Article Text

Abstract
Objectives: This report updates the UK epidemiology of lymphogranuloma venereum (LGV) to the end of April 2007.
Methods: The Health Protection Agency’s Centre for Infections undertakes laboratory testing for LGV and subsequent epidemiological investigation of cases after laboratory confirmation of the LGV serovars (L1–3). Data analysis of enhanced surveillance and laboratory reports was undertaken.
Results: From October 2004 to end April 2007, 492 cases of LGV have been diagnosed and enhanced surveillance forms have been returned for 423. Cases peaked in the third quarter of 2005 with an average of 32 cases per month, while in 2006 this fell to 12 cases per month. Nationally, the outbreak is focused in London, Brighton and the North West. All cases are in men, 99% of whom are MSM, with a median age of 40 and predominantly white ethnicity (91%). Co-infection remains considerable: HIV (74%); hepatitis C (14%); syphilis (5%); and other STIs including gonorrhoea, genital herpes and hepatitis B. The number of men reporting greater than 10 sexual contacts in the previous 3 months has reduced from 23% (47) to 13% (15) from 2005–2006.
Discussion: The epidemic continues in the mostly white MSM population of the UK. The demographics of LGV remain similar to those previously described and high levels of HIV co-infection continue. Reduced numbers of sexual contacts might be contributing to the reduced numbers of LGV seen in 2006 but could simply mean that LGV is moving out of the highest risk groups.
- LGV, lymphogranuloma venereum
- MSM, men who have sex with men
- STBRL, sexually transmitted bacterial reference laboratory
Statistics from Altmetric.com
- LGV, lymphogranuloma venereum
- MSM, men who have sex with men
- STBRL, sexually transmitted bacterial reference laboratory
Prior to 2004, lymphogranuloma venereum (LGV) was predominantly a tropical disease, rarely seen in the UK. Following the emergence of this disease in the Netherlands and other parts of Europe,1–4 an epidemic is now well established in the UK.5,6 Similar to the ongoing outbreaks of LGV in Western Europe and America, the epidemic is concentrated in the MSM population with high levels of HIV co-infection.7 As initially little was known about the transmission and symptoms of this disease, enhanced surveillance was set up in the UK to collect information on demographics, transmission and clinical presentation.6
This report presents updated data on the epidemiology of LGV in the UK, 14 months on from the last report in 2006, and outlines the changes that are occurring in clinical presentation of the disease through time as well as changes in patient behaviour in terms of sexual networks.
METHODS
The methods for LGV referral for laboratory testing and referral policy have been extensively outlined in a previous report.6 In brief, the Sexually Transmitted Bacterial Reference Laboratory (STBRL) tested rectal specimens from patients with anorectal symptoms (typically proctitis and rectal discharge), or urethral specimens from patients with inguinal lymphadenopathy who were known to be positive to C. trachomatis. Surveillance of LGV began in 2004 and the epidemiological questionnaire on laboratory confirmed cases collects information on demography, sexual behaviour, sexual networks, co-infection with other STIs including HIV and HCV, detailed information on clinical presentation, and therapy. All protocols produced by the incident team and the Health Protection Agency’s Centre for Infections (HPA CfI) are posted on the HPA website (http://www.hpa.org.uk).
The chlamydia status of specimens was determined using a plasmid based in-house real-time PCR assay.8 From October 2004 to September 2005 genotyping of the samples positive for C. trachomatis was performed using ompI RFLP-PCR by the methods of Lan et al9,10 From September 2005 samples were genotyped using the method of Morre et al11 using a real time PCR that differentiates between LGV and non-LGV associated serovars, with the differentiation of L1, L2 or L3 being performed by the method of Lan et al9,10
Analysis
Differences in proportions of symptoms between time categories were assessed using χ2 tests of association.
