Article Text

Abstract
Objectives: A high proportion of individuals infected with HIV are unaware of the infection. They miss the opportunity for timely treatment. Our sexually transmitted infection (STI) clinic (South Limburg, The Netherlands) recognised the need to increase test rates and from 2004 routinely includes a HIV test, unless the client refuses, in each consultation. We evaluated the effectiveness of this opting-out approach for HIV testing.
Methods: We used anonymised data from our STI clinic from 2003–2007 to assess trends in HIV testing and (reasons for) test refusal using multivariate analyses and interview. Laboratory registry data from the area that is served by the clinic were evaluated as well.
Results: In South Limburg the number of HIV tests increased, which was mostly due to increasing STI clinic requests and antenatal screening. Of STI clinic attendees, 84% (1616/1920) were tested in 2003 and this proportion increased to 96% (3699/3836) in 2007. However, 88% (n = 57/65) of men who have sex with men and 44% (191/424) of heterosexuals who refused HIV testing after 2004 were linked to higher STI/HIV risk. Our clinic now uses these findings to develop more effective and tailored HIV/STI counselling in order to further optimise HIV testing practice.
Conclusions: Standard testing on HIV in a STI clinic is feasible and effective in increasing awareness of one’s HIV status. It should be an essential part of STI screening in STI clinics and should be considered in other healthcare settings for specific risk groups.
Statistics from Altmetric.com
Worldwide, large numbers of HIV positive individuals do not know they are infected.1 2 They miss the opportunity for timely treatment and play an important role in the spread of HIV in the population.3
Various healthcare settings worldwide currently undertake efforts to reduce the number of people who are unaware of their HIV infection by implementing standard HIV testing according to the opting-out strategy (standard testing unless a person refuses). For the developing countries, the opting-out strategy has been advised by UNAIDS/WHO.4 In 2006, the Centers for Disease Control and Prevention (CDC) recommended opting-out for HIV testing in all healthcare settings in the USA for people 13–64 years old.5 Also, in Europe, there were several initiatives to include routine HIV testing in different healthcare settings. Compared with other industrialised countries, the proportion of adults ever tested for HIV is generally low in the Netherlands. For example, according to a national sexually transmitted infection (STI) clinic registry (registering 68 977 consultations) in 2006, 57% of attendees had no prior HIV test.6 It is estimated that 80% of heterosexuals who are HIV positive and 40–60% of men who have sex with men (MSM) who are HIV positive do not know they are infected; thus, at least 7400 people nationwide are unaware they are HIV positive.7–11 Our STI clinic recognised the need to increase test rates and was the first STI clinic setting nationally to integrate standard HIV testing in all STI consultations unless the client refused as of 2004. In the Netherlands, opting-out has also been added to the screening of pregnant women since 2004 and in this setting it has been shown to be successful by yielding a very low refusal rate (2%) and those refusing were not being linked to high HIV risk.12
The aim of the current study is to assess effectiveness of and barriers associated with the implementation of this new HIV test policy in an STI clinic using STI clinic and laboratory registry data from 2003–2007.
MATERIALS AND METHODS
STI clinic procedures and study population
The outpatient STI clinic of the Public Health Service of South Limburg offers free-of-charge examination and treatment for STIs and saw approximately 5000 consultations in 2008. The clinic is spread over the region of South Limburg (population of 0.63 million) with three fixed locations for visit. All attendees are routinely screened for Chlamydia trachomatis, Neisseria gonorrhoeae, Treponema pallidum (syphilis) and hepatitis B at every new consultation. Before 2004, HIV tests were offered actively to the clients. Since 2004, HIV testing follows the opting-out strategy. Laboratory testing includes HIV antibody testing (Axsym, Abbott Laboratories, North Chicago, Illinois; Abbott Determine HIV 1/2) and reactive samples are confirmed by Western Blot (HIVblot 2.2, Genelabs Diagnostics, Sciencepark, Singapore). All STI diagnoses and other patient information are recorded in an electronic patient database.
For the current study, data from all clients in the period 2003–2007 were used with the exception of those who were known to be HIV positive.
