Article Text

Abstract
Objective: This study compared failure rates of a standard-sized condom and a condom fitted to a man’s penile length and circumference and assessed users’ perceptions of condom acceptability and confidence in the efficacy of both condoms.
Method: Using an experimental crossover design with Internet-based daily diaries, 820 men who wore at least one of each condom type reported outcomes and perceptions of condoms used during vaginal and anal intercourse events for which they were the insertive partner.
Results: Breakage for fitted condoms (0.7%) was significantly less than for standard-sized condoms (1.4%). When assessed by penile dimensions, significantly less breakage of fitted condoms than standard-sized condoms was observed among men in the middle circumference category (12–13 cm) during anal intercourse (1.2% versus 5.6%), men in the larger circumference category (⩾14 cm) during vaginal intercourse (0.6% versus 2.6%), and men in the longer length category (⩾16 cm) for both vaginal (0.5% versus 2.5%) and anal (3.0% versus 9.8%) intercourse. More slippage upon withdrawal after vaginal intercourse occurred with fitted condoms among men in the middle penile length (1.9% versus 0.9%) and circumference (2.2% versus 0.7%) categories.
Conclusions: Fitted condoms may be valuable to sexually transmitted infection prevention efforts, particularly for men with larger penile dimensions. That fitted condoms slipped more for some men provides insights into the need for unique educational materials to accompany such products. Findings also highlight the need for participatory approaches between public health, condom manufacturers, and the retail industry to integrate fitted products into our work successfully.
Statistics from Altmetric.com
Men’s complaints about the fit and feel of condoms have anecdotally and empirically been associated with inconsistent and incorrect condom use.1–5 Penile dimensions vary6–11 and researchers have documented associations between penile dimensions and condom failure rates,1 12–15 which typically fall in the range of less than 1% to approximately 5%.16–25
Although some have called for manufacturers to expand the condom sizes available, to date the industry has offered only limited access to condoms of different sizes. As it does so, it will be important to examine the impact of these new products and their potential for improving sexually transmitted infection (STI) prevention outcomes. This study compared men’s reports of breakage and slippage, ratings of confidence in, and acceptability of, a standard-sized condom and an individually fitted condom.
METHODS
Participant recruitment
Recruitment advertisements were placed in newspapers and at HIV/STI-related organisations in seven geographically diverse US states that have disproportionate STI prevalence, and on sexuality-related websites. Eligibility requirements included being a sexually active adult man who used condoms for sexual activity, agreed to continue any non-condom contraceptives, and had no known allergies or adverse reactions to latex or silicone-based products.
Data collection
An experimental crossover design utilising Internet-based daily diaries was used. The study website described the study’s purpose and methods and stressed relations between penile measures participants would be asked to provide and the size of the fitted condoms that they would receive. After signing an electronic consent form, participants printed study instructions and tools for penile measurement. Men not meeting specific technology requirements received these materials via post to ensure accuracy in printed measures.
After reporting penile measures, participants were randomly assigned to one of two conditions (standard-sized or fitted) and were mailed six standard-sized or six fitted condoms. Two weeks later, each received six alternate-type condoms. Participants reporting combinations not among those of the fitted condom received two standard-sized condoms. To mask condoms, stickers (red for standard-sized and blue for fitted) were affixed to the wrapper of each condom and only sticker colour was referenced in protocols and measures. Participants received guidelines for proper condom use in each mailing.
Upon receiving the condoms, men returned to the website daily for 30 days to describe their sexual behaviours and condom use. Incentives were valued at US$50–70. All study protocols were approved by the Institutional Review Board of Indiana University, Bloomington.
Study condoms
Both the standard-sized condom (VIVA) and fitted condom (TheyFit) were manufactured by Richter Rubber Technology in Kedah, Malaysia. The lubricants of each were virtually identical. The VIVA condom dimensions were within the range established by the International Standards Organisation (ISO) and were therefore consistent with condoms considered “standard-sized.”
