Article Text

Abstract
Background: Published individual-based, dynamic sexual network modelling studies reach different conclusions about the population impact of screening for Chlamydia trachomatis. The objective of this study was to conduct a direct comparison of the effect of organised chlamydia screening in different models.
Methods: Three models simulating population-level sexual behaviour, chlamydia transmission, screening and partner notification were used. Parameters describing a hypothetical annual opportunistic screening program in 16–24 year olds were standardised, whereas other parameters from the three original studies were retained. Model predictions of the change in chlamydia prevalence were compared under a range of scenarios.
Results: Initial overall chlamydia prevalence rates were similar in women but not men and there were age and sex-specific differences between models. The number of screening tests carried out was comparable in all models but there were large differences in the predicted impact of screening. After 10 years of screening, the predicted reduction in chlamydia prevalence in women aged 16–44 years ranged from 4% to 85%. Screening men and women had a greater impact than screening women alone in all models. There were marked differences between models in assumptions about treatment seeking and sexual behaviour before the start of the screening intervention.
Conclusions: Future models of chlamydia transmission should be fitted to both incidence and prevalence data. This meta-modelling study provides essential information for explaining differences between published studies and increasing the utility of individual-based chlamydia transmission models for policy making.
Statistics from Altmetric.com
Screening is widely promoted as an effective and cost-effective intervention to control genital Chlamydia trachomatis infection amongst sexually active young adults and improve sexual health.1–3 Controlling C trachomatis is important because it is the most commonly reported sexually transmitted infection in many developed countries,4 it causes serious problems in women, men and newborns, and most infections are asymptomatic.5 The aim of screening is to detect and treat asymptomatic chlamydia in cases and their sexual partners to interrupt the spread of infection in the population and prevent the most common consequence: upper genital tract scarring that could lead to infertility and ectopic pregnancy. National chlamydia screening guidelines recommend annual testing,6 7 but the level and frequency of uptake required for a clinically relevant impact on transmission or complications have not been determined in any country.
Mathematical models can help understand the potential impact of chlamydia screening by showing how early detection and treatment affect transmission over time, when empirical data are lacking. Among the different types of transmission models, individual-based stochastic simulation models represent heterogeneity in transmission, screening and partner notification more realistically than population-based (compartmental) models. Results from apparently similar models, however, differ;8–12 the predicted reduction in prevalence with 10% annual uptake (50% after 10 years) in one model12 was greater than with 64% uptake in another (32% after 10 years).11 Differences between studies in the screening interventions investigated make it difficult to explain these findings. The objectives of this study were to compare the model structures and parameters describing transmission in three individual-based models of C trachomatis transmission, and to determine whether differences in model predictions could be explained by the specifications of the interventions.
METHODS
We compared three individual-based stochastic simulation models describing the transmission of C trachomatis in heterosexuals (meta-modelling) (table 1).10 13 14 All models described an age-structured population with a dynamic sexual partnership network.
All had a “susceptible-infected-susceptible” structure; individuals could be susceptible to chlamydia, or infected and infectious, with or without symptoms. Individuals with a cured or cleared infection were returned to the susceptible state without immunity. If individuals sought treatment or were screened, a proportion of their partners could be traced and treated through partner notification. Each model had parameters relating to the key components of infection dynamics: transmissibility; sexual contact rate and duration of infectiousness.19
The initial input values of key parameters (table 2) were based on estimates from the literature. Some of these parameters were then adjusted (model calibration) until, in combination, they generated baseline chlamydia prevalence rates and sexual behaviour patterns that corresponded with published data specific to each study. The original models and data sources are described briefly below. The names used here refer to the institution or project in which they were developed.