Laboratory surveillance
For this study, we also obtained data from the three laboratories that serve the coverage area of the South Limburg STI clinic over the period 2003–2007. In these laboratories almost all HIV tests in South Limburg are registered.
Statistical analyses
In all analyses, tests from people known to be HIV positive were excluded. We analysed time trends in percentage of test refusals at the STI clinic and relative share of STI clinic and other healthcare providers in all test requests in the region univariately using logistic regression. To assess the characteristics of those who refuse testing, we analysed determinants associated with HIV test refusal (that is, sex, age, nationality, drug use, commercial sex work, current STI diagnosis, history of STI, history of (negative) HIV test, sex abroad, reason for STI clinic visit). Therefore, we performed univariate and multivariate logistic regression analysis with backward selection. Analyses were run separately for heterosexuals and MSM because we expect different determinants associated with HIV test refusal. For heterosexuals, we included an interaction term between the investigated determinants and sex. Determinants related to HIV test refusal were assessed for the period in which opting-out strategy was implemented (2004–2007). Finally, we assessed whether risk factors were different from those before the introduction of opting-out by examining interaction terms between independent risk factors and period (2003 vs 2004 through to 2007).
We considered a p value <0.05 as statistically significant or <0.10 in the case of interaction terms. Analyses were performed with SPSS version 14.0.2.
RESULTS
STI clinic
Population characteristics
In the period 2003–2007, 12 949 consultations were recorded. The number of consultations increased annually from 1920 in 2003 to 3836 in 2007 (fig 1). Overall, women comprised 52.9%, heterosexual men 38.4% and MSM 8.7% of consultations. Altogether, 34% of consultations were made by attendees aged 30 years or older and 11.7% by non-Dutch attendees—mostly (44%) of Belgian or German nationality since the STI clinic serves a European border region.

Absolute number of consultations (lines, right y-axis) and proportion of HIV tests refusals (bars, left y-axis) on the total number of consultations, excluding consultations by known HIV positive attendees of the STI clinic, South Limburg 2003–2007. MSM, men who have sex with men; STI, sexually transmitted infection.
Number of HIV tests and proportion tested
The absolute number (and proportion) of HIV tests increased strongly from 1616 (84.2%) to 3699 (96.4%) from 2003–2007 (p<0.001; fig 1). Increases were noted in all demographic groups—that is, by sexual orientation, nationality and age. Conversely, rates of test refusal declined over time reaching 2.6%, 3.0% and 2.1% in July to December 2007 for women, heterosexual men and MSM, respectively.
Before opting-out was implemented in 2003, test refusal rates were similar between heterosexuals and MSM. But during the implementation of opting-out, MSM refused significantly more often than heterosexuals (interaction term between sexual orientation and period of opting-out: p = 0.076). Notably, in 2007, no significant differences were detected anymore in refusal rates between heterosexuals and MSM.
Risk factors for not testing during opting-out
For heterosexuals, independent risk factors (table 1) to refuse HIV testing during opting-out were Dutch nationality (women only), lower number of sex partners, history of STI, previous negative HIV test, STI-related complaints and having had a partner who was diagnosed with a STI (“partner-warned”). Risk factors were no different from those in 2003 when standard HIV testing was not an integrated part of STI consultation.
For MSM, independent risk factors were having STI-related complaints, “partner-warned” and being older than 30 years of age. Notably, in 2003, older age was not a significant risk factor for HIV test refusal in MSM (interaction between opting-out period and age; p = 0.029).
The question is whether those who refuse HIV testing actually have a lower or higher risk of being unaware HIV positive. Some of our identified independent risk factors for not testing may imply a higher risk for being infected with HIV. These risk factors are being warned by a sex partner, having STI-related complaints, being older than 30 years of age (for MSM only11) and having a history of a STI (for heterosexuals only). At least one of these determinants was present in 87.7% (57/65) of MSM who refused HIV testing and in 44.1% (191/424) of heterosexuals who refused HIV testing. Overall, attendees who refused testing and had at least one of these aforementioned determinants comprised 2.2% of the total STI clinic population.
