were investigated for N gonorrhoeae infection according to the protocol.
In all, 107 (3.2%) were diagnosed with N gonorrhoeae infection, and 106 patients for whom case notes were available were evaluated (fig 2).
{kind=link}
{kind=link}
Flow diagram representing the results of the post-implementation audit of the strand-displacement assay (SDA) screening protocol. GC, Neisseria gonorrhoeae, +tive, positive; −tive, negative.
In all, 97 patients, 59 of 62 (95%) men and 38 of 44 (86%) women, had a listed risk factor (box 1) for acquiring N gonorrhoeae infection. Correct protocol for sampling had been followed in all of these, and they all had N gonorrhoeae culture and SDA swabs taken at presentation.
Additionally, a patient without listed risk factors had culture and SDA specimen submitted.
Therefore, 98 patients had both N gonorrhoeae culture and SDA submitted, with 82 of these testing positive with both tests. Of the remaining 16 patients, 10 were diagnosed by culture alone, but had N gonorrhoeae isolated from a site (nine from rectal or pharyngeal and one from female urethra) from which N gonorrhoeae culture alone was submitted. Five patients were SDA positive alone, with negative culture. One patient was negative on both the SDA and culture, testing positive on rectal microscopy alone after being identified as a gonorrhoea contact (fig 2).
The other 8 patients with N gonorrhoeae infection did not have a listed risk factor, 5 (5% of the positive or 0.15% of the tested population) of them required recall for N gonorrhoeae culture prior to initiating treatment because according to the protocol (fig 1), they only had a SDA swab taken at presentation. However, the protocol was then followed poorly in these individuals, as only one was re-tested with SDA and culture prior to treatment. The other three were diagnosed by a positive N gonorrhoeae culture, which was submitted despite the protocol requiring the submission of SDA swab for N gonorrhoeae screening from patients without listed risk factors.
In total, 10 individuals tested positive with the SDA alone, either because cultures were negative or not done. When a full assessment of these individuals was done taking into account the results of microscopy, risk factors for gonorrhoea, follow-up tests, consort data and other microbiological information, 7 of the 10 were found to have evidence to back up a positive SDA for N gonorrhoeae infection (table 2). Three patients had no identifiable listed risk factor or positive culture or microscopy at the time of positive SDA test. Only one of these patients had a follow-up culture test, which was negative.
Listed risk factors and results of follow-up Neisseria gonorrhoeae cultures on patients diagnosed with N gonorrhoeae infection by positive N gonorrhoeae test alone
DISCUSSION
Our study, like others,2 shows that SDA for N gonorrhoeae is both sensitive and specific for the diagnosis of N gonorrhoeae infection in a high-risk population of GUM attendees, and provides a rapid and objective diagnosis with the advantage of use of a non-invasive and single specimen for screening for C trachomatis and N gonorrhoeae. During our evaluation study of the SDA, we found that 83% of the positive SDA samples gave a reproducible positive result; however, all the non-repeatable positive results were obtained during a period when the laboratory experienced problems with cross-contamination, therefore none of these results was reported prior to repeat testing for confirmation. Once the cross-contamination was controlled, we did not experience any further non-repeatable positive results in the SDA.
Further work shows that 94% of specimens which are repeat reactive in the N gonorrhoeae SDA with a method other than acceleration value of ⩾10 000 were culture positive, the remaining either had positive microscopy for N gonorrhoeae, were contacts of N gonorrhoeae -confirmed patients or had cultures submitted after antibiotic treatment.5 In addition, our post-implementation audit of the protocol also showed that 70% (7 of 10) patients who had N gonorrhoeae infection diagnosed by repeat reactive SDA test alone had features that were consistent with the diagnosis (table 1). N gonorrhoeae infection could not be confirmed in three patients due to lack of follow-up in two and identifiable risk factors in the third.
These results show the importance of repeat testing of all specimens initially reactive by a NAAT and the value of environmental sampling to identify laboratory cross-contamination. Failure to do so would lead to the incorrect classification and unnecessary treatment of patients because of false positive SDA test result.
