Article Text

Abstract
Background: In England, screening for genital chlamydial infection has begun; however, screening frequency for women is not yet determined.
Aim: To measure chlamydia incidence and reinfection rates among young women to suggest screening intervals.
Methods: An 18-month prospective cohort study of women aged 16–24 years recruited from general practices, family planning clinics and genitourinary medicine (GUM) clinics: baseline-negative women followed for incidence and baseline-positive women for reinfection; urine tested every 6 months via nucleic acid amplification; and behavioural data collected. Extra test and questionnaire completed 3 months after initial positive test. Factors associated with infection and reinfection investigated using Cox regression stratified by healthcare setting of recruitment.
Results: Chlamydia incidence was mean (95% CI) 4.9 (2.7 to 8.8) per 100 person-years (py) among women recruited from general practices, 6.4 (4.2 to 9.8) from family planning clinics and 10.6 (7.4 to 15.2) from GUM clinics. Incidence was associated with young age, history of chlamydial infection and acquisition of new sexual partners. If recently acquiring new partners, condom use at last sexual intercourse was independently associated with lower incidence. Chlamydia reinfection was mean (95% CI) 29.9 (19.7 to 45.4) per 100/person-year from general practices, 22.3 (15.6 to 31.8) from family planning clinics and 21.1 (14.3 to 30.9) from GUM clinics. Factors independently associated with higher reinfection rates were acquisition of new partners and failure to treat all partners.
Conclusions: Sexual behaviours determined incidence and reinfection, regardless of healthcare setting. Our results suggest annual screening of women aged 16–24 years who are chlamydia negative, or sooner if partner change occurs. Rescreening chlamydia-positive women within 6 months of baseline infection may be sensible, especially if partner change occurs or all partners are not treated.
- GUM, genitourinary medicine
- NCSP, National Chlamydia Screening Programme
Statistics from Altmetric.com
The implementation of the National Chlamydia Screening Programme (NCSP) is currently underway, targeting young men and women aged <25 years for screening outside genitourinary medicine (GUM) settings,1,2 operating within guidelines for target populations, screening venues, type of specimen and laboratory test, and management and follow-up of screened people3; however, there are no guidelines for screening intervals.
In the US, the Centers for Disease Control and Prevention has recommended 6-monthly rescreening of chlamydia-positive women, annual screening for others who match selective criteria, and cessation of screening for women with three consecutive annual negative tests and no change in sexual partnership.4 Published studies have reported incidence rates ranging from 3 to 34 and reinfection rates from 4 to 51 per 100 person-year,5,6,7,8,9,10,11,12,13,14,15,16 but many were limited by either design8,9,12–15 or measurement of incidence or reinfection.6,11–13,16 Some studies did not include patient-treatment information, making it difficult to assess patient-treatment non-compliance or patient-treatment failure as explanations for reinfection.11,12,14,15 Lastly, previous studies were unable to reliably investigate associations with time-dependent risk factors such as the acquisition of new sexual partners10–16 or the unsuccessful completion of partner treatment.5,6,7,8,9,10,11,12,13,14,15,16 The aim of our study was to estimate chlamydia incidence and reinfection rates in women recruited from general practice, family planning and GUM clinics, overcoming these limitations, and to use these estimates to suggest screening intervals for women participating in the NCSP in England.i
METHODS
Study population
We designed a prospective cohort study of women aged 16–24 years. A range of infection rates at 1, 5, 10, 15 and 20% with corresponding 95% confidence intervals were calculated based on sample sizes of 100, 200, 500 and 1000 women using the GLIM software developed by the Health Protection Agency Statistics Unit. Targets of 1200 negative women (400 in each setting) and 700 positive women (240 each from general practices and family planning clinics, 220 from GUM clinics) were set to achieve rate estimates with narrow confidence limits.
Between March 2002 and August 2003, women aged 16–24 years were opportunistically screened in 61 general practice, 21 family planning and 8 GUM units in Portsmouth and the Wirral, representing those of supposedly low (general practice), medium (family planning) and high risk (GUM), and invited to participate in the study.2 Clinics were paid £10 for each screening test and £15 for each woman recruited to reflect the time required for participation.