RIVM model, The Netherlands
This model was developed at the Dutch National Institute of Public Health and the Environment (RIVM are the initials in Dutch) to evaluate strategies for controlling chlamydia and gonorrhoea.14 Individuals in the model belong to one of two sexual activity groups; a small core group of younger adults who have more casual, including concurrent, partnerships, and the rest (table 1). C trachomatis transmission probabilities per sexual contact were estimated from published data about sexual partnerships with concordant chlamydia status20 and the number of contacts per partnership (all unprotected). The model was calibrated so that the baseline chlamydia prevalence fitted age and sex-specific rates from a study of opportunistic testing in general practices in Amsterdam21 and sexual behaviour data from a population-based survey.15
ClaSS model, UK
The Chlamydia Screening Studies (ClaSS) model was developed as part of the ClaSS project, to evaluate register-based screening using home-collected specimens in the UK.10 Input values for infection transmission and duration were similar to the RIVM model.8 There were three levels of sexual activity, labelled core (highest partner change rate), adjacent and periphery.22 The model was calibrated so that the baseline chlamydia prevalence fitted age and sex-specific rates and sexual behaviour data from a population-based survey conducted for the ClaSS project.10 23 Progression to reproductive tract sequelae was also included.
HPA model, UK
The Health Protection Agency London (HPA) model13 was developed to inform the National Chlamydia Screening Programme in England.12 24 25 It was based on a previous model for gonorrhoea transmission.26 Individuals had a preference for short or longer partnerships. In addition, a small core group (as in the RIVM model) could have concurrent partnerships. Transmissibility and the proportion of partners treated were determined by fitting the model to female chlamydia prevalence in studies conducted in general practice.18 The model was also calibrated to sexual behaviour reported by men in the second UK National Survey of Sexual Attitudes and Lifestyles (NATSAL, 2000).17 The proportion of women reporting previous treatment for chlamydia27 was used to calibrate the rate of treatment seeking at baseline.
Strategy for model comparison
We first determined whether or not differences in the published results could be explained by differences in assumptions about the content of screening interventions in each study. We then compared key parameter values, which was facilitated by the similarity in construction of the three models.
Standardised chlamydia screening programme
We standardised the components of a hypothetical intervention with the same parameters for the uptake and frequency of opportunistic screening and partner notification outcomes. We implemented this in each model, while keeping parameters describing transmission and duration of infection the same as in the published models. All sexually active 16–24-year-old adults were eligible to be screened once per year. The proportion screened was the product of three independent probabilities: attending a health service where screening was offered (70%); being offered a test (70%); and accepting (70%), consistent with the findings of a systematic review.28 These probabilities gave an overall uptake rate of approximately 35% every year in a random sample of the target population. For this study, it was assumed that 45% of current partners of cases detected in the programme received treatment and were cured in the RIVM and ClaSS models29 and 20% in the HPA model.12 We simulated the intervention 100 times in a hypothetical population of 40 000. We investigated the effects of screening women only and both women and men and examined the proportional reductions in prevalence from the baseline value after 10 years of screening.
Pre-intervention assumptions
Healthcare seeking behaviour before the introduction of a new screening intervention contributes to the baseline chlamydia prevalence. For this study it was assumed in the ClaSS and RIVM models that 45% of sexual partners of symptomatic individuals were notified and treated before the intervention was introduced.29 In the published RIVM model and in this study all symptomatic individuals (30% of women, 50% of men, table 2) sought treatment but there was no initial screening of asymptomatic individuals or partner notification.14 In the ClaSS model used for this study, there was no initial screening of asymptomatic individuals but all symptomatic cases sought treatment (30% of women, 75% of men). The HPA model retained the published assumptions of no screening of asymptomatic individuals but treatment of 20% of sexual partners of symptomatic individuals.
Comparisons of model parameters
We compared variables describing components of the basic reproduction number; contact rates, transmission probabilities per contact and the duration of infection,19 to determine how they affected the model predictions. We compared sexual partner formation and dissolution in each model and measures of the numbers of partners. We calculated both the mean annual and the effective contact rate (c), defined as c = m + v/m, where m is the mean number of sex partners per year and v its variance.19 This is a quantitative measure that can be compared between models to describe heterogeneity in numbers of partners that determines the transmission dynamics independent of the specific network structure.30 The effective contact rate is higher than the mean because it takes into account the skewed distribution in which a small part of the population has very high rates of sexual activity and plays a disproportionate role in transmission. We then compared model assumptions about the probability of C trachomatis transmission per sexual contact and the durations of infectiousness without intervention for symptomatic and asymptomatic men and women. We also compared the fractions of infected individuals seeking treatment before the intervention in the three models. Finally, we examined the turnover of new infections in each model by counting numbers of transmission events resulting from: new infection in a previously uninfected individual; new infection acquired in a new partnership; or re-infection within the same partnership.
