Article Text

Abstract
Objectives Commercial sex is licensed in Victoria, Australia such that sex workers are required to have regular tests for sexually transmitted infections (STIs). However, the incidence and prevalence of STIs in sex workers are very low, especially since there is almost universal condom use at work. We aimed to conduct a cost-effectiveness analysis of the financial cost of the testing policy versus the health benefits of averting the transmission of HIV, syphilis, chlamydia and gonorrhoea to clients.
Methods We developed a simple mathematical transmission model, informed by conservative parameter estimates from all available data, linked to a cost-effectiveness analysis.
Results We estimated that under current testing rates, it costs over $A90 000 in screening costs for every chlamydia infection averted (and $A600 000 in screening costs for each quality-adjusted life year (QALY) saved) and over $A4 000 000 for every HIV infection averted ($A10 000 000 in screening costs for each QALY saved). At an assumed willingness to pay of $A50 000 per QALY gained, HIV testing should not be conducted less than approximately every 40 weeks and chlamydia testing approximately once per year; in comparison, current requirements are testing every 12 weeks for HIV and every 4 weeks for chlamydia.
Conclusions Mandatory screening of female sex workers at current testing frequencies is not cost-effective for the prevention of disease in their male clients. The current testing rate required of sex workers in Victoria is excessive. Screening intervals for sex workers should be based on local STI epidemiology and not locked by legislation.
- Sex worker
- STI
- screening
- cost-effectiveness
Statistics from Altmetric.com
Introduction
Sex work in the state of Victoria, Australia, is decriminalised but regulated through a licensing system. Sex workers in Victoria are required to provide evidence of having regular sexual health check-ups for Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis, and to be examined for genital warts or active herpes lesions every month, plus serology for HIV and syphilis every 3 months.1 Sex workers may be prosecuted for knowingly having sex with clients while carrying a sexually transmissible infection (STI) or for not having the prescribed STI tests. The financial cost of consultations and testing for these STIs is usually covered by the government healthcare system. However, it is known that many sex workers have almost universal condom use at work and a low incidence of STIs.2 The few STIs that they do acquire are usually attributable to private sexual partners.2 Although it is a hallmark of public health campaigns to promote STI testing among groups with relatively large numbers of sexual partners, we postulated that the current testing rates required of sex workers in Victoria may be excessive. We conducted a simple analysis on the cost-effectiveness of these regulations and evaluated the cost-effectiveness of alternative testing frequencies. To assess the cost-effectiveness of regular STI testing, we used a mathematical model to estimate the expected number of STI transmissions from sex workers to their clients based on available behavioural, biological and epidemiological data. We used the model to explore how the expected number of sex worker-to-client transmissions of HIV, syphilis, chlamydia and gonorrhoea changes with the frequency of STI testing and the cost of that testing. We took a health-sector perspective with 3% discounting of costs and outcomes according to standard methods.3 We only included the costs and outcomes of diseases in male clients.
Methods
If a sex worker has an STI, then the expected number of transmissions of the infection to clients (per sex worker per week) can be estimated as the product of the number of clients each sex worker has per week, n, and the probability of transmission per sexual encounter with a client, β. The probability of transmission per encounter can be modelled by
That is, the modelled number of transmissions is a function of the average sexual activity level of sex workers (in terms of number of acts and condom use), the biological transmission efficiency of the organism in question (in terms of both incidence to sex workers and secondary transmissions from sex workers to clients) and the testing frequency.
The total number of infections caused by all infected sex workers per week (equation 1) can be expressed in terms of the total number of tests per week:
If each infection results in a loss of q quality-adjusted life years (QALYs) for the infected person, then the cost outlaid for each QALY saved is
We also used estimates of the cost to treat infections to calculate the expected total financial loss/saving (net monetary benefit) for the health system (total savings is calculated as the cost saved on treatment from averting infections minus the cost of screening, assuming a willingness to pay of $A50 000 per QALY gained). We also calculated the marginal cost-effectiveness ratio by dividing the net monetary benefit by the net health benefit (net QALYs gained was calculated by the product of the number of infections averted and the QALYs lost per infection).
Table 1 presents the values and costs for the parameters of this model based on behavioural, biological, epidemiological and screening cost data and literature associated with HIV,4–8 syphilis,9–18 chlamydia19–21 and gonorrhoea22–26 for Victoria, Australia. We estimate STI incidence in sex workers from sexual-health clinic databases and recently reported estimates of incidence in Victorian sex workers.2 However, we conservatively use the upper 95% confidence bound of incidence as the mean value in our model. Specifically, we take incidence to be 0.1/100 person-years for HIV, 0.1/100 person-years for syphilis, 3.3/100 person-years for chlamydia and 0.7/100 person-years for gonorrhoea. Notably, no confirmed cases of HIV transmission to or from a sex worker in Australia have ever been reported. We take the efficacy of condoms to be 95%27–31 and assume that they break or slip 2.5% of the time,32 even though an Australian prospective study suggested that 0.6% may be a more accurate measure for sex workers.33 We also conservatively assume that a broken or slipped condom equated to unprotected sex. The actual number of sex workers in Victoria is not precisely known, but we base our analysis on an estimated 2000 sex workers. This estimate is derived from studies showing that the proportion of men that access sex workers in Victoria is similar to that in the State of New South Wales2 34 35 and an estimation of the size of the sex industry in New South Wales.36 This is also in agreement with estimates based on the number of registered brothels and average number of women working from each brothel and consistent with expert opinion (CK Fairley, MY Chen, personal communication, 2009).