Test procedures
Women recruited into the study were tested at baseline and 6-monthly intervals for 18 months with an additional test 3 months after an initial positive. Except for the test performed at recruitment, all follow-up tests were administered outside of clinics, using a mailed test kit. This ensured that follow-up was independent of the setting of recruitment and future attendances at healthcare settings. The mailed packet (including the kit, instructions and behavioural questionnaire) was sent 3 weeks before the scheduled follow-up. Self-collected urine samples were either mailed directly to laboratories or via a participating clinic or local study office. Specimens collected on the Wirral were tested using ligase chain reaction (Abbott Laboratories, Abbott Park, Illinois, USA) according to the manufacturer’s protocols. Positive tests were confirmed by repeat ligase chain reaction using the same specimen. Specimens collected from Portsmouth from 1 March 2002 until 7 August 2003 were tested using the same protocols as those used on the Wirral. All subsequent samples (n = 996 or 30% of all study samples from Portsmouth) were tested using strand displacement assay (ProbeTec, Becton-Dickinson, New Jersey, USA) according to the manufacturer’s protocols. Positive results were confirmed by repeat strand displacement assay using the same specimen. At both sites, polymerase chain reaction (Roche Diagnostics, Basel, Switzerland) was used as the arbiter for discrepant results.
Data collection
Baseline and follow-up questionnaires were self-completed and collected information on education, healthcare attendance, contraception, last menstrual period, condom use, antibiotic use, symptoms, number of current and new sexual partners in the past 3 or 6 months, previous sexually transmitted infection or chlamydia diagnosis, and the result and management of the last chlamydia test. For each sample and questionnaire returned after baseline, women were offered £5 gift vouchers to recognise time spent for participation. An enhanced token (£20 gift voucher), approved by the local ethics committees, was used from April to July 2004 to encourage follow-up testing among recruits.
Positive women were followed by study nurses for treatment and partner notification according to established guidelines.18 A test-of-cure was performed 4 weeks after treatment. Patient-identifiable data were encrypted before submission, and databases were protected by a password and were Caldicott compliant.19
Statistical analysis
Recruited women were compared with screened women who were not recruited, regarding infection status and healthcare setting to ascertain representativeness. Recruited women with follow-up tests and those lost to follow-up were also compared, to assess retention bias of only low-risk or high-risk women contributing to follow-up time.
Women with at least one follow-up test after baseline were included for analysis of incidence and reinfection. Follow-up for negatives began at baseline and ended either on the day of the last negative test or, if earlier, the midpoint between the day of the “first positive” test and the day of the preceding negative test. Follow-up time for positive recruits (and negative recruits who converted to positive during follow-up) began after proof of negativity, defined as either clinician-confirmed patient treatment, or any documented negative test (including negative test-of-cure) after the initial positive, and ended either on the day of the last negative test or, if earlier, the midpoint between the day of the “second positive” test and the day of preceding negativity. Subgroup analysis was based on the same time at risk, and assumed that missing risk behaviour data could be “carried back” from the next period of time covered by the questionnaire.
The incidence rate was defined as the number of first positives divided by the follow-up time. The reinfection rate was defined as the number of first subsequent positive tests divided by the follow-up time. Any infection was assumed to have occurred at the midpoint between a positive test date and the preceding negative test date.20–22 Patients with two consecutive negative tests were assumed to remain uninfected during the interim.
Analysis of the overall sample for follow-up time (regardless of the clinical setting) and of the clinical setting and exposure subgroups used estimation of Kaplan–Meier failure functions, estimation of rates, testing of differences between rates using Poisson regression and estimation of unadjusted hazard ratios using Cox regression. Risk factors associated with incidence and reinfection were identified from adjusted hazard ratios using Cox regression stratified by clinical setting. This method made no assumption about the “baseline hazard” for each setting, but assumed that hazard ratios for other factors were similar for each setting and proportional at all times. We tested the proportional hazards assumption in the final multivariable model. Model variables were included, based on those found associated with chlamydia in published studies.5,6,8,9,10,13,15,16
The rate of acquisition of new male sexual partners per month was calculated from the number of new partners over the requested time period (3 months or 6 months). Partner information was reported by recruits on behavioural questionnaires and to the nurse at the time of treatment. Each study site also recorded partner testing and treatment data in a partner attendance database, linking partners to recruits. Cross-referencing revealed discrepancies in number of partners, thus the denominator for partner treatment rates was calculated in two ways: (1) maximum number recorded of either the questionnaire or that reported to the nurse (known partners); and (2) number of partners reported to the nurse at treatment (reported partners). The numerator for the partner treatment rate was derived from the partner attendance database, as this was not subject to reporting bias by recruits.
