Article Text

Abstract
This study aimed to systematically review and describe the evidence on chlamydia and gonorrhoea reinfection among men, and to evaluate the need for retesting recommendations in men. PubMed and STI conference abstract books from January 1995 to October 2006 were searched to identify studies on chlamydia and gonorrhoea reinfection among men using chlamydia and gonorrhoea nucleic acid amplification tests or gonorrhoea culture. Studies were categorised as using either active or passive follow-up methods. The proportions of chlamydial and gonococcal reinfection among men were calculated for each study and summary medians were reported. Repeat chlamydia infection among men had a median reinfection probability of 11.3%. Repeat gonorrhoea infection among men had a median reinfection probability of 7.0%. Studies with active follow-up had moderate rates of chlamydia and gonorrhoea reinfection among men, with respective medians of 10.9% and 7.0%. Studies with passive follow-up had higher proportions of both chlamydia and gonorrhoea reinfections among men, with respective medians of 17.4% and 8.5%. Proportions of chlamydia and gonorrhoea reinfection among men were comparable with those among women. Reinfection among men was strongly associated with previous history of sexually transmitted diseases and younger age, and inconsistently associated with risky sexual behaviour. Substantial repeat chlamydia and gonorrhoea infection rates were found in men comparable with those in women. Retesting recommendations in men are appropriate, given the high rate of reinfection. To optimise retesting guidelines, further research to determine effective retesting methods and establish factors associated with reinfection among men is suggested.
- EPT, expedited partner treatment
- NAAT, nucleic acid amplification test
- STI, sexually transmitted infection
Statistics from Altmetric.com
- EPT, expedited partner treatment
- NAAT, nucleic acid amplification test
- STI, sexually transmitted infection
Chlamydia and gonorrhoea are the two most common bacterial sexually transmitted infections (STIs) in the US, with 929 462 (319.6 per 100 000 population) and 330 132 (113.5 per 100 000 population) reported cases, respectively, in the US and district of Columbia during 2004.1 Serious complications associated with chlamydia and gonorrhoea include chronic pelvic pain, infertility, ectopic pregnancy and pelvic inflammatory disease in women, as well as proctitis and epididymitis in men.2–6 Although the treatment efficacy of first line drugs for both chlamydia and gonorrhoea infection is high,2,3,7,8,9,10,11 the problem of reinfection remains.2,3,12
The prevalence of recurrent chlamydial infection is especially well documented in young and unmarried women, ranging between 6% and 23% within 6 months of treatment.13–19 As a result, the 2002 US Centers for Disease Control and Prevention treatment guidelines recommended that all women with chlamydial infection be tested for reinfection (different from test of cure) at 3–4 months after treatment.20 Although some local health departments recommend retesting men for STIs, there are no established national retesting guidelines for either gonococcal infection in women, or chlamydial or gonococcal infection in men, partly owing to the limited data available for guideline development.
In the US, there has been a 46.6% increase in reported cases of chlamydia in men from 1999 to 2004,1 probably as a result of increased screening and diagnoses of chlamydial infections with the advent of highly sensitive and non-invasive nucleic acid amplification tests (NAATs). Although incident chlamydia tends to be higher in women,1 some recent studies have found that the prevalence of chlamydial infection in young men is comparable with that of young women at 7–15%.21–27
Focusing screening and treatment only on women will not effectively reduce the overall prevalence of both chlamydia and gonorrhoea in the US because their male partners might remain infected.2,3,25,28 Given that untreated male partners are a likely source of reinfection among women following treatment and that men exhibit high rates of asymptomatic infections, it is important to evaluate the need for extending screening guidelines for chlamydial and gonococcal reinfection to men as a means of reducing recurrent chlamydial and gonococcal infection in both men and women. Although several studies implementing expedited partner treatment (EPT) have demonstrated significant decreases in reinfection among women, a considerable proportion of reinfection occurred despite treating existing partners.29,30 Thus, retesting men might be another important prevention strategy.
Earlier literature from the 1970s and 1980s has examined the role of retesting in reducing morbidity from gonococcal reinfection during those decades.31–34 However, there is no recent compilation of the literature about gonococcal reinfection in men and no review has been published to date about chlamydial reinfection in men. We systematically reviewed and described the current evidence of recurrent chlamydial and gonococcal infection among men, focusing on studies using the most sensitive and specific tests. Our results might be useful in developing retesting guidelines for men.
