Article Text

Abstract
Introduction: Estonia is confronted by a dramatic expansion of the initially injection drug use-driven HIV epidemic. Little is known about HIV occurrence in population groups at high risk other than injection drug users.
Objective: To obtain data on the prevalence of HIV and hepatitis C virus (HCV) among female sex workers (FSW) in Tallinn.
Design: An unlinked, anonymous, cross-sectional survey of FSW recruited in Tallinn from October 2005 to May 2006.
Methods: 227 FSW were recruited for the survey and biological sample collection (HIV, HCV antibodies detection) using a combination of time-location, community and respondent-driven sampling.
Results: Among 227 women the HIV and HCV prevalences were 7.6% (95% CI 4.6% to 12.5%) and 7.9% (95% CI 4.5% to 12.6%), respectively. HIV prevalence was higher among FSW working in the street (odds ratio (OR) 6.4; 95% CI 1.1 to 35.6) and at the brothels and apartments supervised by the organised sex industry (OR 5.0; 95% CI 1.3 to 18.4). The duration of sex work was negatively associated with HIV prevalence (OR 0.78; 95% CI 0.63 to 0.97).
Conclusions: Prevention needs of FSW in this area include increasing rates of HIV testing and putting in place effective programmes that can help extend HIV prevention behaviours across a range of sexual and drug use risk behaviours.
Statistics from Altmetric.com
Estonia has experienced major political, economic and social changes associated with declines in health and life expectancy, growth in informal economies, including drugs and the sex trade following the collapse of the Soviet Union1 2 and is confronted by a dramatic expansion of the injection drug use-driven HIV epidemic.3–6 There is little or no evidence about HIV occurrence in other population groups at high risk. Sex work in its current forms and scale is a new phenomenon for post-Soviet societies. In Estonia, Tallinn is the capital city and the biggest harbour and is the centre of sex work in the country.7 This paper estimates the prevalence of HIV and hepatitis C virus (HCV) among female sex workers (FSW) in Tallinn, Estonia.
METHODS
We conducted an unlinked, anonymous, cross-sectional survey of FSW recruited in Tallinn from October 2005 to May 2006. All participants had exchanged sex for money, drugs or goods within the past 3 months. A multistage approach combining time-location, community and respondent-driven sampling8 9 was implemented. In stage 1, contacts (from brothels, apartments, saunas, massage parlours advertised in newspapers/erotic magazines/on the Internet) enlisted in a process of spatial mapping were invited to participate over the phone. Community recruitment was executed by field workers throughout FSW contacts known to them. Night club, bar and street-based FSW were approached directly during weekly field outreach visits. Index cases (N = 43) enrolled through stage 1 were used as “seeds” for subsequent respondent-driven sampling (a chain referral using a dual incentive system of a primary incentive for study participation and a secondary incentive for peer referral).8 9 Behavioural data were collected through a structured face-to-face interview10 administered by trained field workers (employees from the sex work counselling centre).
For anti-HIV antibodies testing venous blood was collected from the first 17 study participants and tested with HIV-1/HIV-2 III Plus from Abbott Laboratories (Abbott Park, Illinois, USA). The rest of the sample donated oral fluid samples obtained using the OraSure device (Epitope Inc, Oregon, USA) and was screened in duplicate for antibodies to HIV (anti-HIV) using Vironostica HIV Uni-Form II plus 0 (BioMerieux, Boxtel, The Netherlands).11 Specimens that were reactive on initial testing were subjected to confirmatory testing using Western blot assay (New LAV Blot I, Bio-Rad, Marnes la Coquette, France). For HCV antibodies specimens were tested by Ortho HCV version 3.0 (Ortho, Bucks, UK).
Statistical analysis
Proportions, means and medians were compared using Students’ t-test, the Kruskal–Wallis test, Pearson’s 2-test and the Mann–Whitney U-test when appropriate. Associations between antibodies to HIV (the outcome of interest) and covariables were explored univariably and by multiple logistic regression.
RESULTS
A total of 227 FSW were recruited; 43% of the sample was under 25 years of age (mean 29.5, SD 9.1). Two-thirds of participating women had completed secondary education (high school), 64% reported monthly income greater than the state average monthly wage (€670)12 and 68% had initiated sex work at or before the age of 20 years. The mean length of sex work was 8.3 years (median 6.2, range 0–30). The proportion of women with a short length of sex work career (<3 years) was highest (47%) in the (self-identified) category of “self-employed” sex work entrepreneurs (p = 0.01).