Statistical analyses were performed using Stata V.8.2 and SPSS V.12.0.
Patient consent and ethical approval
All women recruited signed a written consent form under observation by a study clinician. Ethical approval was granted by the local ethics committees in Portsmouth and the Wirral and by the former Public Health Laboratory Service Ethics Committee.
Role of the funding source
This study was funded by the Department of Health (England), which had initial input into the local study implementation and had representation on the study advisory board; however, the Department of Health was not directly or indirectly involved in data collection, analysis, interpretation or writing of the manuscript.
RESULTS
We enrolled 1971 women in the study: 547 chlamydia-positive women (78% of target of 700) and 1424 who tested negative (119% of target of 1200). A few women (n = 49, 2.5% of all recruits) were tested by cervical swab after recruitment for other concerns. Few demographic, clinical and behavioural differences between recruited women and women who were screened but not recruited were found, regardless of the healthcare setting (table 1). Cystitis and irregular bleeding were more frequently reported by negative recruits (compared with negative screens) in family planning and GUM clinics. Missing data for the questions on the reason for testing and the participant’s ethnicity were more common among screened women in general practice and family planning clinics and recruited women in GUM clinics. No differences in age, other symptoms, treatment completion and mean number of partners (positives only) were found between the women recruited and those not recruited, regardless of the healthcare setting.
Demographic, clinical and behavioural baseline characteristics of 16–24-year-old women screened for chlamydia, grouped by recruitment status, baseline infection and healthcare setting, England, March 2002–August 2003
Among recruits, chlamydia-positive women were younger than negative women. Most were of white ethnicity and tested for chlamydia as part of routine screening. A high proportion of women reported at least one symptom over the past 6 months, regardless of baseline infection status (table 1). Data from baseline questionnaires indicated that a third of negative recruits were in full-time education, the majority of recruits had been to their general practitioner in the past 2 years, and positive and negative recruits reported almost similar histories of chlamydial infection. The frequency of condom use varied and was low for both positive and negative recruits. At baseline, there were high rates of partner change among both positive and negative recruits (data not shown).
We found no differences in age, most baseline symptoms, education, healthcare attending behaviour, last menstrual period, contraceptive use, condom use, rate of new sex partner acquisition or history of chlamydial infection, regardless of the baseline infection status (negative or positive) or healthcare setting of recruitment between recruits with follow-up visits and those lost to follow-up (data not shown).
Chlamydia incidence
Of the 1424 chlamydia-negative recruits, 777 (54.6%) contributed to 839 years of at-risk follow-up time (median: 1 year in family planning and GUM clinics, 1.3 years in general practice). Incidence rates varied by healthcare setting of recruitment: 4.9 (2.7 to 8.8) per 100 person-years in general practices, 6.4 (4.2 to 9.8) in family planning clinics, and 10.6 (7.4 to 15.2) in GUM clinics (table 2), but this difference did not hold in multivariable modelling. The proportion of infections occurring within 6 months of follow-up time was 33% (7/21) among family planning recruits, 53% (16/30) among GUM recruits and 64% (7/11) among general practice recruits, increasing to 67%, 77% and 82%, respectively, by 9 months of follow-up time.
Incidence rate of chlamydial infection among 16–24-year-old women per 100 person-years by setting of recruitment and population characteristics, England, March 2002–August 2003
Among women recruited from general practices, increased incidence rates were observed in 16–17-year olds, those reporting a history of chlamydial infection, and those reporting frequent partner change, especially if condoms were not used at last sexual intercourse. For women from family planning clinics, increased incidence rates were observed in those who reported baseline symptoms, frequent urination and frequent partner change, especially if condoms were not used at last sexual intercourse. For women recruited from GUM clinics, increased incidence rates were found in those of non-white ethnicity, with a history of chlamydial infection, bleeding after sexual intercourse, and recently acquiring new partners and not using condoms at last sexual intercourse. The rate of partner change and non-condom use at last sexual intercourse were the consistent factors associated with increased infection rates across the three recruitment settings (table 2).
Multivariable modelling stratified by healthcare setting of recruitment found age 16–17 years, non-white ethnicity, report of history of chlamydia at baseline and frequent partner change as independently associated with incidence (table 3). We found evidence for an association with condom use at last sexual intercourse, only if recently acquiring new sexual partners. Women who used a condom at last sexual intercourse (regardless of their rate of partner change) and women who did not use a condom but who also did not change their sexual partner had similarly low incidence rates, 3.0 (1.2 to 7.1) and 2.2 (1.1 to 4.5), respectively, per 100 (fig 1).