The TheyFit condom was developed by Oceans Seven International and received original clearance by the United States Food and Drug Administration in 2001. At the time of this study it was distributed by Condomania of Los Angeles and was available in 55 sizes, based on combinations of 14 lengths (range 77–242 mm) and 11 lay-flat widths (range 41–64 mm), with a silicone-based lubricant (range 323–458 mg). Table 1 provides specifications of the study condoms.
Measures
Penile dimensions
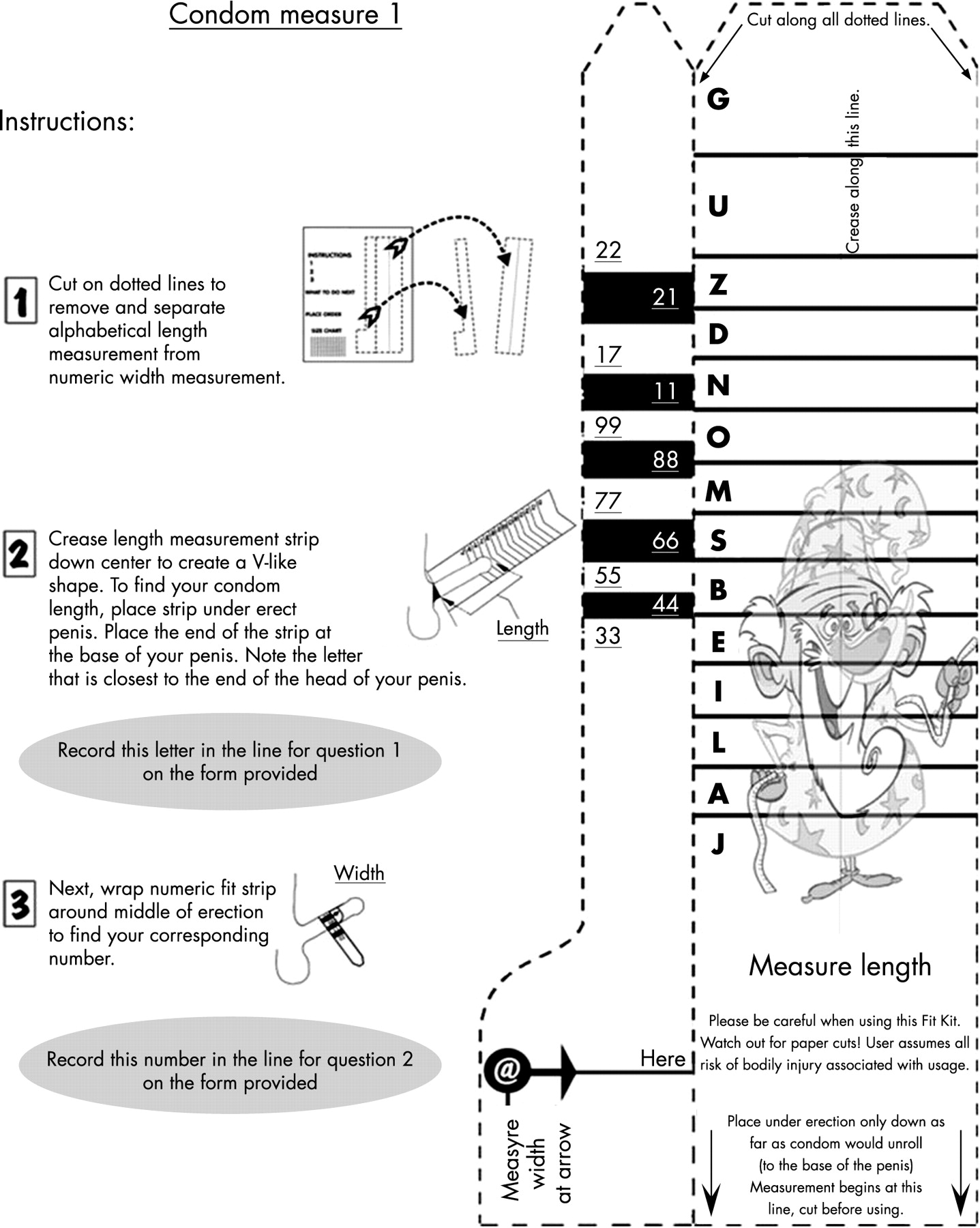
Men measured penile length (14 non-sequential letters) and circumference (11 non-sequential numbers) using a version of the FitKit (fig 1) that had all brand-identifying information removed. Men also provided measures from a device similar to the FitKit but with centimeter markers (length range 0–23 cm; circumference range 0–19 cm).