METHODS
We searched for published or presented scientific literature regarding chlamydial and gonococcal infection, reinfection, retesting and screening recommendations for men. Using PubMed, we used combinations of search terms including “repeat gonorrhea chlamydia”, “recurrent gonorrhea chlamydia”, “repeat gonorrhea”, “repeat chlamydia”, “persistent gonorrhea”, “persistent chlamydia”, “rescreening gonorrhea”, “rescreening chlamydia”, “retesting gonorrhea” and “retesting chlamydia” to find literature published between January 1995 and October 2006. Literature from previous decades was excluded because of differences between current and past disease trends. We searched for scientific abstracts from the US and International STI conferences from January 2000 to August 2006. For relevant conference abstracts, actual posters and/or presentations were reviewed to facilitate data abstraction. To maximise the search, we examined the articles of people known to be involved in the research of chlamydia and gonorrhoea and searched the bibliographies of relevant papers. Finally, we contacted eight authors of relevant articles to acquire any unpublished data.
All studies included men and reported chlamydia, gonorrhoea, or chlamydia and gonorrhoea combined data as well as gender-specific data. Included studies also had a follow-up period starting at least 2 weeks after treatment of initial infection and used NAATs for chlamydia and NAATs or culture for gonorrhoea to ensure consistent sensitivity and specificity of test results. There is a significant difference in test performance of chlamydia NAATs and of older tests for chlamydia,2,35 but little difference between gonorrhoea NAATs and gonorrhoea culture.2,36,37 However, studies varied in whether there were age restrictions for their participants or restrictions by gender of partners. Several studies were excluded for not including gender-specific data,38 not restricting to laboratory-confirmed chlamydia and/or gonorrhoea at baseline39 and not including organism-specific data.40–42
Studies were classified on the basis of the follow-up method: active follow-up as in a prospective cohort study design versus passive follow-up through disease or clinic registries. To standardise reported measures, we calculated the overall proportion of reinfected individuals and defined it as the number of reinfected individuals per followed-up enrollees. Data abstracted from studies were summarised in tables. We report the median as the measure of central tendency to account for the variation in studies, and also report the range. We plotted estimates of proportions of reinfection by study.