Unadjusted and adjusted hazard ratios for incidence of chlamydial infection among 16–24-year-old women by setting of recruitment and population characteristics, England, March 2002–August 2003

Kaplan–Meier failure curve estimates for incidence of chlamydial infection by number of recent new male sexual partners and condom use at last sexual intercourse, 16–24-year-old women, England, March 2002–August 2003.
Chlamydia reinfection
There were 592 women at the risk of reinfection: 547 baseline chlamydia-positive recruits and 45 chlamydia-negative recruits who subsequently tested positive. Of these, 417 (70.4%) women had at least one follow-up visit and contributed 332 years of at-risk follow-up time (median: 0.7 years in family planning, 0.8 years in GUM and 0.9 years in general practice clinics). Reinfection rates for 16–24-year-old women did not vary statistically by healthcare setting of recruitment: 21.1 (14.3 to 30.9) per 100 person-years in GUM, 22.3 (15.6 to 31.8) in family planning, and 29.9 (19.7 to 45.4) in general practice (table 4). The proportion of reinfections occurring by 6 months of follow-up time was 50% (15/30) among family planning recruits, 73% (19/26) among GUM recruits and 73% (16/22) among general practice recruits, increasing to 73%, 85% and 95%, respectively, by 9 months of follow-up.
Chlamydia reinfection rates among 16–24-year-old women per 100 person-years by setting of recruitment and population characteristics, England, March 2002–August 2003
Among general practice recruits, increased reinfection rates were observed in 16–17-year olds, those reporting cystitis, those with two or more new sexual partners and those with incomplete partner treatment (table 4). For women from family planning clinics, increased reinfection rates were associated with one or more new sexual partners and incomplete partner treatment. An unexpectedly high rate was found in women whose reported partners were all treated and who used a condom at last sexual intercourse. For women from GUM clinics, increased reinfection rates were found among those reporting abdominal pain, recent bleeding after sexual intercourse or pain during sexual intercourse, those with two or more new sexual partners, and incomplete partner treatment. The most important factors for reinfection, regardless of recruitment healthcare setting, were rapid acquisition of new sexual partners and incomplete partner treatment. Small sample sizes limited the precision of reinfection rate estimates by some cofactors (table 4).
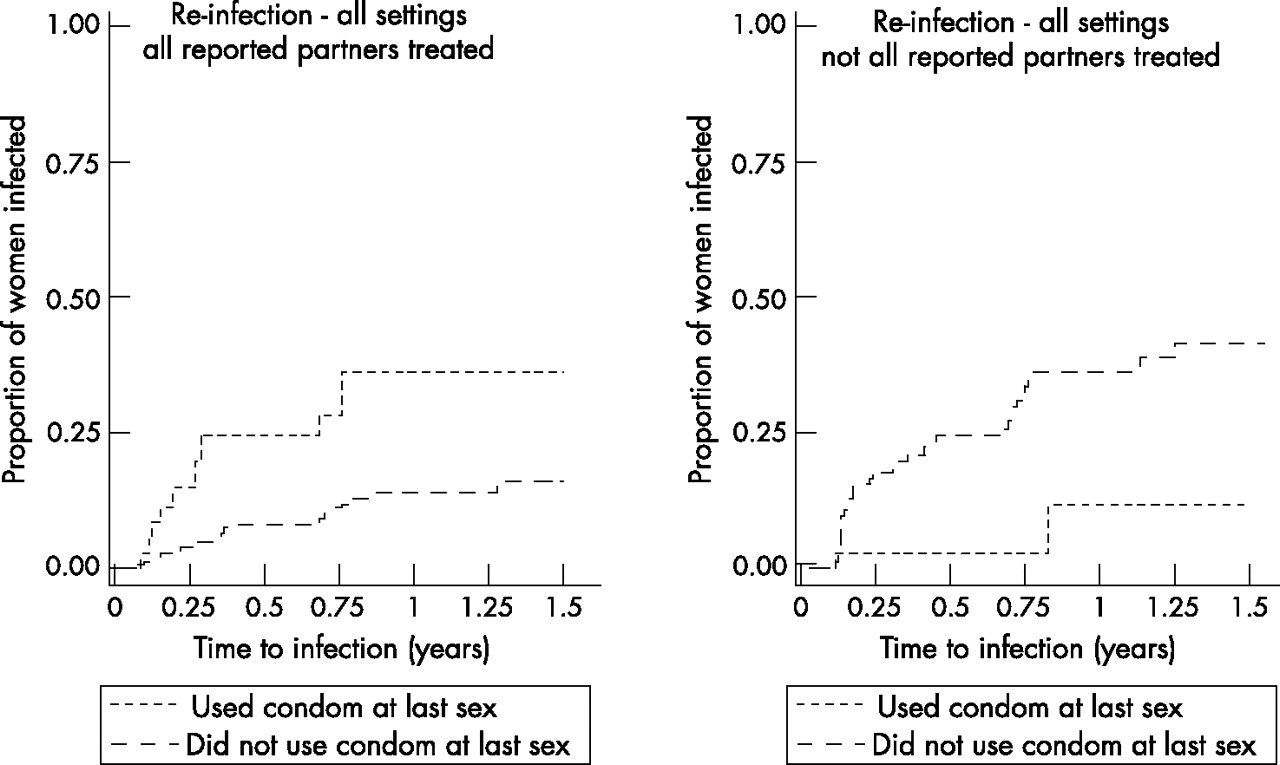
Multivariable modelling stratified by healthcare setting of recruitment found high rates of partner change and incomplete partner treatment to be independently associated with reinfection (table 5). Symptoms were excluded from the model, as they were indicators of infection. There was no evidence for an independent association with age. Evidence was found for an interaction between incomplete partner treatment and condom use at last sexual intercourse (p = 0.001). Reinfection risk increased for women who did not use condoms at last sexual intercourse if there was incomplete partner treatment; paradoxically, women with 100% reported partners treated and who used condoms at last sexual intercourse also had a higher risk of reinfection (fig 2, table 5).