RESULTS
Diagnostic testing
Between 4 October 2004 and 30 April 2007, the STBRL received 3277 specimens for LGV diagnostic testing. STBRL was unable to test 183 specimens due to incorrect specimen referral or lack of clinical information. Of the 3094 specimens processed, the presence of C. trachomatis specific DNA was detected in 2651 specimens. Details regarding rates of specimen confirmation have been reported elsewhere.12
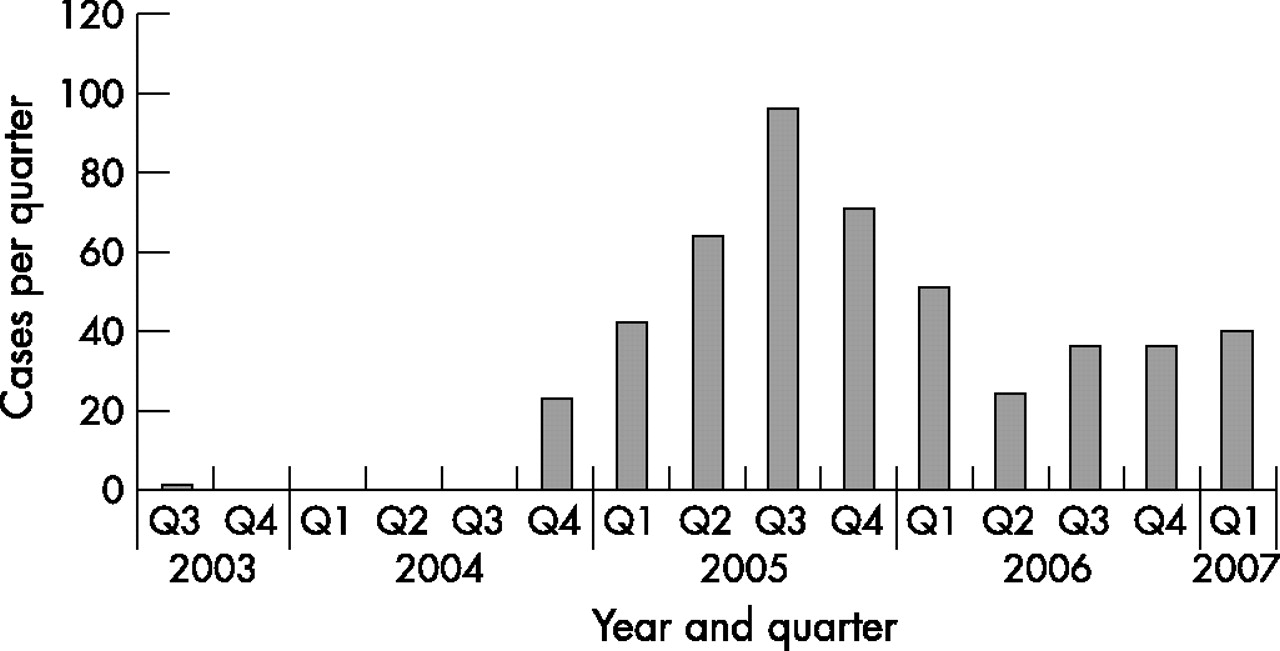
A total of 492 LGV positive specimens have been identified using a combination of ompI RFLP-PCR (October 2004 through September 2005)6 and a LGV specific real-time PCR followed by ompI RFLP if positive (after September 2005).11 This is an additional 165 cases since the last report.6 Full ompI RFLP genotyping has been performed on 470 of the LGV positive specimens, of which 426 were confirmed as L2, 33 were untypable due to low DNA loads, and 11 were found to have non-LGV associated C. trachomatis profiles probably due to patients having infections with mixed serovars of C. trachomatis. Figure 1 shows the epidemic curve to the end of April 2007, based on numbers of laboratory confirmed cases. Cases peaked in the third quarter of 2005 with an average of 32 cases per month, while in 2006 this fell to 12 cases per month.

{kind=link}
Numbers of laboratory confirmed cases of LGV, by quarter of diagnosis, for United Kingdom. Cases from 2003 are based on stored samples that were retrospectively tested.
Enhanced surveillance
GUM clinics returned reports on 423 cases of LGV cases to the enhanced surveillance system, 419 (99%) from MSM, 3 from heterosexual men and 1 of unspecified sexuality. The majority of cases were of white ethnicity (91%; 387/423) with a median age of 40 years (range 24 to 69). Although cases have been received from all over the UK, including Scotland and Wales, the majority were seen in London (74%; 313/423) and Brighton (10%; 44/423). Of the London cases, 175 (56%) occurred in 2005, compared with 99 cases (32%) in 2006. Similarly in Brighton the greatest number of cases occurred in 2005, 37 (84%) compared with 4 (9%) in 2006. The North West region has the next largest cluster with 16 cases.