RESULTS
Chlamydia prevalence before and after screening
At baseline, female chlamydia prevalence in 16–44 year olds was similar in all models (3.2% in the RIVM, 2.6% in the ClaSS and 2.8% in the HPA models) and fitted published age-specific rates in each model. Male baseline prevalence in 16–44 year olds was 2.9% in the RIVM, 3.1% in the ClaSS and 3.7% in the HPA models. There were differences between studies in male prevalence patterns, particularly under 30 years (fig 1). The highest rate was in 16–19 year olds in the HPA model, which was not fitted to empirical data. In the RIVM and ClaSS models, age-specific prevalence rates were similar to published data. The number of screening tests carried out was comparable in all models.

Chlamydia prevalence at steady state before the introduction of screening intervention, by age and sex. The Dutch National Institute of Public Health and the Environment (RIVM) and Chlamydia Screening Studies project (ClaSS) models were fitted to age and sex-specific chlamydia prevalence in women and men. The Health Protection Agency London (HPA) model was fitted to age-specific prevalence in women.
The predicted reductions in chlamydia prevalence after 10 years of the standardised intervention were similar to published results and showed the same pattern of differences between models (fig 2). The HPA model predicted that if only women were screened, prevalence would fall by 85% in women and men aged 16–44 years. The reductions predicted in women and men by the RIVM model were 25% and 26% and by the ClaSS model 5% and 4%, respectively. The same screening programme implemented in women and men resulted in greater relative reductions in prevalence in all models.

Predicted chlamydia prevalence in women 16–44 years before and after implementing a standardised screening programme. Shaded bars show overall chlamydia prevalence in women in each model. The predicted prevalence 10 years after introducing the screening intervention was examined for scenarios targeting women only (dotted) and women and men (hatched). ClaSS, Chlamydia Screening Studies project; HPA, Health Protection Agency London; RIVM, Dutch National Institute of Public Health and the Environment.
Sexual contact rates
There were large differences in sexual behaviour (fig 3), despite similarities in the processes of partnership formation and separation. The HPA model had the highest effective contact rates (more than eight) and mean numbers of partners per year (more than four per year) for both women and men aged 16–19 years. In the RIVM model effective contact rates were higher for women than for men in all age classes, with the highest rates observed for 20–24-year-old women. Effective contact rates were lowest in the ClaSS model and decreased with age in both women and men.

Effective contact rate and mean total numbers of sexual partners per year, by age and sex. Two measures of sexual behaviour were calculated for each model: closed shapes represent the mean number of sexual partners in the past year; open shapes represent the effective partner change rate. The dotted lines are present to show values from the same study in each age and sex category. ClaSS, Chlamydia Screening Studies project; HPA, Health Protection Agency London; RIVM, Dutch National Institute of Public Health and the Environment.
Transmission probability
The probability of chlamydia transmission in the HPA model was much lower than in the RIVM or ClaSS models (table 2). In the HPA model, the probability of transmission was one of the variables that was varied to fit the model to chlamydia prevalence. In the RIVM and ClaSS models these values were fixed based on literature estimates and were similar.
Duration of infection
Assumptions about the duration of symptomatic infection in women and men and the duration of asymptomatic infection in men were similar in all three models. The duration of asymptomatic infection in women in the RIVM model (370 days) was approximately twice that in the HPA and ClaSS models.