Within the past week a median of seven clients (mean 11; range 0–100) were served. Overall, 84% (191/227) had vaginal contacts with their clients, 41% (92/227) reported anal contacts. Always using condoms for anal, oral and vaginal sex was reported by 46%, for anal and vaginal sex by 75% of the respondents. Compared with HIV-negative women HIV-infected women were significantly more likely to report consistent condom use (vaginal, anal, oral intercourse combined; 87% versus 42%, p = 0.003). Twelve per cent of women reported having unprotected intercourse on request of a client within the preceding 7-day period. Current (within past 4 weeks) non-injection drug use was admitted by 23% and injection drug use by 6.6% (N = 15) of respondents. HIV-positive status was associated with injecting drugs (23.1% versus 6.7%, p<0.05).
One-third (34.5%) of respondents reported never being tested for HIV. Of those ever tested for HIV, 94.0% (140/149) reported being HIV negative, 2.7% (4/149) having received an HIV-positive test result and the rest did not disclose the result they received.
HIV prevalence was 7.6% (16/206; 95% CI 4.6% to 12.5%) and HCV prevalence was 7.9% (15/191; 95% CI 4.5% to 12.6%). The prevalence of HIV/HCV co-infection was 2.7% (95% CI 0.9% to 6.1%; five cases). Of those HIV infected, 18.6% (3/16) were aware of their serostatus. One women reporting knowing being HIV positive in fact tested negative on this occasion.
In the multivariate analysis after adjusting for age, injecting drugs and self-identified sex work category, HIV prevalence remained significantly higher among women working in the street (odds ratio (OR) 6.4; 95% CI 1.1 to 35.6) and at the brothels and apartments supervised by the organised sex industry (OR 5.0; 95% CI 1.3 to 18.4) compared with the rest of the women (sex work entrepreneurs “self-employed”, soliciting sex at alcohol vending venues or hotels, other). The duration of sex work remained negatively associated with HIV prevalence (OR 0.78; 95% CI 0.63 to 0.97). Women aged over 30 years were more likely to be HIV negative compared with younger women (OR 0.87; 95% CI 0.78 to 0.98). HIV-infected women were significantly more likely to use condoms consistently (OR 7.5; 95% CI 1.4 to 39.5) and to have larger FSW networks (OR 3.6; 95% CI 1.08 to 13.0; fig 1).