Clinical presentation
Most LGV cases (82%, 346/423) presented because of symptoms, others presented as contacts (5%, 20/423), through referral (4%, 15/423), or were detected during routine examination (5% 22/423) and screening for STI or HIV. In 2004–5, 90% of cases presented with proctitis and 24% with systemic symptoms, compared with 77% (p = 0.001) and 15% (p = 0.04) in 2006/7. In 2006/7 18% (24) were reported as having not presented with at least one of the symptoms of proctitis, genital or systemic symptoms. This compares with only 5% (15) of those presenting in 2004/5. Almost all (88 of 89) with systemic symptoms also had proctitis.
Co-infection
HIV co-infection was present in 74% (312/423) of cases while hepatitis C co-infection was seen in 14% (57/411, 12 non-respondents). Other concurrent STIs were documented in 48% (205/423) of cases, including gonorrhoea (78), syphilis (21), other non-LGV chlamydial infection (20), genital herpes (11) and hepatitis B (1).
Sexual networks
Data on sexual behaviour and networks for meeting partners are limited due to the nature of the surveillance, and there are a lot of missing data. However, overall, 35% of men (149/423) reported meeting new sexual partners at sex on premises venues or sex parties, and 38 (9%) via the Internet. Most LGV (78%) was thought to have been acquired in the UK. Possible acquisition abroad was noted mostly in the Netherlands and Spain. In 2005 24% (47 men) reported sexual contact with more than 10 men in the previous 3 months, while in 2006 this had dropped to 14% (15 men, p = 0.04; table 1). Table 1 also shows the large numbers of untraceable contacts reported by men with LGV. From 2004 to date, the majority of men (65%; 274/423) reported unprotected anal sex. Fisting and the use of sex toys were reported by 28 (11%) and 15 (6%) men respectively. These findings have remained constant the during this time period.
LGV sexual networks: total contacts and traceability
DISCUSSION
The first detailed description of the LGV epidemic outlined trends for the first 17 months of the UK epidemic6 and showed that cases were focused on mainly white MSM with high levels of HIV and hepatitis C co-infection. This update shows that during the subsequent 14 months, the demographics have remained similar to those previously described, with infection concentrated in the same groups and clustering in certain large urban areas.
Despite this, some changes in the epidemic are becoming apparent as the epidemic continues to unfold in the UK. Firstly, the diagnosed incidence has declined from a peak in 2005 and cases are at a more endemic level. A similar picture has recently been reported in the Netherlands.13 This could reflect a decrease in awareness after the initial interest in the epidemic, but this is not supported by data on numbers of specimens referred for testing which has increased over time. From 2004, the Terrence Higgins Trust mounted large campaigns aimed at MSM, distributed via clubs, GUM clinics and the internet.14,15 These, together with alerts and publications to health professionals, increased awareness and could have contributed to the observed reduction as cases presented and were diagnosed and treated, thus preventing ongoing transmission. Secondly, more recent cases report significantly fewer sexual partners. This could indicate that LGV is moving out of the highest risk groups into MSM of somewhat lower risk status, which could in turn be reducing transmission. If this is the reason it could be a worrying development as the number of susceptibles within a lower risk group are considerably more and might be harder to reach, increasing the possibility of an ongoing endemic phase to this outbreak. Thirdly, the clinical presentation of LGV also appears to be changing. Initially there was a predominance of proctitis and systemic symptoms, but whilst proctitis remains the commonest symptom (77% of those diagnosed in 2006/7) it is decreasing. Further detailed work on the clinical presentation is required.
It is too early to say we have the outbreak under control given the overall number of cases, but a reduction in the number of cases is encouraging and the earlier presentation and treatment is indicative of good clinical care, especially given all the pressures on GUM clinic services currently.
Acknowledgments
The authors would like to thank Pamela Saunders and Ucheoma Ugoji for processing many of the LGV specimens at STBRL, and the many clinicians and microbiologists who have contributed to the enhanced surveillance program. We also acknowledge Neil Macdonald and Iona Martin, who initially set up the enhanced surveillance system and diagnostic testing systems respectively.
REFERENCES
Footnotes
-
↵* Helen Maguire, (Health Protection Agency London Epidemiology Unit); Lesley Wallace (Health Protection Scotland); Andrew Winter (Sandyford Initiative); Pat Munday (British Association for Sexual Health and HIV, and West Hertfordshire Hospitals NHS Trust); Patrick French (University College London Hospital); Will Nutland (Terrance Higgins Trust); Neil Irvine (Health Protection Agency Northern Ireland); Alexander McMillan (Edinburgh Royal Infirmary), Ann Sullivan (Chelsea & Westminster Hospital).
-
Competing interests: HW is co-editor and CI is an associate editor of STI.
Linked Articles
- Editorial