Reasons for not testing
Of a sample of the population (that is, those who visited the STI clinic since 2006) additional information on reasons for not having an HIV test could be retrieved. Reasons were registered by the STI clinic nurse who took the STI consultation and performed STI counselling. Such additional information was available for 82% of the people without a HIV test in 2006 and 2007. Major reasons (table 2) included fear, being in window phase and recently tested.
Laboratory surveillance
HIV tests according to healthcare provider
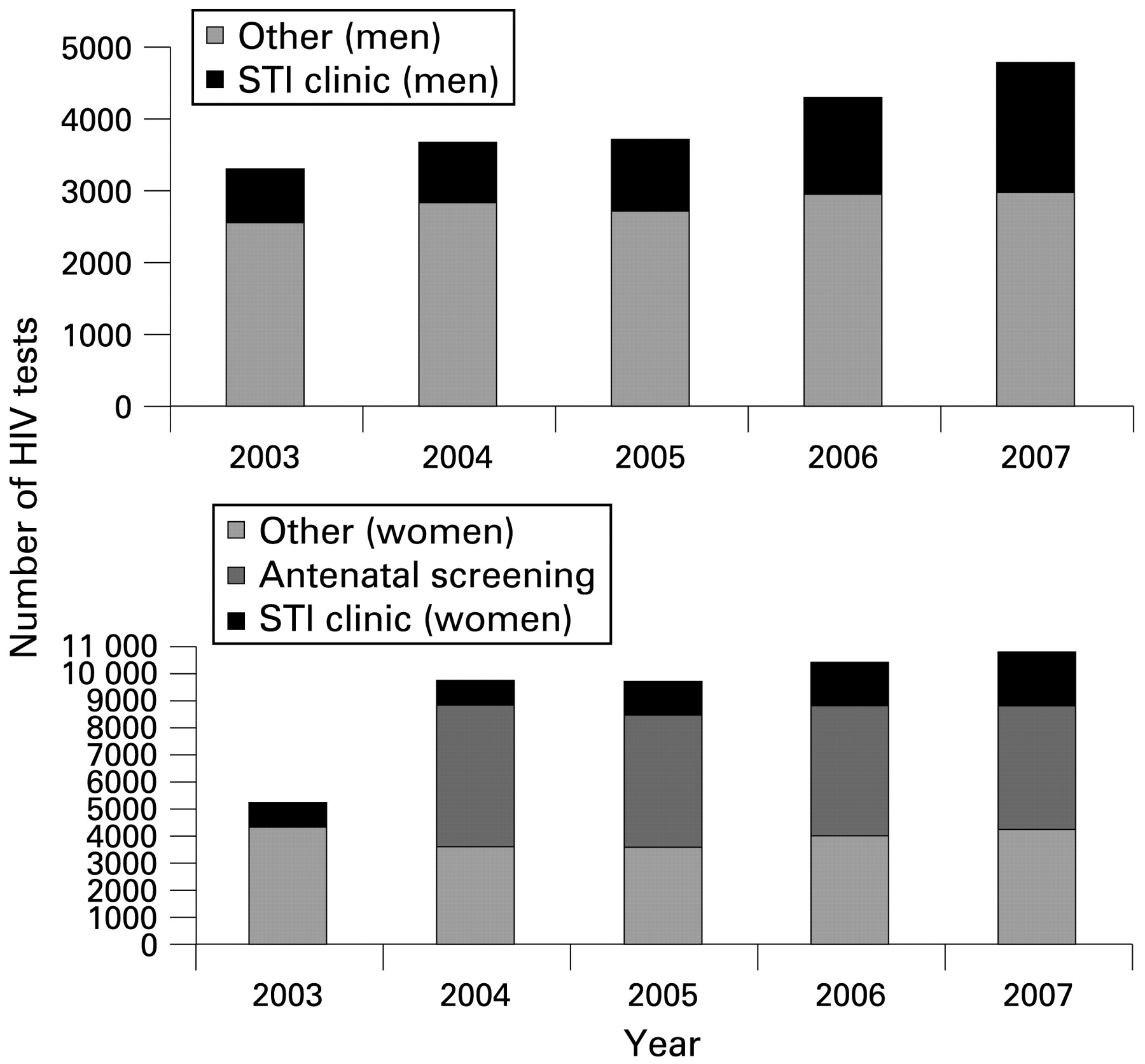
In the period 2003–2007, 65 801 HIV tests were performed in the region of South Limburg, excluding people who already had had a previous HIV positive test and children less than 16 years of age (fig 2). The number of HIV tests increased over time, which was mostly due to changed antenatal screening (HIV opting-out since 2004) and by increasing test requests by our STI clinic. In the period 2003–2004, 18.8%, 13.0%, 16.1%, 19.8% and 23.8% of all tests were requested annually by our STI clinic. This increase between 2004 and 2007 was noted for both men (23.1% to 37.2%) and women (9.3% to 17.9%). Taking into account the annual composition of the population in the region (source: Statistics Netherlands), and assuming that per annum a single test represented a single person, the overall incidence of HIV testing was 1.6, 3.0, 3.0, 3.2, and 3.3 tests per 100 adult women and 1.0, 1.2, 1.2, and 1.4 per 100 adult men for each sequential year in the period 2003–2007, respectively.