Pre-screening intervention treatment rates
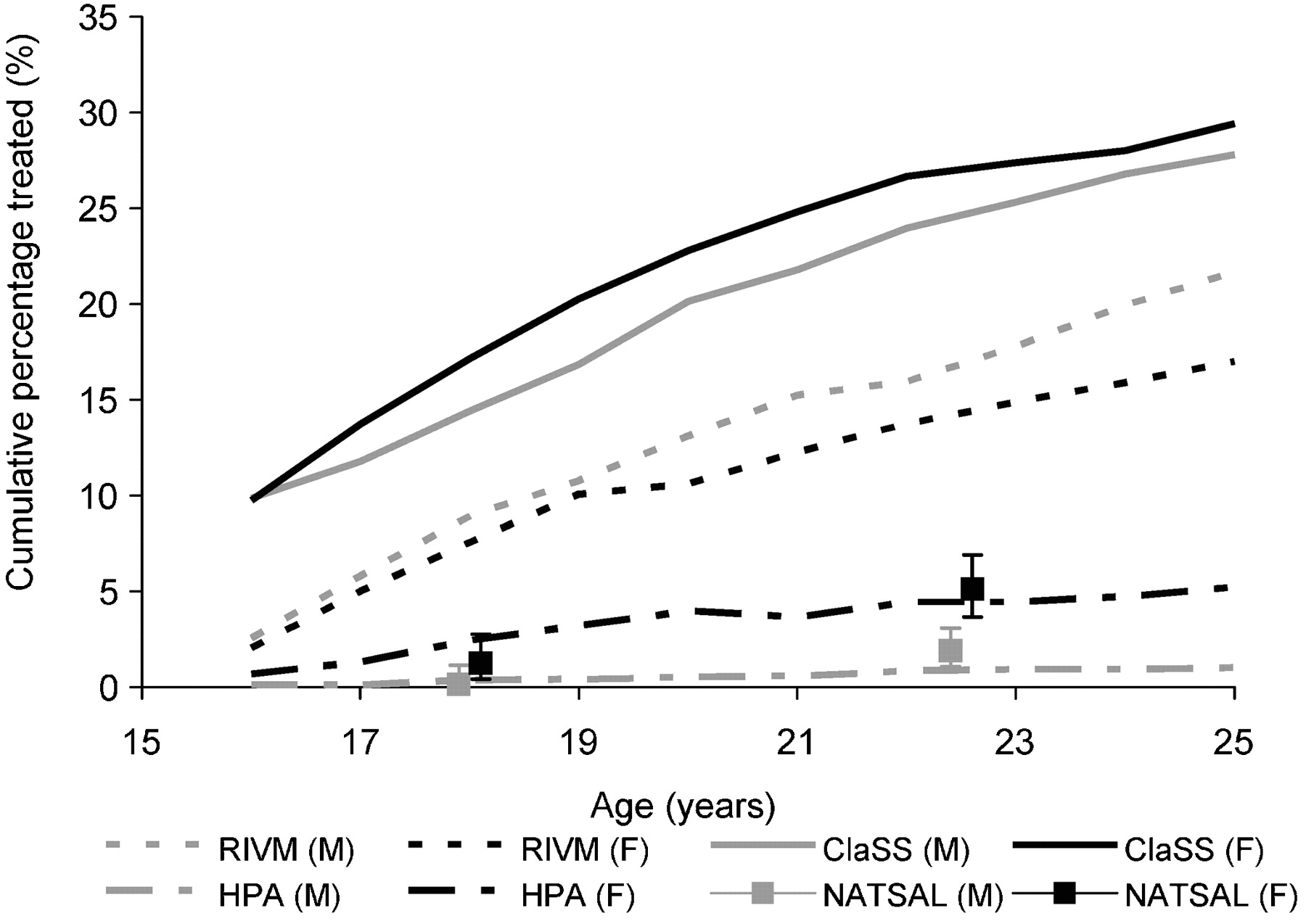
Differences in the assumptions about testing and treatment for chlamydia are described above. For model simulations using the standardised intervention, only symptomatic individuals were assumed to seek treatment spontaneously. The proportions assumed to be symptomatic were highest in the ClaSS and RIVM models, and these resulted in high proportions of the target populations having received treatment before the introduction of the screening programme (fig 4).