Unadjusted and adjusted hazard ratios for chlamydia reinfection among 16–24-year-old women by setting of recruitment and population characteristics, England, March 2002–August 2003

{kind=link}
{kind=link}
Kaplan–Meier failure curve estimates for re-infection of chlamydia by effective partner treatment rate and condom use at last sexual intercourse, 16–24-year-old women, England, March 2002–August 2003.
DISCUSSION
Summary and comparison with other studies
Our study found chlamydia incidence rates lower (4.9/100 person-years in general practices and 6.4 in family planning clinics) than in other studies of similar populations.5,7 The rate among GUM recruits, 10.6/100 person years, was similar to that found in a study of female attenders at sexually transmitted disease clinic attenders at (11.4/100 person years)10 but significantly lower than the 27.8/100 person-years among young people reported by Richey et al.8 Factors predictive of incidence were behavioural history (chlamydial infection and recent partner change) irrespective of the clinical setting from which women were recruited. Rietmeijer et al10 noted that history of sexually transmitted infection was associated with increased risk of incidence, but this factor was not predictive in a study of adolescents in Baltimore.5 In our study, women with a history of chlamydial infection before recruitment had an incidence rate of 18.3/100 person-years, which may reflect reinfection rather than true incidence. Future incidence studies should exclude such women to ensure a truly chlamydia-naïve population for follow-up. Our findings also suggest that condom use may be protective, which could strengthen the conclusions by Morris et al,23 who found condoms to be impermeable to Chlamydia trachomatis.
Our reinfection rates were comparable to that reported by similar studies.7,10,13 As with infection, behaviours (new sexual partner acquisition and incomplete treatment of partners) were the principal risk factors for reinfection, regardless of the recruitment healthcare setting. Our findings were similar to other reports that noted age as a poor independent predictor of reinfection.16 Variations in study design, population recruited, baseline prevalence, definition and measurement of incidence and reinfection, clinical setting and country of study may account for some of these differences. Other reinfection studies have not been able to accurately account for partner change8 or partner treatment,10,16 a key strength of our study.
The effect modification of condom use at last sexual intercourse on partner treatment rates was both surprising and contradictory. We expected women who did not use condoms and who did not have partners treated to be at risk of reinfection, and our results suggest this is the case. However, the risk was also high in women who had 100% partner treatment and who used condoms at last sexual intercourse. We found that women reported more partners on the confidential questionnaire than they reported to the treatment nurse at follow-up (data not shown). It is possible that this group of women reinitiated sexual intercourse with partners not reported and for whom treatment may not have occurred. Further analysis is warranted to more thoroughly investigate this paradox.
