Article Text

Abstract
Objectives: To assess the feasibility and acceptability of opportunistic Chlamydia trachomatis (CT) screening of asymptomatic men attending three different secondary healthcare settings and to investigate CT positivity in these settings.
Methods: Men attending fracture, fertility and family planning (FP) clinics were invited to be screened by first-void urine and complete a questionnaire which collected demographic, sexual and behavioural characteristics, and their opinion about the screening process.
Results: 1290 men were approached, with 80% participating. The number of men approached, number providing a satisfactory urine specimen and CT positivity rate (95% CI) were, respectively, n = 401, n = 206, 14.6% (10.4 to 20.1) for the FP clinic, n = 505, n = 328, 1.2% (0.5 to 3.2) for the fracture clinic and n = 384, n = 319, 0.3% (0.1 to 1.8) for the fertility clinic. The highest rates of CT infection were found in men attending the FP clinics, aged between 20–24 years. Most of the men from all three clinics felt that the setting (87.9%) and specimen (97.7%) were acceptable.
Conclusion: Opportunistic chlamydial screening of asymptomatic men in three secondary healthcare settings found high positivity rates, but low uptake rates in a FP setting compared with fertility and fracture clinics. Innovative and targeted intervention strategies are required to engage this high-risk group of men in screening.
- CT, Chlamydia trachomatis
- FP, family planning
Statistics from Altmetric.com
Chlamydia trachomatis (CT) infection is the most common sexually transmitted infection in the UK, with profound consequences on reproductive health. In the UK, the incidence of CT is rising (http://www.hpa.org.uk/hpa/publications/hiv_sti_2005/chlamydia.htm). Although increased screening opportunities and sensitivity of testing have played a part, the influence of a male reservoir of infection has recently been considered.1 Despite the evidence that the number of men attending general practitioners is higher than women, the overall number of men screened for CT is low.2 In the case of female screening, infection eradication is usually hampered by poor compliance in the treatment and follow-up of male partners.3 Thus, the combination of suboptimum rescreening strategies in women and a relatively unscreened and untreated population of men promote reinfection and undermine programmes aiming to reduce chlamydia infection. Universal screening of men has not been shown to be cost-effective per event prevented,4 but a recent study highlighted the potential of opportunistic testing among women.5 A recent pilot study comparing postal and opportunistic screening in women has confirmed the feasibility of an opportunistic approach, but was unable to provide any firm conclusions owing to its pilot nature and a high opt-out rate before randomisation.6
If men are to be included in the screening process, it is important that local prevalence rates of CT in asymptomatic men are determined first. Despite the paucity of studies on men, available evidence suggests that the prevalence of CT among UK men ranges from 1% to 5% in population-based studies7–9 and from 1% to 16%3,10,11 in clinic-based studies in settings such as the armed forces, general practice, family planning (FP), orthopaedic and genitourinary medicine. The wide range reported indicates the mixed settings, different recruitment methods and varying uptake rates. Moreover, although these figures represent the situation in England, few data exist for asymptomatic CT infection rate among men in Scotland. For example, there is variation in CT positivity by setting and gender in Portsmouth (an area chosen by the Department of Health, London, UK, for the screening pilot) compared with the Highlands,12 although this would have been affected by different screening approaches in England and Scotland.
The aims of this study were to investigate the positivity of CT infection in asymptomatic men attending three different secondary healthcare settings—a fracture clinic, a fertility clinic and a FP clinic, and to ascertain the acceptability and feasibility of screening in each setting. This approach paralleled that of the National Chlamydia Screening Programme where screening is offered in both primary and secondary healthcare settings.3
METHODS
As part of a prospective cross-sectional study, we approached men attending three outpatient clinics over a 2-year period. Recruitment was undertaken on a part-time basis, but on recruitment days, we invited consecutive male patients to participate. Men aged >15 years were identified from the fertility and fracture clinic lists and given an information leaflet by the researcher. All men attending FP clinic were approached and given an information sheet if they confirmed that they were aged >15 years. Those consenting to take part completed a questionnaire. Men who were not sexually active were excluded. Presence of symptoms was systematically explored by three questions pertaining to urinary symptoms, penile discharge and scrotal pain. Men who had symptoms were excluded from analysis. The questionnaire collected brief demographic, sexual and behavioural data. An acceptability survey was also carried out within the same questionnaire exploring the appropriateness of the clinical setting in which screening was carried out and the acceptability of the sample. Comments on CT screening were requested. Men were given the opportunity of privacy to complete the questionnaire, and informed consent was obtained. Non-anonymised contact details were recorded and a preferred contact method was requested. Participants were asked to provide a first-void urine sample at the clinic. This was tested using a strand displacement amplification assay (Becton Dickinson Diagnostic System, Oxford, UK) as per manufacturer’s instructions. In keeping with existing laboratory protocols, positive specimens were tested again, and only those confirmed as positive on a second test were reported as truly positive. Positive results that were not confirmed on repeat testing were reported as “equivocal” and a further specimen was requested. Patients who tested positive were referred to the genitourinary medicine clinic, FP clinic or their general practitioner for treatment and partner notification.