Percentage of population receiving treatment for chlamydia before the introduction of the standardised screening programme, by age. Lines represent predictions for women and men in each study. The squares with error bars show empirical population-based survey data about the proportions of 16–19 and 20–24 year olds reporting that they have been diagnosed with chlamydia in the UK National Survey of Sexual Activity and Lifestyle 2000 (NATSAL) study.17 ClaSS, Chlamydia Screening Studies project; HPA, Health Protection Agency London; RIVM, Dutch National Institute of Public Health and the Environment; F, female; M, male.
In the RIVM model a higher proportion of symptomatic men received treatment than women. In the HPA model, the proportions seeking treatment were much lower and were based on published data.27
Estimate of new transmission events
The numbers of transmission events resulting in the baseline chlamydia prevalence rates in each model differed markedly (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Turnover of infection in individual-based models of C trachomatis transmission, by age and sex. Transmission events include: new infections transmitted from an infected individual to a previously uninfected individual; infections transmitted from an infected individual to a previously infected but treated individual in a new partnership; re-infections in individuals because of failed partner notification; and re-infections transmitted within ongoing partnerships from an infected individual to a partner who has cleared infection spontaneously before receiving treatment. ClaSS, Chlamydia Screening Studies project; HPA, Health Protection Agency London; RIVM, Dutch National Institute of Public Health and the Environment.
The highest turnover of infections was in the ClaSS model. The RIVM model produced the lowest numbers of transmission events despite also assuming a high rate of pre-intervention treatment. The duration of infection in women was, however, the longest. In contrast to prevalence estimates, there were fewer transmission events in women than men in the RIVM model. In the HPA model the rate of new transmission events was intermediate.
DISCUSSION
We compared three models of the dynamics of sexually transmitted C trachomatis, all based on the same principles. All models resulted in comparable baseline levels of chlamydia infection in 16–44-year-old women, but not men. There were differences in the predicted chlamydia prevalence after implementing a hypothetical standardised screening programme. There were also differences in: C trachomatis transmission probabilities; sexual behaviour measures; proportions of symptomatic men and women treated for chlamydia before introducing screening and turnover of infections.
The main strength of this study was the direct comparison of three individual-based models under standardised conditions. This allowed us to explain some differences in model results, overcoming the difficulties of published data in which interventions and reported details about the models differ. Another advantage was that we examined and present the effects of the screening intervention in isolation from other model differences. We retained, as far as possible, original parameter values and prevalence data so that each model was calibrated and internally validated. This could be viewed as a limitation because we did not calibrate the models to the same observed data or investigate other screening options.31 This study therefore provides interim data. These are nevertheless essential to inform further ongoing analyses that will involve extensive re-calibration.
Key messages
-
Predictions from three individual-based models of chlamydia transmission would result in inconsistent policy recommendations about the likely effectiveness of a chlamydia screening programme.
-
This study suggests that models of C trachomatis transmission should be calibrated to empirical data on incidence as well as prevalence.
-
All model assumptions, including those for which no empirical data are available, should be made explicit and their consequences should be explored, if possible in a range of different models.
-
A meta-modelling approach provides essential information for explaining differences between published studies and increasing the utility of individual-based chlamydia transmission models for policy making.
Model comparisons are rarely reported32 but are recommended for understanding which model assumptions have the greatest effect on inferences, which should be modified, and for discovering flaws in model parameters or structure.33 Halloran and colleagues32 compared individual-based stochastic simulation models to examine the predicted effects of combining targeted and general interventions to contain a pandemic of H5N1 influenza. The models showed similar qualitative effects, particularly when the basic reproduction number was two or less, which is useful for pandemic planning. Our study found that a hypothetical chlamydia screening intervention reduced prevalence in all models, but that differences in the levels of effects could lead to different policy decisions. There might therefore be more agreement about the transmission dynamics and management of a new unknown influenza pandemic than about C trachomatis.