{kind=link}
{kind=link}
Number of HIV tests in South Limburg by healthcare provider (sexually transmitted infection (STI) clinic vs other requesters*) and by sex, laboratory registries, South Limburg, 2003–2007. *For women, number of women tested due to HIV opting-out in antenatal screening (implemented in 2004) is estimated by the proxy of 98% of number of alive-born children per year (since the refusal rate of HIV testing among pregnant women was 2%). Separate data from pregnant women who requested HIV testing (not opting-out) are unavailable in 2003.
HIV prevalence
Of all HIV tests in South Limburg in 2003–2007, 0.3% (n = 198) were registered as HIV positive. Of all HIV positive diagnoses, 22.7% originated from our STI clinic. At our clinic HIV prevalence was 0.4% (n = 45), which was higher for MSM (2.8%) than for heterosexuals (0.1%). No statistically significant time-trends in HIV prevalence were present.
DISCUSSION
Since the introduction of the opting-out strategy for HIV testing in 2004, we assessed a marked increase in the absolute and relative number of HIV tests at our STI clinic. This increase continued in following years and HIV test refusal rates are currently as low as 3%. Awareness of positive and negative HIV status has increased and more HIV infections were traced—that is, their number rose from around four to ten new infections annually since introduction of opting-out.
Routine HIV testing presents new challenges to healthcare providers and health systems. It needs to be linked to excellent referral systems and treatment services, since timely care is essential for best HIV treatment results.13–17 According to a Dutch HIV registry (data accessed April 2008, personal communication, A van Sighem, HIV Monitoring Foundation, The Netherlands), 45 new patients (65% MSM) entered HIV care in South Limburg in 2007. Three-quarters of new patients entered care shortly, within 1.5 month, after diagnosis. On entering the HIV treatment clinic, the median CD4 cell count was 396 (interquartile range: 250–671). The proportion of known HIV positive people on highly active antiretroviral treatment is relatively high with 80% being treated. Yet, there is much to be gained by effectively increasing referral and timely diagnosis because in our region 17% of people HIV positive have a long delay still—that is, more than 1.5 years—between diagnosis and entering HIV care and 18% of new HIV positive cases have low (<200) CD4 cell counts when treatment is shown to be less effective.8 16 17 Factors that currently hamper the optimal diagnosis, referral and treatment should be explored further and improvement of existing HIV testing practices in both STI clinics and other healthcare settings, such as general practices, is needed.
In our current systems of care, limited provider time and competing demands are well-recognised obstacles to the optimal delivery of a host of preventive services, including counselling, testing and referral.18 A health service location, such as a STI clinic, is an excellent setting for increasing timely diagnosis of HIV infection since HIV testing can easily be routine practice, optimal referral to healthcare delivery systems can be provided and a STI clinic is a natural setting for risk-reduction counselling. In the integrated STI/HIV counselling session provided during each consultation, the needs of individual patients can be addressed, such as those patients who might require more time to accept HIV testing or those patients who receive a negative HIV test result but require active intervention to facilitate changes in ongoing high-risk behaviour.19 Another advantage is that in a STI clinic setting a higher risk population can be targeted. With a share in HIV positive diagnoses of 23% and in the total number of annual HIV test requests of 18%, the role of the STI clinic in HIV testing practice in the region is substantial.