{kind=link}
Demographics
Measures included gender, age, ethnicity, sexual orientation, relationship status, and education.
Daily diary measures
For 30 days men completed event-specific diaries of daily sexual behaviours. Those using condoms for insertive anal or vaginal intercourse completed outcome measures for each condom used.
Condom failure
Condom failure calculations were based on established protocols.26 Rates included non-clinical breakage (during application), clinical breakage (during intercourse), total breakage (sum of non-clinical and clinical breakage), complete slippage (complete slippage from the penis), and total failure (sum of total breakage and complete slippage). Complete slippage was assessed through three separate measures (upon insertion, during intercourse, and upon withdrawal).
Condom acceptability and confidence
Two items assessed the acceptability of each condom used (willing to purchase, willing to recommend to a friend) and three items assessed confidence in the efficacy of each condom used (in disease prevention, pregnancy prevention, and ability to apply correctly). Response options for both constructs used a four-point Likert-type scale (very, somewhat, a little, not at all willing/confident).
Statistical analyses
For sample size, conservative estimates of condom failure based on established ranges and the maximum number of independent variables were considered. Estimates also accounted for non-independent data, the magnitude of correlation of breakage and slippage outcomes within a cluster (eg within a person), anticipated dropout given the study design, and established the type I error rate (α) at 0.05 and minimal power (1 – β) at 80%.27
To compare condom outcomes, levels of statistical significance were established using the SAS GENMOD procedure (SAS Institute, Cary, North Carolina, USA) using generalised estimating equations with the covariance structure assuming a constant correlation between observations within participant. The binomial distribution was used to model the binary breakage and slippage outcomes and the gamma distribution was used to model numerical acceptability and confidence outcomes in the presence of high skewness. After adjusting for order of condition assignment, effect size significance was assessed using the resulting two-sided chi-square test (α = 0.05). The null hypothesis underlied each analysis and all were performed using SAS version 9.1 (SAS Institute).
RESULTS
This paper reports data from 820 participants from all 50 states of the United States who used at least one of both condoms; the majority of these men represented the seven states prioritised during recruitment.
Participant characteristics
The majority of men were Caucasian (83.1%, n = 682), heterosexual (88%, n = 722), in a monogamous sexual relationship (77.8%, n = 638), and had completed some college (82%, n = 672). Ages ranged from 18 to 72 years (mean 27.36, SD 8.73).
Penile dimensions
Penile lengths ranged from 5.0 to 26.0 cm (mean 14.14, SD 2.63) and circumferences ranged from 3.0 to 19.0 cm (mean 12.22, SD 2.14).
Sexual and condom behaviours
Diaries included outcomes for 5287 condoms used during vaginal intercourse (48.8% (n = 2580) were standard-sized and 51.2% (n = 2707) were fitted). During anal intercourse, 770 condoms were used (49.6% (n = 382) were standard-sized and 50.4% (n = 388) were fitted). Some individuals used the same condom for both anal and vaginal intercourse during a sexual event.
Overall condom failure
Total failure rates were not significantly different between condom types when no consideration was given to penile dimensions; this was the case for vaginal and anal intercourse. For combined intercourse types, clinical breakage with fitted condoms (0.7%, n = 19) was approximately half that observed with standard-sized condoms (1.4%, n = 35). This was also reflected in the total breakage rate (0.7%, n = 20 for fitted; 1.6%, n = 38 for standard-sized).