This study suggests that models of C trachomatis transmission should be calibrated to empirical data on incidence as well as prevalence. Models of chlamydia transmission tend to be fitted to cross-sectional data from a single time point. Our study shows that similar steady state chlamydia prevalence rates are reached with marked differences in the combinations of transmission probability, contact patterns and rates, treatment rates and duration of infection. Validation of transmission models for infections such as measles and influenza requires a demonstration that model data fit reports of new cases over time.31 This is not possible for chlamydia, because case reports reflect intensity of testing rather than incidence.34 High quality incidence data are, however, lacking. Most reports are from retrospective facility-based studies in the USA that overestimate incidence.35 One prospective study reported 4.9 (95% CI 2.7 to 8.8) incident cases per 100 person-years for women aged 16–24 years in UK general practices but loss to follow-up was high.36
Our study allowed us to compare how realistic were the assumptions of each model. The assumptions in the ClaSS and RIVM models, that all symptomatic cases would be treated and that a high proportion of men was symptomatic, were based on clinic-based studies using insensitive diagnostic tests and do not apply to the general population. These values resulted in an improbably high proportion of the model population having received treatment before the hypothetical intervention began and contributed to the lower impact of screening in these than in the HPA model. The UK NATSAL 2000 study used for the HPA model provides empirical evidence of lower values, with fewer than 5% of women and men ever reporting a diagnosis of chlamydia.27 Sexual activity levels were, on the other hand, highest in the HPA model. Summary values for 16–19 year olds were more than twice those in the ClaSS and RIVM models (fig 3). The mean annual numbers of partners in this model (approximately four in 16–19-year-old and two in 20–24-year-old women and men) were also higher than those reported in NATSAL 2000 (mean new partners 0.75 in women and 1.45 in men aged 16–24 years in the past year).17
The lowest predicted impact of organised chlamydia screening in the ClaSS model could partly be explained by higher pre-intervention treatment levels. The turnover of infection was, however, high, possibly resulting from re-infections within relationships as a result of a combination of the high frequency of sexual intercourse, high per-contact transmission probability, and long duration of casual partnerships despite lower levels of sexual partner change than in the other models. The large impact of screening in the HPA model probably resulted from low levels of pre-intervention treatment combined with high levels of transmission of asymptomatic infection with a short duration among teenagers, despite the low transmission probability. The per-contact transmissibility of C trachomatis has not been established with any certainty but the values used in all three models were within a plausible range estimated by Katz,37 depending on the number of sexual contacts. The effect of screening in the RIVM model was intermediate, possibly because of the moderate level of pre-screening treatment but a longer duration of infection leading to lower overall turnover. Future studies will elucidate these differences in greater detail.
Current individual-based models of chlamydia transmission would result in inconsistent policy recommendations, particularly in the UK.10 12 We could not say which, if any, of the model predictions was accurate because of uncertainty about a large number of key parameter values and the lack of data for external comparison. Parameter uncertainty is a problem for all mathematical models, but the number of parameters that has to be defined is greater in an individual-based than in a deterministic compartmental model.33 38 In general we suggest that: model predictions should be interpreted relative to the baseline situation that is modelled; all model assumptions, including those for which no empirical data are available, should be made explicit and their consequences should be explored; and if possible, a range of models should be used to explore and understand better the impact of specific model structure on transmission dynamics. For future research about chlamydia and its prevention, in addition to incidence studies, additional data for external validation should be obtained from trials randomly selecting distinct geographical areas to measure the relationship between screening uptake and change in population prevalence over time. More certainty about plausible transmission probabilities and the duration of infection are also required. In conclusion, this meta-modelling study provides essential information for explaining differences between published studies and increasing the utility of individual-based chlamydia transmission models for policy making.
REFERENCES
Footnotes
-
Funding: UK NHS Health Technology Assessment Programme project 97/32/31, Swiss National Science Foundation project 320030-118424.
-
Competing interests: None.