Interpretation and implications for policy
Our results suggest that different screening intervals based on the initial screening test may be appropriate. Because incidence occurred less rapidly than reinfection, initially negative women could be screened less frequently. A protocol of annual screening (for negatives) is used in other screening programmes, based on similar evidence.4 This approach may be reasonable for the NCSP to consider in the context of their current focus in non-GUM settings, but may not be applicable to GUM clinics, as their protocols promote full sexual health screens for all attenders.
As most reinfections in our study occurred fairly quickly, more frequent screening of chlamydia-positive women may be necessary to reduce both risk of reinfection and onward transmission. Rescreening initially positive women within 6 months is the suggested protocol in the US,4 based on similar published evidence,5,6,7,8,9,10,11,13,15,16 and may be appropriate for not only the female population targeted by the NCSP but also as a policy consideration for GUM.
Researchers have highlighted the need to directly measure partner change and verify partner treatment so that the relative contribution of each could be explained.16 We have quantified the critical role that sexual partner change have in the acquisition or reacquisition of chlamydial infection. This suggests that screening for chlamydia should be more frequent among women with high rates of partner change, regardless of initial screening result. The current NCSP guidelines encourage rescreening if a woman changes her sexual partner,3 and our results indicate that this is a reasonable approach. Additionally, for reinfection, the importance of treatment of all reported partners is clear. Single-dose azithromycin treatment as first-line treatment for all partners should be considered to expedite partner treatment compliance.
Limitations
Our findings may not be generalisable to the whole population of 16–24-year-old women in England. However, there are high attendance rates for this age group at the settings from which women were recruited,17 and we found no relevant differences between the women screened but not recruited and those who joined the study in each practice setting. Furthermore, we found no differences in the factors most critical to both infection and reinfection between women with follow-up visits and those lost to follow-up, regardless of healthcare setting of recruitment, suggesting minimal loss-to-follow-up bias. We tried to control for any underlying differences between the recruitment settings by stratifying our multivariable Cox regression model that assessed predictors of infection and reinfection. Even so, firstly, combining all practice settings in multivariable analysis may mask important differences between the clinic populations and further studies following a larger number of women within each setting may be warranted. Secondly, retrospective behavioural data may be subject to recall bias, as was noted in the under-reporting of partners. Other factors that may influence chlamydial infection or reinfection, such as treatment failure or partners having sexual intercourse with other partners, were not recorded. Thirdly, our study was limited to women only, and further studies are needed to evaluate screening intervals for men. Finally, less than optimum sample sizes and follow-up rates reduced the precision of our setting-specific estimates. However, women were followed up for longer and at more frequent intervals while maintaining an overall retention rate comparable with other published studies.6,7,11,16
CONCLUSION
In this first prospective cohort study of chlamydia incidence and reinfection among young women attending general practice, family planning and GUM settings in England, we have shown that age, partner change (modified by condom use) and history of chlamydial infection are the best predictors of incidence, and have quantified and shown the pivotal role of partner change and incomplete partner treatment in the risk of chlamydia reinfection. On the basis of this study, annual screening for 16–24-year-old women seems reasonable, and screening intervals should depend on the result of the initial screening test, combined with partner change and partner treatment data: (1) if the initial screening is negative, continue annual chlamydia screening unless a new sexual partner is acquired; (2) if the initial screening is positive, rescreening should occur within 6 months, or sooner if a new sexual partner is acquired or there is evidence of an untreated partner.ii Condom use should be advocated; however, the mixed influence of condom use on infection and reinfection requires further study before consideration within the construct of screening intervals recommendations.
Key Messages
-
The incidence rate of chlamydial infection was 4.9 (2.7 to 8.8) per 100 person-years among 16–24-year-old women recruited from general practices, 6.4 (4.2 to 9.8) from family planning and 10.6 (7.4 to 15.2) from genitourinary medicine (GUM), and was higher in 16–17-year olds, those with a history of chlamydial infection, and those recently acquiring new sexual partners. If recently acquiring new partners, condom use at last sexual intercourse was found to be independently associated with lower incidence.