Definitions and values of parameters used in our analysis
Screening costs
We used costs reported under the Australian Medicare health system for consultation and STI testing (October 2008). Costs for each clinical consultation for a sexual health check-up are $A32.80 (assuming level B on the Medicare scheme). In addition, it costs $A24.55 to conduct a chlamydia and/or gonorrhoea PCR assay (item 69316). If both HIV and syphilis testing are carried out together (item 69387), then the extra testing cost is $A25.30, but if the tests are carried out on separate occasions, then the syphilis testing cost (item 69384) is $A13.40, and the HIV ab/ag testing cost (item 69384) is $A13.40. For consultations in which multiple STIs are screened, we apportioned the consultation costs equally across each STI.
Treatment costs
If a screening test detects an infection, then we consider the treatment costs for chlamydia and gonorrhoea as the cost of one consultation for screening tests (MBS item 23) plus the cost of the relevant medication required to clear the infection (using costs under the Pharmaceutical Benefits Scheme). Similarly for syphilis, the treatment cost is composed of three consultations, one for providing medication and two follow-up serological tests.
Costs of disease in male clients
Costs associated with each infection in male clients were estimated. There are no recent estimates of the costs of people living with HIV or experiencing complications related to chlamydia, gonorrhoea and syphilis in Australia. Therefore, we used the lifetime costs of HIV infection in 2004 derived from data in the USA,37 inflated to 2007 prices with the medical component of the US Consumer Price Index38 and converted to Australian dollars using the Purchasing Power Parity39; this estimate was $A490 370 discounted at 3%. We used an expected value analysis of the complications of chlamydia and gonorrhoea to estimate the costs of infection (appendix 1). Data from Australia and expert opinion on the frequency and treatment of disease (and complications including arthritis, epididymitis and infertility) are used to estimate a cost per chlamydia infection of $A57 and cost per gonorrhoea infection of $A82. We did not calculate the cost associated with complications of syphilis infection because of a lack of data and uncertainty.
Utility of disease
We estimated a loss of 7.5 QALYs from the time of HIV infection, discounted at 3%, as used in a recent systematic review of economic evaluations of HIV interventions.40 For the utility loss associated with complications of chlamydia and gonorrhoea in men, we used the expected value analysis discussed above to calculate a utility loss of 0.0085 per infection over 12 months, undiscounted. We did not calculate a utility loss for syphilis.
Results
The implementation of current STI screening guidelines for 2000 female sex workers in Victoria costs over $A3 750 000 per year at the current screening frequency of every 12 weeks for HIV and syphilis and every 4 weeks for chlamydia and gonorrhoea. The cost of screening for chlamydia and gonorrhoea is $A1 490 000; the cost of screening for HIV is $A400 400 (figure 1).

Relationship between the annual cost of screening sex workers for STIs (solid curves) and the modelled expected number of STI transmissions from sex workers to clients (dashed curves) versus the duration of time between testing for (A) HIV, (B) syphilis, (C) chlamydia and (D) gonorrhoea. The grey lines and numbers indicate the screening cost and expected number of transmissions under the current testing frequency of once every 12 weeks for HIV and syphilis, and once every 4 weeks for chlamydia and gonorrhoea. The expected number of transmissions is shown on a log10 scale.
The expected number of STI transmissions from sex workers to male clients per year is low, with fewer than 0.1 HIV cases, ∼3.6 syphilis cases, ∼16.4 chlamydia cases and ∼2.8 gonorrhoea cases (figure 1), even if the STI incidence rate to sex workers is conservatively high. This is because the population prevalence (and incidence) of STIs in sex workers is low, and condom usage rates are very high.
If testing frequency was increased, then screening costs would increase sharply. However, not surprisingly, if the testing frequency was decreased, then screening costs would decrease, but the number of infections to clients would increase (figure 1). Even if testing frequency was decreased to just once per year, if the incidence rate to sex workers remained unchanged then less than 1 HIV transmission, ∼16 syphilis transmissions, ∼36 gonorrhoea transmissions and ∼210 chlamydia transmissions could be expected to male clients.