Culture for N gonorrhoeae, although invaluable in its ability to provide an isolate for sensitivity testing, requires stringent culture conditions and has problems with subjectivity of interpretation. We came across both false negative and false positive N gonorrhoeae culture results in the evaluation study. We suspect that our laboratory is not unique in this respect, as these results would normally go unnoticed without a parallel test like the SDA test. Notably, review of culture results from five of the seven patients with discrepant culture and SDA result confirmed the SDA result to be the true result. In a laboratory with a heavy workload and N gonorrhoeae prevalence of 3.4%, the majority of culture plates to be read are negative. Using SDA as first-line screen for N gonorrhoeae infection to screen out the negative samples, allows the laboratory to discard the negative plates without having to incubate them for a full 48 h, also, as the positive specimens are identified early on by the SDA test, the laboratory staff are able to concentrate on culture plates from the positive samples, thereby saving time and reducing the risk of errors and subjectivity in identifying positive culture isolates. Our laboratory was already doing the chlamydia screening by BD ProbeTec SDA, the consumable cost of the combined chlamydia/ N gonorrhoeae kit was marginally more; however, this was offset by the saving in staff time because of the reduction in the number of N gonorrhoeae cultures submitted. The laboratory was therefore able to introduce the protocol on a cost neutral basis.
The problem of a negative SDA on endocervical swabs remains a concern in women with N gonorrhoeae at the urethral site only. In a study from 1978,6 607 women presenting to a GUM clinic in London were found to have N gonorrhoeae infection. Sampling of these women was similar to our current practice, with microscopy and culture being taken from the urethra and cervix of all women attending for screening. Rectal microscopy and culture along with pharyngeal culture were only taken in women known to be contacts of N gonorrhoeae infection. Of these 607 women, about 30% were found to be positive at a single site only and in 6% of cases, this single site was the urethra. This was a large study and therefore probably more representative of this aspect of sampling than our small study. In our study, 2 of 27 (7%) women were culture positive at the urethral site and culture negative at the endocervical site, with SDA detecting one of these at the endocervix. Therefore, 1 (4%) of these women with N gonorrhoeae infection would have been missed if SDA were done on the endocervical site alone. This woman was asymptomatic and had no known risk factors. The feasibility and economics of testing more possible sites of infection with NAATs should be investigated.
There is an obvious need to have culture isolates from infected patients for testing antibiotic sensitivity, both to provide epidemiological data on resistance patterns and also for the management of individual patients. The ability to identify the majority of those with likely N gonorrhoeae infection prior to initial testing is essential, so as to minimise the number of patients requiring recall for a further N gonorrhoeae culture test before treatment. In our study, all men with N gonorrhoeae infection had an identifiable listed risk factors, so the assessment of risk factor that we have described appears to be a good way of identifying men at high risk of N gonorrhoeae infection. Only 4 (15%) women without an identifiable listed risk factor were found to be infected. We therefore drew up a protocol that required all FVUs from men and endocervical swabs from women to be screened for C trachomatis and N gonorrhoeae by SDA. In addition, samples from patients with any of the listed risk factors (box 1) for N gonorrhoeae infection were also examined by culture. For those patients who were SDA positive but had not already been cultured (because of lack of known listed risk factors), we took a culture swab at the recall visit before starting treatment. A pre-implementation audit suggested that this would result in reducing the number of culture screens by half, allowing the laboratory to concentrate on cultures from those patients who are likely to be positive.
Key messages
-
Molecular diagnosis of Neisseria gonorrhoeae is feasible in a routine diagnostic setting for genitourinary medicine attendees. Provided that positive results are confirmed by repeated testing of the sample, the Becton Dickinson strand displacement assay (BD ProbeTec SDA) is both sensitive and specific
-
Molecular diagnosis of N gonorrhoeae provides rapid results and allows the use of non-invasive samples (first void urine in men), with benefits for workflow in both the laboratory and the clinic
-
A differential protocol which includes a sample for N gonorrhoeae culture from those with a listed risk factor for N gonorrhoeae infection will allow a N gonorrhoeae isolate to be available for antibiotic sensitivity testing
A post-implementation audit confirmed that the protocol can be easily followed in a busy GUM clinic and had actually achieved a reduction of 59% in culture submission. We found that the protocol was followed well in patients with a listed risk factor, but some patients without a listed risk factor also had culture specimens (contrary to the protocol) submitted.
We also found that there was no difference before and after implementation of N gonorrhoeae SDA test, in the prevalence of N gonorrhoeae infection (3.4% and 3.2%) or the number of patients with N gonorrhoeae infection who have a listed risk factor for acquiring infection (92.5% and 92%) in the population studied. Our post-implementation audit confirmed the high concordance in results between FVU SDA and urethral swab cultures in males, and SDA and culture both on endocervical swabs in females. Whenever the diagnosis of N gonorrhoeae infection was made on the basis of culture alone, it was from a site other than urethral (male) and endocervix (female), this emphasises the relevance of continuing to sample other anatomical sites as indicated by sexual practice. Only 1 of 44 (2%) female patients had infection at the urethral site alone, and this was consistent with our earlier finding. Interestingly, our post-implementation audit showed that only 5% of the positive patients or 0.15% of the tested population required a recall for N gonorrhoeae culture prior to initiating treatment, compared with the projected figures of 7% and 0.25%, respectively, on the basis of the initial study.