RESULTS
Our initial search of PubMed returned 71 articles for “repeat gonorrhea chlamydia”, 19 articles for “recurrent gonorrhea chlamydia”, 53 articles for “repeat gonorrhea”, 108 articles for “repeat chlamydia”, 51 articles for “persistent gonorrhea”, 417 articles for “persistent chlamydia”, 5 articles for “rescreening gonorrhea”, 9 articles for “rescreening chlamydia”, 6 articles for “retesting gonorrhea” and 31 articles for “retesting chlamydia.” Numerous duplicates were found among the various search terms. Of these, 12 published articles tested men and met our inclusion criteria of having a follow-up period and using NAATs for chlamydia testing and using NAAT or culture for gonorrhoea testing.29 In addition, one presentation and one poster from national and international STI conferences met our inclusion criteria.43,44 Reviewed studies were published or presented between 2000 and 2006, with data collected from 1992 to 2004. Tables 1 and 2 provide a select summary of the 14 reports.29,45–5657
Data abstracted from studies with active follow-up of chlamydial and gonococcal reinfection among men
Data abstracted from studies with passive follow-up of chlamydial and gonocaccal reinfection among men
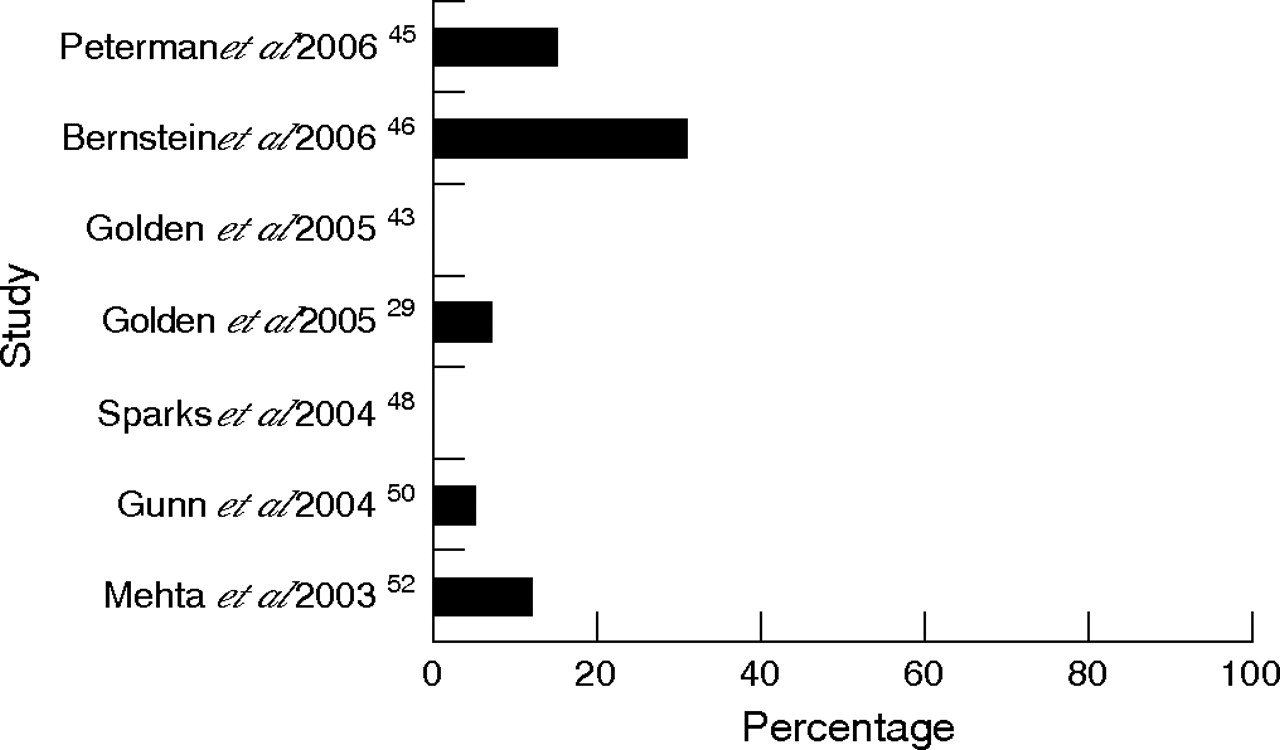
Of the 14 studies, 5 investigated both chlamydial and gonococcal reinfections, 4 studied only chlamydial reinfection and 3 studied only gonococcal reinfection. The proportion of men with repeat chlamydia ranged from 9.8%45 to 18.3%,53 with a median of 11.3% (fig 1). The proportion of men with repeat gonorrhoea ranged from 0%43,48 to 30.8%,46 with a median of 7.0% (fig 2).
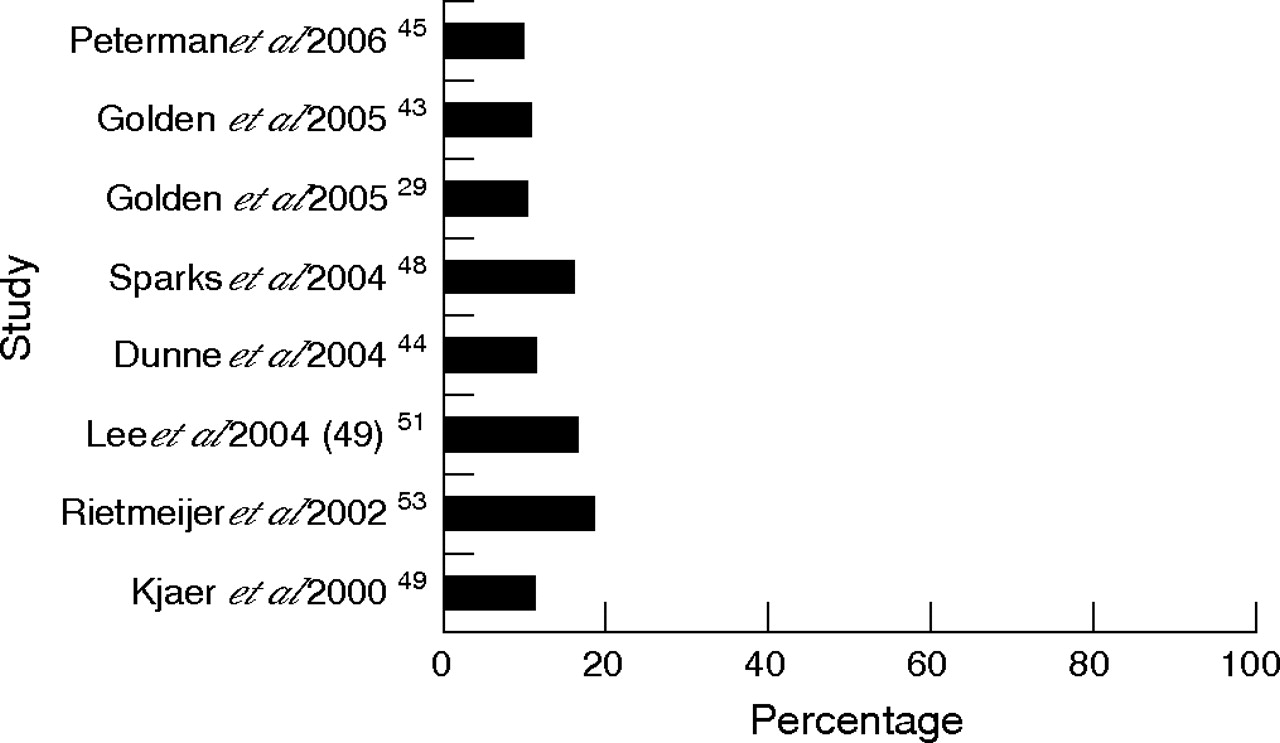
Percentage of chlamydial reinfection among men by study.

{kind=link}
{kind=link}
Percentage of gonococcal reinfection among men by study.