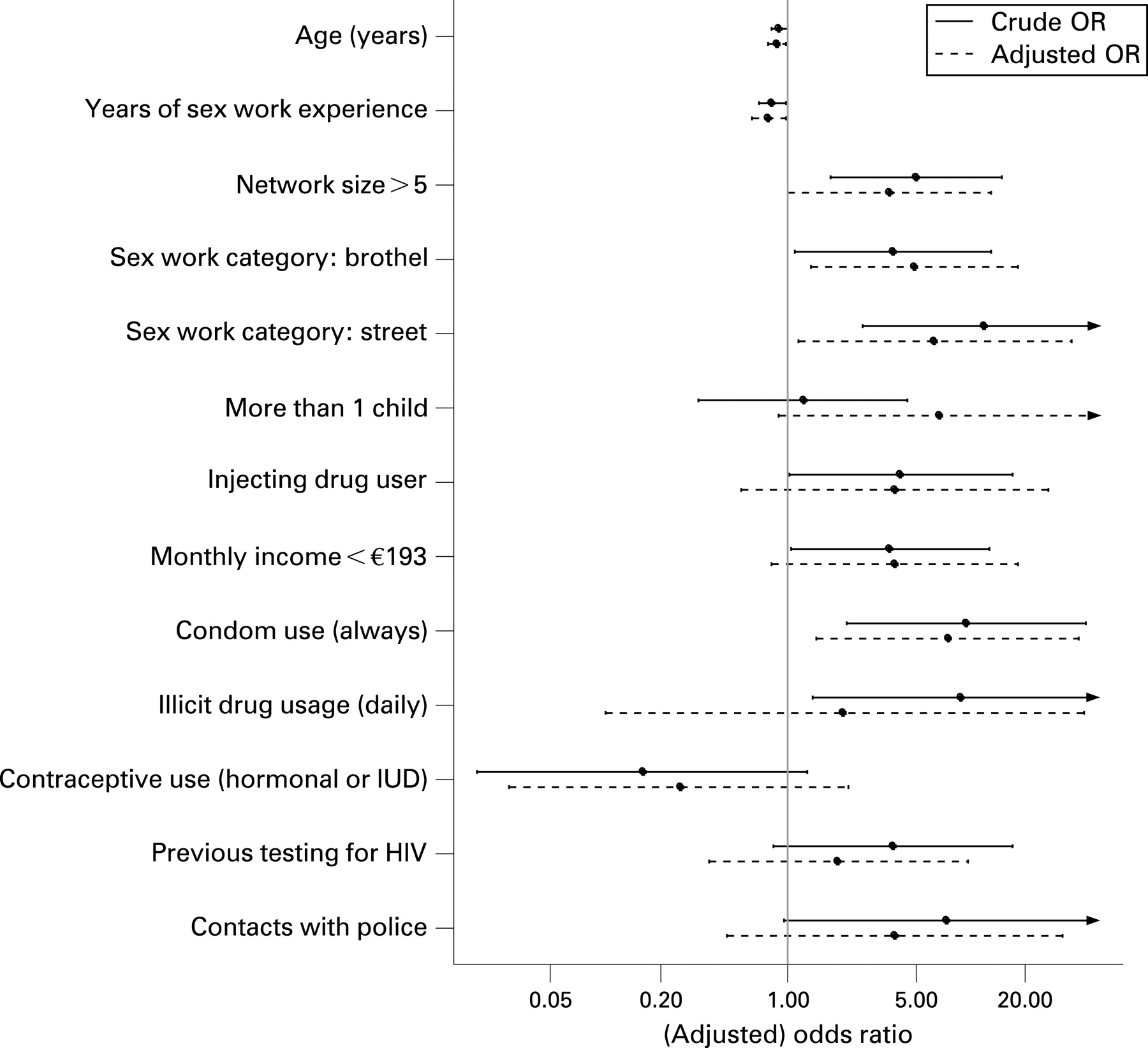
{kind=link}
DISCUSSION
This is the first study reporting a high prevalence of HIV infection among FSW from an eastern European country. Previous studies from the region have reported no HIV infection among FSW.13 14 More recently, an HIV prevalence of 3.8% was detected among street prostitutes while visiting a Lithuanian Social Ailments Consultation centre (a majority of these women were also reportedly injection drug users).15 Shakarishvili et al10 reported a 4% HIV prevalence among women at the remand centre in Moscow, 79% of the women were sex workers.
In our sample relatively few of the women were HCV/HIV co-infected. As a result of the much higher transmissibility of HCV in injection drug users compared with HIV16 17 a higher ratio would have been expected if most HIV cases were injection drug use acquired. Therefore we argue that within this group of women the sexual transmission of HIV is occurring.
We observed an inverse relationship between HIV status and the duration of sex work and age of the respondents. Women with shorter sex work careers were more likely to be HIV positive (irrespective of the actual age of the women). No differences in condom use or the number of clients were present (data not shown). Additional research is needed to delineate the risk (situational, behavioural) for contracting HIV among recent initiates to sex work.
A high proportion of HIV-infected sex workers were unaware of their HIV-positive status and over half of the women had never been tested for HIV. Intervention efforts are needed to increase rates of HIV testing and to promote HIV prevention behaviours.
Acknowledgments
The authors would like to thank Aire Trummal from the National Institute for Health Development in Estonia for helpful comments in the revision of the manuscript.
REFERENCES
Footnotes
Funding: The Global Fund to Fight AIDS, Tuberculosis and Malaria funded this study through the National Institute for Health Development in Estonia. Funding was also received from the Fogarty International Center, National Institutes of Health, USA (R01 TW006990).
Competing interests: None.
Ethics approval: Ethical approval was obtained from the National Institute for Health Development, Medical Research Ethics Committee IRB, Tallinn, Estonia.
Linked Articles
- Brief encounters