Assuming CT positivity in asymptomatic men to be 5%, we estimated that a sample size of 328 men in each setting would allow us to estimate the proportion of men testing positive within 3% (95% CI 2% to 8%). Data were recorded on a database and analysed using SPSS V.13.0. The Grampian Research Ethics Committee approved the study.
RESULTS
Overall
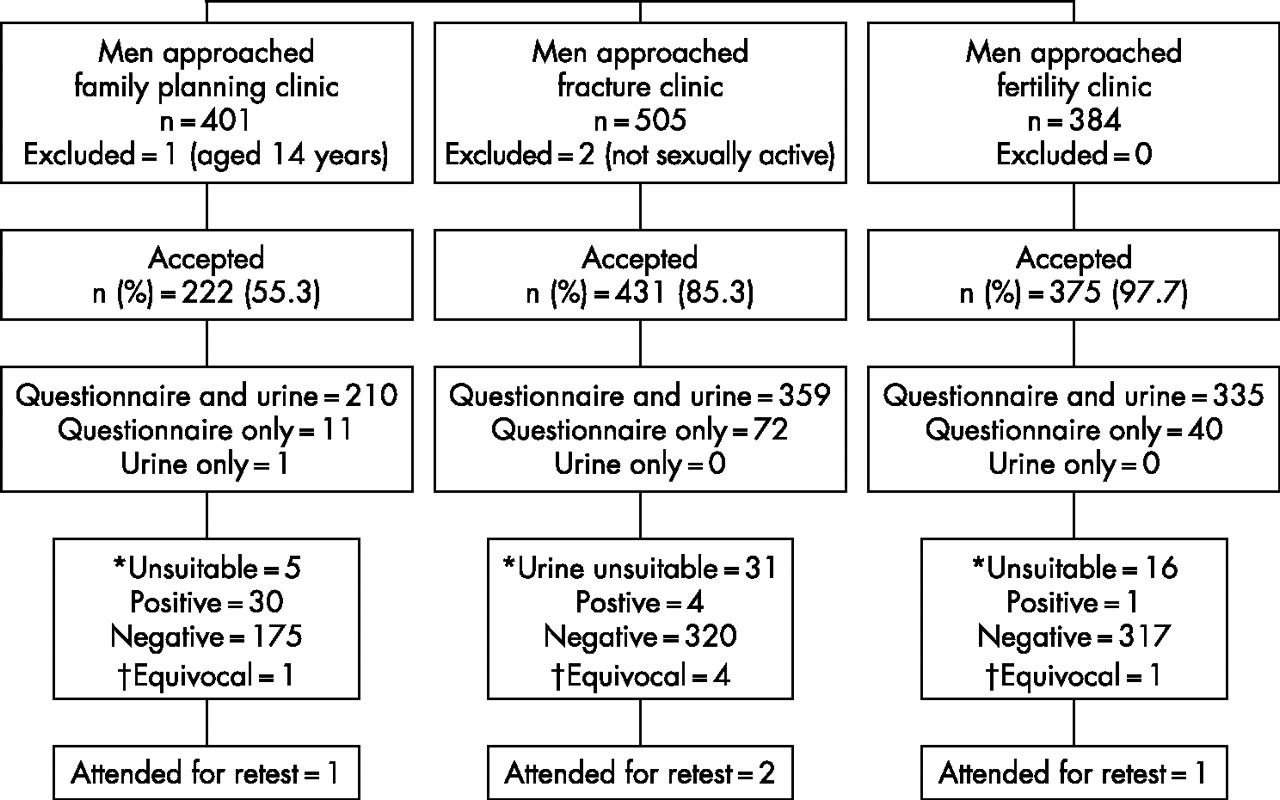
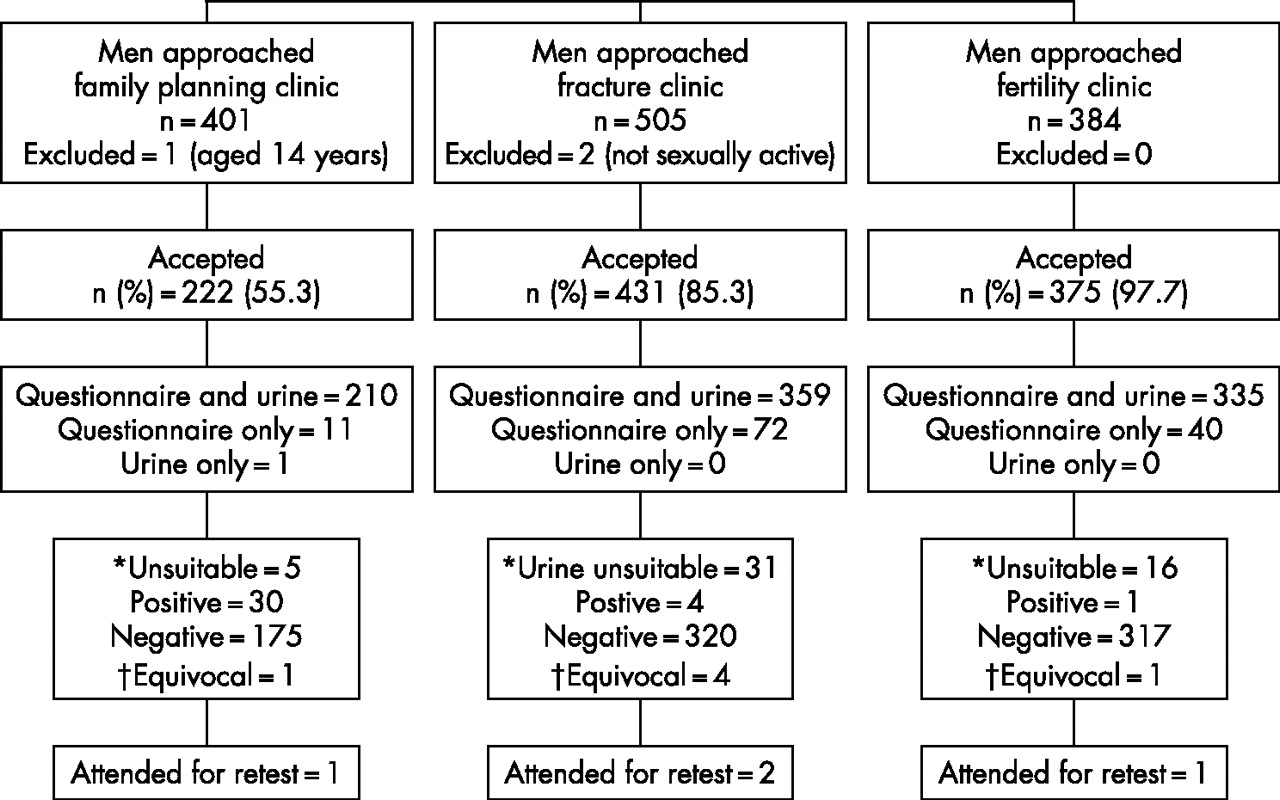
Figure 1 shows the number of participants in each setting. Figures for the number of men approached are shown, but we were unable to ascertain the total number of men eligible for the offer of the screening test in each setting. None of the participants were excluded due to symptoms, but two men attending the fracture clinic and one attending the FP clinic were excluded for never having been sexually active and for being aged <15 years, respectively. Table 1 gives the setting-specific positivity figures and other demographic characteristics for CT positivity. The highest infection rates were found in those attending FP clinics, aged 20–24 years. In all, 58 (7%) specimens needed to be repeated due to an unsuitable specimen or equivocal results (fig 1), and awareness about CT was higher in the sexual health settings (table 1). Most participants (94%) requested conveying of positive status by mobile phone.