Follow-up periods for the studies with active follow-up ranged from 10 weeks48 to 24 weeks,49 with a median of 4 months. By contrast, the studies with passive follow-up allowed for repeat infection definitions up to a maximum of 4.8 years52 from initial infection. The studies with active follow-up had moderate proportions of repeat chlamydia and gonorrhoea among men, with respective medians of 10.9% and 7.0%. Follow-up rates to obtain these estimates ranged from 24.3%46 to 83.3%,45,49 with a median of 62.4%. The studies with passive follow-up had higher proportions of both chlamydial and gonococcal reinfection among men, with respective medians of 17.4% and 8.5%. The follow-up rate of the studies using passive follow-up was indeterminable.
In the studies accounting for infection in both sexes, the proportions of repeat chlamydia and gonorrhoea among men were comparable to those among women. The proportions of chlamydial reinfection among males was only slightly lower,29,45,49,50,53 and in two studies higher,43,48 than those among women. A study in three major US cities with active follow-up by a scheduled 3-month STD clinic visit found a repeat chlamydia proportion among men at 9.8% comparable with that among women at 10.7%.45 A study with passive follow-up found a similar trend with a chlamydial reinfection proportion among men at 18.3% only slightly lower than that among women at 23.2%.53
The proportions of repeat gonorrhoea among men were either nearly equal29 or slightly above those among women.46,50,52 A study with active follow-up by scheduled clinic visit or disease investigation specialist found a repeat gonococcal infection proportion among men at 30.8% to be slightly higher than that among women at 28.9%.46 Similarly, a passive study found gonorrhoea among men at 5.0% to be greater than that among women at 4.1%.50
Some studies only presented combined chlamydial or gonococcal reinfection data. In these studies, combined chlamydial or gonococcal reinfections among men were either equal to54 or even higher than those among women.55 One study with passive follow-up in North Carolina found repeat infection among men to be higher than that among women, with respective reinfection proportions of 28.3% and 19.0%.55
One study specifically focused on the effect of treatment of partners on reinfections rates and showed that increased treatment of partners reduced the amount of chlamydial and gonococcal reinfection among men.29 This study found that with standard referral, repeat chlamydia among men and women was nearly equivalent at 12% and 13%, respectively, and with EPT, repeat chlamydia among men at 7% was lower than that in women at 11%.