The implementation of this test into our routine clinical practice from February 2005 has contributed to changes in many areas of our clinical practice. Less time spent on microscopy and not having to take urethral swabs from the majority of male attendees has allowed us to significantly increase our clinical throughput, and we have been able to use the SDA test as part of a fast-track clinic for screening asymptomatic patients. A recent audit of clinical practice has shown that between May 2005 and November 2005, 48 h access has improved from 24% to 40%. We also found that turnaround time for negative results improved as these were reported the next day rather than after 48 h of culture. Another benefit was the increase in acceptability of the test by male patients (especially in the asymptomatic men) because of testing via non-invasive FVU.
Our experience shows that NAAT screening can be successfully introduced in a routine GUM setting for screening N gonorrhoeae infection without the loss of epidemiological data on sensitivity of the organism. A NAAT screening protocol for N gonorrhoeae infection, as implemented by us, has many advantages like improved turnaround time for negative results, increased patient throughput in the clinic because invasive urethral sampling in men can be avoided and acceptability of screening for N gonorrhoeae infection, especially in men because of the non-invasive sampling. Furthermore, as the NAAT screening can be automated, it allows the laboratory to concentrate on culture samples from patients likely to yield a positive result.
Acknowledgments
We thank the statistics department at the Sheffield Teaching Hospital Trust for statistical advice and Dr Christine Bowman, Consultant GUM physician at Sheffield and Rotherham, for providing the audit data on 48 h access.
REFERENCES
COMMENTARY
Developments in diagnostic techniques that demonstrate significant advantages on robust evaluation should be welcomed into clinical practice. Nucleic acid amplification tests (NAATs) are already widely used in North America and some European countries for the detection of Neisseria gonorrhoeae infection, often as a combined chlamydia/gonococcal (GC) test at little or no extra cost. There are important drivers why these tests should be more widely used—they are highly sensitive, they facilitate modernisation of service delivery in genitourinary medicine (GUM) clinics, they enable screening in community settings with specimens collected by patients and they are amenable to automated processing. Culture still remains necessary for surveillance of antimicrobial resistance, confirmatory testing and testing at non-genital sites (rectum and pharynx).
In this issue, Ryan et al1 validate the BD Probe Tec assay and describe an algorithm using this assay as the standard test for detection of N gonorrhoeae at genital sites in a GUM clinic setting. Microscopy is still used as a rapid test, but selectively for patients with symptoms or a specific risk factor for gonorrhoea. Culture is maintained, but again used selectivity for patients with symptoms, those at higher risk of gonorrhoea (men who have sex with men, past infection with gonorrhoea or contacts of gonorrhoea) and for testing at non-genital sites. The reported outcome of this approach is increased sensitivity of gonorrhoea detection, confirmation by culture for most infections and reduced laboratory processing of negative culture plates. The study also offers further reassurance on the specificity of GC NAATs when supported by supplementary testing, as has recently been reported in a population with low prevalence of gonorrhoea.2
Should the Sheffield algorithm be widely adopted by GUM clinics? Might alternative testing protocols be more appropriate? Could dual testing by NAAT and culture be reduced further? Screening men for urethral infection by a combined GC/chlamydia NAAT on urine with an additional urethral culture test taken from those who are sexual contacts of gonorrhoea or who have symptoms or signs of urethral discharge would seem fairly straightforward. Asymptomatic and untreated men testing positive in the NAAT would be reassessed by culture and then receive antimicrobial treatment. In women, genital tract GC infection is frequently asymptomatic. Infection may be confined to the urethra. Vaginal discharge is a common symptom, with poor sensitivity and specificity for this infection. Do cultures really need to be taken for all symptomatic women? Further debate is needed and more experience needs to be gained on the relative effectiveness of taking cultures using a “best-guess” approach as against greater reliance on recall and reassessment. History shows that the UK was slow to implement molecular tests for the detection of genital-tract chlamydial infection. With appropriate strategies and quality assurance, the time is surely right to move forward with GC NAATs.3
Footnotes
-
Published Online First 3 January 2007
-
Competing interests: None declared.
-
All authors contributed to the conceptualisation and development of the project, in addition: CR contributed in collection and analysis of clinical data, synthesis of relevant literature and writing and critical review of manuscript; GK in supervision of SDA technical work, analysis of laboratory data, synthesis of relevant literature and writing and critical review of manuscript; SMI in performance of SDA technical work and analysis of laboratory data; SD and PZ in analysis of laboratory data, critical review of manuscript and supervision of N gonorrhoeae cultures; and GK in critical review of manuscript and supervision of clinical data collection.