Comparison of participants’ characteristics and prevalence in the three clinical settings
{kind=link}
Flow of participants. *Unsuitable sample, sample with inhibitory substances, leaking on arrival at laboratory, insufficient quantity. †Equivocal sample, further urine sample required for retest.
Table 2 summarises the acceptability survey in all three settings. Uptake rates varied considerably between the three settings, with higher rates (87.2%) being reported from fertility clinics, than the FP clinic (52.6%) and fracture clinics (71.1%). Most of participants felt that the clinic they attended was an acceptable setting (87.9%) and that urine was an acceptable specimen (97.7%) for testing. Comments such as the following highlighted men’s understanding of the consequences of Chlamydia infection:
Men’s uptake of opportunistic screening and acceptability of setting and specimen type in the three settings
... these issues should be highlighted more often ... (study number 55, fracture clinic)
... it should be done to stop the spread ... (study number 760, fertility clinic)
Five men made comments that the urine specimen was easy to produce and preferable to a urethral swab,
... it was by far the most convenient option I was aware of ... (study number 900, family planning clinic)
… it was an easy way to find out if you have an infection … (study number 989, family planning clinic)
but one commented that it was not easy to produce the sample on demand.
… could not produce a urine sample … (study number 431, fracture clinic).
Family planning clinic
The median (interquartile range, IQR) age of participants was 21 (19–24) years. This setting had the highest positivity rate, 14.6% (95% CI 10.4 to 20.1), with highest infection rates found in men aged 20–24 years, 25.6% (95% CI 17.4 to 36.0; table 1). This setting had the lowest uptake (52.6%; table 2) and the highest number of men with a history of infection with CT (5.0%; table 1).
Fertility clinic
Men in this clinic were older in comparison to other settings, with a median (IQR) age of 35 (31–39) years. This setting had the highest uptake (87.2%) and lowest positivity rate (0.3%) (95% CI 0.1 to 1.8).
Fracture clinic
This group had the largest proportion (17%) who failed to provide a urine specimen. The median (IQR) age of participants was 33 (23–42) years. Low positivity rates were found 1.2% (95% CI 0.5 to 3.2).
DISCUSSION
Uptake and acceptability of screening setting and specimen type were high in the fertility and fracture clinic settings. In contrast, only half of those who were approached at the FP clinic agreed to screening, yet infection rates were highest among these men.
To our knowledge, this is the first study that assesses the acceptability of opportunistic CT screening of men in secondary healthcare settings. The strengths of this study include the large numbers screened, the clinical settings chosen and the asymptomatic population. The study’s limitations include the possibility of selection bias, as we were unable to collect the number of men eligible for the study in each setting and the poor uptake rates that were reported in the FP group. As a result, positivity rates and acceptability reported in each setting may not be universally applicable. Our inability to re-test a proportion of samples from men in whom initial urine samples were reported as unsuitable/equivocal reduced the overall number of men screened. The wide CIs around the proportion of men testing positive indicated the small number of overall positives in an asymptomatic unselected population. Finally, data from the fertility clinic lacked information on condom usage, and a partner change in the preceding 6 months, as these questions were deemed ethically unsuitable.
In terms of comparative prevalence rates, a systematic review of male prevalence studies has been published.13 Our results from the FP clinic confirm the high infection rates (13%) reported from the National Chlamydia Screening Programme.3 There, half of those who were aged <25 years and were screened using strand displacement assay of first-void urine also came from FP clinics. We were unable to compare uptake rates as these were not available. Similar high infection rates (10%) were also reported in a Scottish study involving male military recruits of all ages, where participation was universal and most (90%) were asymptomatic.10 No other study in a non-genitourinary medicine setting has been able to replicate these results, suggesting that the military population may be unique in terms of uptake of screening and CT positivity. In contrast, other studies screening young men using urine assayed using ligase chain reaction have reported low positivity rates of 1% and 2% among 758 male students aged between 18–21 years in Sheffield9 and 501 men aged between 18–35 years in London, respectively.8 These studies, however, had low uptake rates (29–50%), used a mixture of postal and clinic-based screening approaches, and did not exclude men who were not sexually active. Regarding the fracture clinic population, a study undertaken in an orthopaedic outpatient setting reported higher (6%) rates of CT positivity, but most (82%) participants were aged <29 years.11 The low infection rates reported in this group are similar to that found in the National Survey of Sexual Attitudes and Lifestyles (2% among men aged 18–44 years) and ClaSS (chlamydia screening studies) project (3% among men aged 16–39 years), both community-based postal surveys.14 Our uptake rate was higher than the 35% reported by ClaSS possibly reflecting the face-to-face invitation to screening, although such influence is yet unproven. The uptake rate (70%) reported in an orthopaedic outpatient setting11 was similar to the 71% in males of fracture clinic who produced a urine sample. These uptake rates probably reflect the opportunistic approach against a background of other pressing medical issues.11 The very low positivity reported from the fertility clinic suggests that these men represent a low-risk population, influenced by older age and stable sexual relationships. To our knowledge, there are no comparative, published UK studies from this clinical setting.