Analysis of factors associated with chlamydial and gonococcal reinfection among men found that a history of STIs was consistently predictive of reinfection with either or both infections.44,45,54,55 Reinfection in either sex was also strongly associated with having untreated partners43,45,46,50 and the demographic factors of younger age29,50,52,53,55 and non-white race.45,55 High-risk sexual behaviour, including not using condoms, change in partners and higher number of sexual partners inconsistently, was associated with an increased risk for repeat infection.29,45,51,52
DISCUSSION
The reviewed studies provide strong evidence for the substantial incidence of chlamydial and gonococcal reinfection among men. The proportions of repeat chlamydial infection among men had a median of 11.3% and ranged from 9.8% to 18.3%. Proportions of repeat chlamydia among men were similar to those among women. Such data are especially significant because current retesting guidelines only recommend chlamydia rescreening in women 3 months after initial infection.20 Although initial incident chlamydial infection may be higher in women than in men,1 probably due to shorter duration of natural clearing of infections in men, the reinfection data suggest that chlamydial reinfection rates among men are similar to those among women, and may contribute to continued infections in women.
The proportions of repeat gonococcal infection among men in the reviewed studies had a median of 7.0% and ranged from 0% to 30.8%. Proportions of repeat gonococcal infection among men were similar to those among women. There are currently no gonorrhoea retesting guidelines for either men or women, probably owing to the decreased reported national incidence of gonorrhoea and more limited recent data about reinfection. Because the studies we reviewed indicated that proportions of repeat gonococcal infection among men are equal if not higher than those of repeat chlamydia among women, retesting men after initial treatment might be effective in reducing the prevalence of gonorrhoea among both men and women.
A history of STIs and the demographic factors of younger age and non-white race were strongly associated with chlamydial and gonococcal reinfection. Data from the studies indicate an inconsistent association between reinfection and risky sexual behaviours such as increased number of partners and not using condoms. Because no specific behavioural factors predict reinfection, all chlamydia- or gonorrhoea-infected men should be retested for reinfection.
Certain factors limited the findings of this review. The search strategy could have possibly overlooked relevant studies, although numerous steps were taken to prevent this oversight. The search on PubMed was limited to English-only sources, thus possibly excluding studies from non-English-speaking countries with high prevalences of chlamydia. Most importantly, there is little published literature documenting repeat chlamydial and gonococcal infection.
Major discrepancies in reported reinfection proportions were due to the variation of study designs. The studies had either active or passive follow-up in their design and so used a wide range of different follow-up periods. The longer follow-up periods for many passive studies compared with active follow-up studies (years vs months) allowed more people to become reinfected with time, yielding higher median reinfection proportions in passive studies than in active follow-up studies. In addition, all study designs might be affected by a differential return for follow-up among symptomatic and asymptomatic individuals. Given that symptomatic people are more likely to return than asymptomatic people, this would cause an overestimate of the true rate of reinfection. Studies with passive follow-up, which depend on people seeking services, are especially vulnerable to this bias.56 In addition, the studies with active follow-up experienced variable follow-up rates ranging from 24.3% to 83.3%, which may also differentially account for asymptomatic infections.
Although current recommended treatments for both chlamydia and gonorrhoea show low instances of treatment failure,2,3,7,8,9,10,11 all studies attempted to account for persistent chlamydial or gonocaccal infection due to treatment failure by eliminating data within certain time periods of initial treatment. Most of our reviewed studies looked at high-risk populations, which may limit the widespread generalisability of our results. Most data were collected at or from records of public STD clinics where only a minority of reported cases of infection are detected in men: 36% of chlamydia and 45% of gonorrhoea.1
Despite these limitations, our review clearly established the considerable proportion of repeat chlamydia and gonorrhoea among men comparable with that among women. Although one of the studies suggests effective reduction of repeat chlamydial and gonococcal infection with EPT,29 a substantial proportion of repeat infection remains. Even with the widespread implementation of EPT, proportions and incidences of both chlamydial and gonococcal reinfection might remain high.
Given the limited resources and the need for focused interventions, targeting previously infected men for retesting might disproportionately reduce the transmission of chlamydia and gonorrhoea, thereby reducing reinfection in women and their subsequent adverse sequelae. Our analysis of the current body of literature established substantial proportions and incidences of repeat chlamydia and gonorrhoea among men that are similar to those among women consistent across studies, suggesting that retesting of all chlamydia- and gonorrhoea-infected men at 3 months after initial treatment should be recommended. We recognise the challenge in implementing successful retesting programmes38,43 and suggest additional research to optimise retesting procedures and establish rates of repeat infection in other populations as a means to further refine retesting guidelines for chlamydial and gonococcal infections among men.
REFERENCES
Footnotes
-
Published Online First 13 December 2006
-
Competing interests: None declared.
Linked Articles
- Editorial