Condom failure by intercourse type
No significant differences in condom breakage were detected between condoms used for vaginal intercourse. For anal intercourse, total breakage with fitted condoms was approximately one-fifth that of standard-sized condoms (p<0.01). Complete slippage of fitted condoms during anal insertion was significantly less (0.8%, n = 3) than for standard-sized condoms (1.1%, n = 4). These data are summarised in table 2.
Condom failure by penile dimensions
Based upon the relatively normal distribution of penile dimensions, three length groups and three circumference groups were constructed, with 25% being assigned to each of a smaller and larger group and 50% being assigned to a middle group. The “shorter” group contained men whose penile lengths ranged from 4.0 to 12.0 cm (mean 10.89 cm, SD 1.21), “middle” from 13.0 to 15.0 cm (mean 14.43 cm, SD 1.10), and “longer” from 16.0 to 26.0 cm (mean 18.11 cm, SD 1.59). With regard to penile circumference, the “smaller” group contained men whose penile circumferences ranged from 3.0 to 11.0 cm (mean 9.48 cm, SD 1.72), “middle” from 12.0 to 13.0 cm (mean 12.84 cm, SD 0.78), and “larger” from 14.0 to 19.0 cm (mean 15.57 cm, SD 0.82).
A detailed comparison of condom outcomes by participant length and circumference for vaginal intercourse are provided in table 3; data for anal intercourse are provided in table 4. Men with penile lengths of 16 cm or greater using fitted condoms had significantly less clinical and total breakage during both types of intercourse. This was also the case for men in the larger circumference category during vaginal intercourse and men in the middle circumference category during anal intercourse.
During both types of intercourse, slippage rates were similar between the two condoms for those with both shorter and longer lengths and those with smaller and larger circumferences. For those in the middle length and circumference categories, however, higher rates of slippage were observed with fitted condoms upon withdrawal after vaginal intercourse only. This influenced rates of total slippage, clinical failure, and total failure among these men for vaginal intercourse.
Condom confidence and acceptability
Men having anal intercourse expressed significantly higher levels of confidence in the efficacy of the fitted condom to protect them from disease (mean 3.44, SD 0.67) compared with the standard-sized condom (mean 3.36, SD 0.72). When compared by composite confidence scores, however, there were no significant differences in confidence for either intercourse type. With regard to acceptability for both types of intercourse, composite mean scores on the acceptability construct were significantly higher for the fitted condom (mean for anal 3.33, SD 0.78; mean for vaginal 3.15, SD 0.87) than the standard-sized condom (mean for anal 2.79, SD 1.05; mean for vaginal 2.91, SD 0.96). These findings are detailed in table 2.
Key messages
Some researchers and health practitioners have called for a broader range of condom sizes in order to reach men who are resistant to their use because of concerns of fit and feel
In this assessment of a condom sized to a man’s penile dimensions, significant reductions in condom breakage were observed when men wore the fitted condom, particularly men with longer penile lengths and during anal intercourse
Some men for whom a standard-sized condom should be of adequate fit experienced increased slippage with the fitted condom, highlighting the unique educational considerations that may need to be considered by STI prevention providers as the range of condoms evolves
Sized-to-fit condoms may support improved outcomes and less resistance to condoms by some men, but will also require unique and innovative methods to integrate them fully into STI prevention efforts
DISCUSSION
Rates of condom failure for both the fitted and standard-sized condoms were low and within previously established ranges. Breakage with the fitted condom was, however, significantly lower among men in the larger dimension categories for anal and vaginal intercourse and men in the middle circumference category during anal intercourse. These findings suggest that fitted condoms may be an important tool in STI prevention efforts.
Men in the middle dimension categories reported more slippage during vaginal withdrawal with the fitted condom. The unrolled latex typical of standard-sized condoms that would have been expected among men of this length may have facilitated better adherence to the penis, but this highlights the importance of withdrawal immediately after ejaculation as changes in penile rigidity may reduce the match between penile dimensions and the fitted condom. That increased slippage only occurred after vaginal intercourse also suggests the need to understand better whether withdrawal behaviours differ between vaginal and anal intercourse.