Key message
-
Men are likely to take up opportunistic Chlamydia screening by first-void urine.
-
Positivity rates and uptake vary depending on clinical setting.
-
Young men attending family planning (FP) clinic are at highest risk of infection.
-
Interventional strategies to improve uptake in FP clinics are urgently needed.
In our study, the disparity between the three clinical settings in terms of uptake and test positivity could be due to a number of reasons. Age is inversely associated with male positivity in national genitourinary medicine figures (http://www.hpa.org.uk/infections/topics_az/hiv_and_sti/epidemiology/2005datatables/Sel16 ected_sti_UK_tables_1996_2005.pdf pg 11) with highest rates found in men aged 20–24 years. About 40% of participating men in the FP clinic belonged to this age group, compared with 11% and 1.5% in the fracture and fertility clinics, respectively. Furthermore, those attending the fracture and fertility clinics were patients attending a hospital clinic for investigation or treatment. As personal health status would be high on their agenda that day, this might make them more likely to agree to see another healthcare professional and undergo investigations. Time constraints would also be less of a factor. In contrast, those attending the FP clinic did not anticipate a health contact as they were either there as accompanying partners or had dropped in to pick up condoms. As a result, this group of men would have been less prepared to wait, provide a sample or complete a questionnaire.
Ecological time trend studies from Europe15 and America16,17 show a decline in pelvic inflammatory disease associated with screening activities. However, these population-based ecological trends may not constitute evidence of the effectiveness of screening interventions at an individual level.18 A recent rise in CT infection in Sweden has suggested that suboptimum female screening coverage and partner notification of positive cases are promoting reinfection. In the UK, although women have been targeted with greater emphasis as they are thought to be easier to reach and as they develop long-term morbidity, there is now a recognition that men have riskier patterns of sexual behaviour,7 and attend primary care more often than previously thought.2 It is therefore disappointing that both population-based postal and opportunistic screening approaches to date, do not target men effectively.14
If men are to move higher up on the Chlamydia-prevention agenda, screening must branch out to clinical areas that are attended by men. This study confirms the feasibility of CT screening in these three secondary healthcare settings. Further prevalence studies are needed to advise on the specific clinical settings and type of men whom screening should target, and uptake must be improved in settings where prevalence is high. Assessing reasons for non-uptake would inform targeted interventional strategies, although the hidden costs of screening, psychological sequelae, social stigma associated with testing and difficulties in partner notification require further attention.19 Current attempts to engage men and provide a more holistic approach to sexual and reproductive health can only improve inclusion in the screening process. Targeting men with equal emphasis may, in the long term, help improve male sexual health, avoid sexual stereotypism, inculcate responsibility for sexual health and ultimately control the rise in sexually acquired infections.
CONCLUSION
Opportunistic chlamydial screening of asymptomatic men in three secondary healthcare settings found high positivity rates, but low uptake rates in a FP setting compared with fertility and fracture clinics. Innovative and targeted-intervention strategies are required to engage this high-risk group of men in screening.
REFERENCES
Footnotes
-
Published Online First 21 February 2007
-
Funding: Funded by University of Aberdeen.
-
Competing interests: None.
-
SS was involved in project design, and was responsible for recruitment, data analysis and writing the first draft; SL was involved in project design and interpretation of results, responsible for editing the paper; SMcG was involved in recruitment and analysis in family planning clinics; AT initiated the project and edited the final draft; HM was involved in project design, interpretation of results and was a liaison consultant in microbiology; AS was involved in patient recruitment and was a liaison consultant in the fracture clinic; MH peer-reviewed the protocol and was involved in interpretation of results; and SB was involved in project design, supervision of the project and editing the paper.
Linked Articles
- Editorial