-
The chlamydia reinfection rate was 29.9 (19.7 to 45.4) per 100 person-years from general practices, 22.3 (15.6 to 31.8) from family planning clinics and 21.1 (14.3 to 30.9) from GUM clinics, and was higher in 16–17-year olds, those recently acquiring new sexual partners, and those with incomplete partner treatment from the initial positive test. An unexpectedly high reinfection rate was found in women whose reported partners were all treated and who did use a condom at last sexual intercourse.
-
Our findings suggest annual screening for women aged 16–24 years. If the initial screening is negative, continue annual screening unless a new sexual partner is acquired. If the initial screening is positive, rescreen within 6 months or sooner if there is incomplete partner treatment or acquisition of a new sexual partner.
Acknowledgments
We thank the Department of Health (England) for generous funding and their support for this study. We also thank the contributions of general practices, contraceptive/family planning clinics, genitourinary medicine and laboratories in providing facilities for seeing patients and processing specimens. We acknowledge additional contributions made to this study by the following: Dr Mike Catchpole for assistance with the original study design and funding acquisition; Dr Jeanne Pimenta for assistance with study design and methodology and initial project management; Mrs Pauline Rogers for assistance with study protocol and design, statistical methodology and sample size calculations, and design of data collection forms and database; Mr Nick Richardson for development and maintenance of database and data management software; and Dr Katherine Turner and Ms Elisabeth Adams for insightful comments on the manuscript.
REFERENCES
Footnotes
-
↵i Note from principal author: Our study was designed during the original pilot of chlamydia screening in Portsmouth and the Wirral17 and implemented before the decision for a national screening programme that would exclude GU medicine and include men. We present results for women recruited from GU medicine, but recognise that the standards of care regarding chlamydial infection are dictated by different guidelines.
-
↵ii A separate manuscript in this journal presents the results of a transmission dynamic modelling study of the screening interval recommendations from this study to assess whether this recommended screening strategy, or others currently in use, can be used to achieve effective chlamydia control by reducing prevalence and transmission in the target population.24
-
Published Online First 18 October 2006
-
Funding: Funding for this study was provided by the Department of Health (England), Skipton House, 80 London Road, London SE1 6LH, UK. The opinions of the authors are reflective of the Chlamydia Recall Study Advisory Group and do not necessarily represent the views of the Department of Health (England).
-
Competing interests: None.
-
Guarantor statement: I, D Scott LaMontagne, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Contributions: DSL was the lead investigator for the study from April 2003, supervised the study implementation, developed the plan and analysed study data in collaboration with statisticians and study coordinator, interpreted study findings, and was the principal author of the manuscript. KB was the statistician for the study, developed the plan and analysed study data in collaboration with the lead investigator and study coordinator, interpreted study findings, and coauthored the manuscript. LE was the study coordinator from March 2004, oversaw local data collection, collated and cleaned all study data, developed the plan and analysed study data in collaboration with lead investigator and statistician, interpreted study findings, and coauthored the manuscript. TN was the statistician during the revisions’ process, gratefully covering for KB while she was on maternity leave.
In addition to reviewing and commenting on final drafts of the manuscript, the following authors had these additional contributions: SR assisted in developing the local study protocol, and was lead clinician in Portsmouth for the study; LML was responsible for management of the study in Portsmouth, including subject recruitment, follow-up of recruits, patient and partner clinical management, and local data collection; PM was responsible for management of the study in Portsmouth, including subject recruitment, follow-up of recruits, patient and partner clinical management, and local data collection; VH assisted in developing the local study protocol and managed patients from GUM in the study; JMT assisted in developing the local study protocol and recruitment and management of patients from GUM in the study; GSU participated in protocol development and was responsible for the laboratory aspects of the study in Portsmouth; WGH performed local database administration, supervising implementation and integrity of the research database software; JH assisted in developing the local study protocol, and was lead clinician in the Wirral for the study; TG was responsible for management of the study in Wirral, including recruitment, follow-up, management of those screened positive and data collection; AKG supervised the local study implementation in the GU department of Arrowe Park Hospital, Birkenhead; HM assisted in developing the local study protocol and was responsible for laboratory testing the samples collected from study subjects in Birkenhead, and supervised the local data collection and database management; ARD coordinated the data management and was involved in data analysis and interpretation of results in the early stages of the study; GH was the original principal investigator and study manager (until March 2003) who developed the study idea, designed the study, wrote the protocol and acquired the funding; and KAF was an investigator and senior epidemiologist on the project, contributed to its design, implementation and was a previous guarantor of the study.
Linked Articles
- Editorial