Although the need for accurate penile measures was stressed, it may be that those at the extreme ends of penile ranges were more careful in their measurement given that they could have experienced more challenges with actual condom fit in the past. The standard-sized condom should have reasonably fit men in the middle ranges, but it may be that some overstated their size in order to accommodate for past perceptions of condom discomfort (regardless of actual fit).
Most research on penile measurement and its reliability has used measures taken from the top of the penile shaft.6 The FitKit represents the transition of penile measures for research to those taken for other purposes. That the FitKit has to be printed on paper, and to ensure that men can see the length designation when looking downward on the penis, requires measures to be taken from the bottom of the penile shaft. More examination of the reliability of this device is necessary given that it was designed for non-research purposes, uses atypical methods, and that measures directly influence the selection of condoms.
It is also reasonable to consider whether a generalisable reliability of such a measure should be expected28 given that different physical and psychological states and other variables across sexual scenarios could influence penile length and circumference during both measurement and subsequent condom use.8 29–33 Future research with this tool should seek to engage men in studies that vary these internal and external variables in order to assess the expected variance in penile measures.
Although men held high confidence in the efficacy of both condoms, the fitted condom was rated more highly by men using it for anal intercourse. The fitted condom was also consistently rated as more acceptable than the standard-sized condom, although men with shorter penile lengths using the fitted condom for anal intercourse indicated more willingness to purchase it but less willingness to recommend it to friends, perhaps indicating that the marketing of fitted condoms will need to be sensitive to men’s concerns related to penis size.
Particularly given that some counselling-based interventions have demonstrated effectiveness at helping men reduce condom failures,18 practitioners may also find tools such as the Condom Fit and Feel Scale1 to be helpful in understanding men’s perceptions of condom comfort and helping them to select from those available in the marketplace. In addition, condom manufacturers and health practitioners should remain focused on understanding and responding to the other characteristics of condoms that some men and their partners consider undesirable and that support their resistance to using them, regardless of the extent to which concerns related to condom fit are addressed by more condom sizes.
The analyses presented in this paper only provide for an absolute comparison of condom outcomes and do not account for other important variables that have been associated with condom outcomes, such as the use of additional lubricants34 35 and error-making,36 37 among others. Although the daily diary method enabled more immediate reports of condom outcomes, and protocols stressed the importance of accuracy in penile measurement, all data were self-reported, which presented typical challenges to the validity of the findings. Finally, efforts to mask condom type may have been futile for those at the extreme ends of penile dimensions and their perceptions of the condoms may have been influenced by their detection of a difference in condom size.
Further research should assess the mechanisms through which a wider range of condom sizes would be made available. The Internet may present an acceptable forum given that one can access and complete the penile measures in the home, that it provides greater confidentiality and that it eliminates the need for the increased space allocation in stores; all important issues to be resolved by those who sell condoms in physical retail spaces. There will also be unique challenges for those making free condoms available through STI prevention campaigns (eg bowls of condoms in public sex venues and clinics). Integrating multiple sizes of condoms into these public health programmes will necessitate new and creative methods for distributing a measurement tool and sized condoms in a feasible manner.
Acknowledgments
The condoms used in this study were donated by their manufacturer, Richter Rubber Technology of Kedah, Malaysia. Condomania, of Los Angeles, California, USA, contributed other study materials and participant incentives.
REFERENCES
Footnotes
Competing interests: None declared.
Contributions: MR and DH designed the study, were responsible for the implementation of all study protocols, and led the writing of this paper. PM and MT conducted the statistical analyses presented in this paper and contributed to the writing of the paper. SAS served as a methodological consultant on the study and contributed to the writing of the paper. WLY provided conceptual contributions to the measures used in the study and contributed to the writing of the paper.