However, in spite of low and decreasing refusal rates, this current study shows that a substantial proportion of those who do refuse may be at higher risk for STIs including HIV. When assuming that those who report a history of STIs, current complaints, those being warned by a partner diagnosed with a STI and MSM who are older11 20 may be at higher risk for HIV, 44% of heterosexuals and 88% of MSM who refuse testing may be linked to a higher HIV risk.
Since this study was a retrospective exploratory study, we could not study in detail the underlying reasons of not testing. However, our data suggest that both client-related (that is, fear) as well as healthcare provider-related (mis)conceptions may be related to not testing. We registered short time between risk exposure and consultation, low number of sexual partners and having a recent HIV negative test elsewhere as reasons for not testing. These may well be (subjective) reasons of an individual healthcare provider not to test for HIV. The identification of such client and provider driven factors related to not testing should be the focus of local settings that incorporate routine HIV testing in order to optimise existing testing and counselling within their healthcare facility.
The finding that older MSM were more likely not to test than younger MSM corresponds with earlier observations and it is likely that these men are difficult to motivate having experienced the earlier years of the HIV epidemic and the earlier conservative HIV testing policy of test discouragement.20 Older MSM comprise a substantial part of STI clinic attendees, with 60% of MSM attendees being 30 years or older. It is very important to reach this group since it is shown that HIV incidence especially increases among these older MSM and highest HIV incidence rates are found among older MSM and MSM diagnosed with STIs.11 Still, we found that with opting-out, HIV test uptake increased in all demographic groups, including older MSM. Strategies to further improve test uptake in older MSM and other clinic attendees who may be linked to higher HIV/STI risk should be explored. Such strategies include tailored counselling (motivational interviewing), adequately coping with reactions of people who received unanticipated HIV diagnoses21 and creating awareness in health providers of the risks and consequences of not testing. Findings are now used to further optimise HIV testing practice in our clinic.
Results of this study showed that standard testing on HIV in a STI clinic is feasible and effective in increasing awareness of one’s HIV status. Implementation of opting-out in a STI clinic can lead to more traced HIV infections and more people receiving timely anti-HIV treatment. It should be an essential part of STI screening in STI clinics and should be considered in other healthcare settings for specific risk groups as well.
Key messages
-
Standard HIV testing in a sexually transmitted infection (STI) clinic is feasible and effective in increasing awareness of one’s HIV status.
-
The effectiveness of a HIV opting-out strategy can differ in various healthcare settings and should be locally evaluated for improving best practice.
-
Specific attention for people who refuse HIV tests in an opt-out setting is needed to identify those who are high risk and provide them with more tailored HIV testing and counselling.
Acknowledgments
The authors thank the Dutch AIDS Fund for sponsoring this study and the staff of our STI clinic. We thank the Medical Microbiology laboratories: Jos Bus (Atrium, Medical Centre, Heerlen), Peter Terporten, Inge van Loo (Maastricht University Medical Centre, Maastricht), Dick van Dam and Monique Manders (Maasland Hospital, Sittard-Geleen) for providing laboratory surveillance data, Ard van Sighem (Stichting HIV Monitoring, The Netherlands) for providing information on HIV registry data and Femke Koedijk for providing national and local STI clinic surveillance data.
REFERENCES
Footnotes
-
Funding: This study was sponsored by a grant from the Dutch AIDS Fund (grant number 2007083).
-
Competing interests: None.
-
Contributors: ND was the lead investigator, analysed the data and wrote the manuscript; AN interpreted the data and contributed to the final manuscript; MV contributed to data collection and the final manuscript; CH interpreted the data, contributed to the final manuscript and supervised STI clinic procedures.