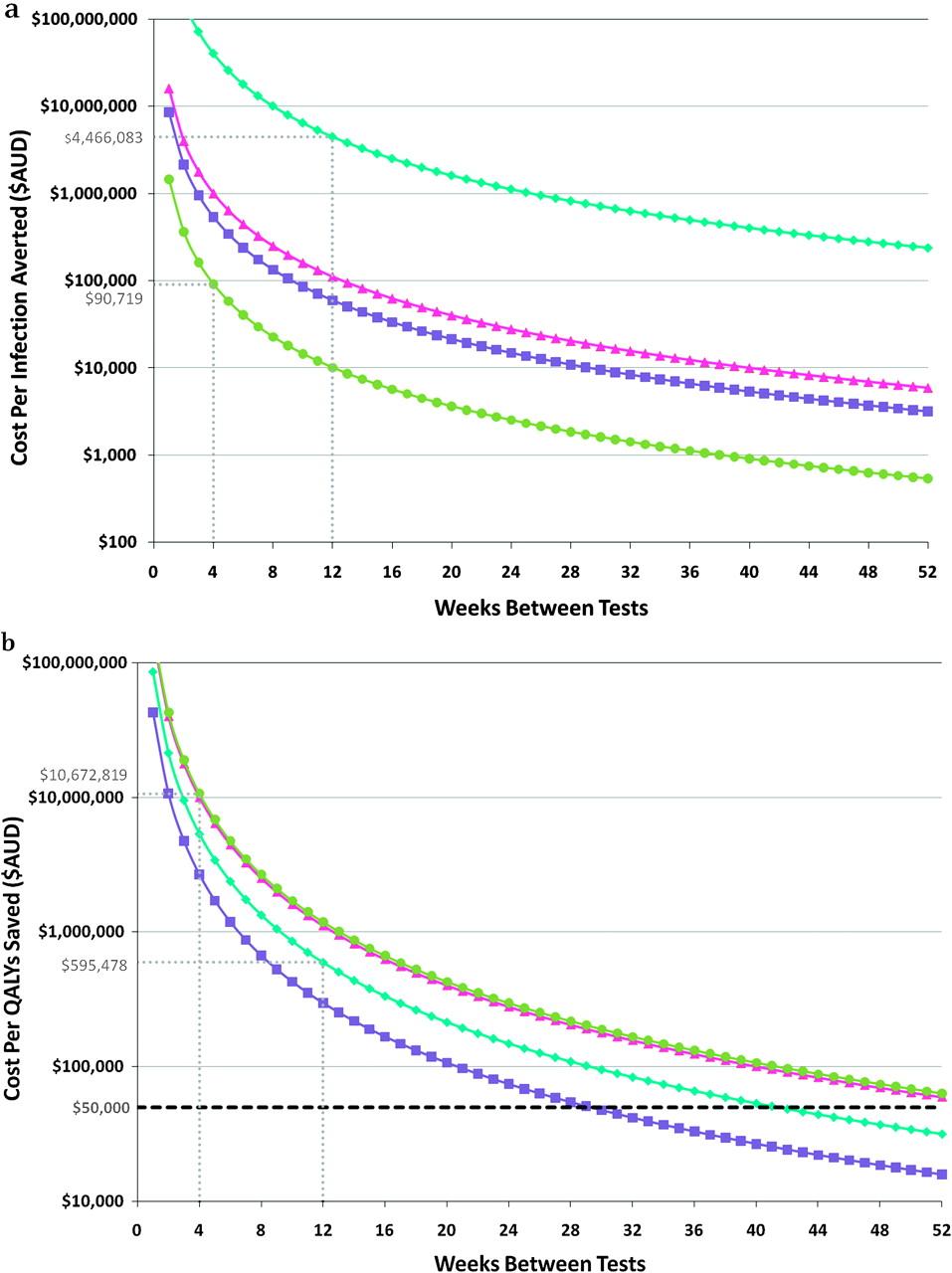
To ascertain the degree to which investment in frequent testing can be attributed to the low incidence, we calculated the cost outlaid (for screening) per infection averted in clients. Figure 2A presents the modelled relationship between the screening costs per infection averted and the number of weeks between tests for HIV, syphilis, chlamydia and gonorrhoea. Under current testing rates, for example, it costs over $A90 000 in screening costs for every chlamydia infection averted and over $A4 000 000 for every HIV infection averted (figure 2A). To assess the value of this testing schedule, we extended this relationship to estimate the cost per QALY saved (figure 2B). We calculated that under current testing rates, it costs almost $A600 000 in screening costs for each QALY saved due to the burden of chlamydia infections, and it costs over $A10 000 000 in screening costs for each QALY saved from HIV infection.

Modelled relationship between the (A) cost per infection averted and testing frequency; (B) cost per QALY saved and testing frequency, for HIV (blue diamonds), syphilis (pink triangles), chlamydia (green circles) and gonorrhoea (purple squares).
We determined the incidence levels that would be required in order for the current testing rates to become cost-effective. We found that current frequencies of STI testing would be cost-effective only if incidence increases substantially (table 2). Incidence would need to increase by 12-fold for HIV, 67-fold for syphilis, 213-fold for chlamydia and 53-fold for gonorrhoea from the conservatively high incidence already assumed.
Comparison between current conditions and increased risk scenarios in order to satisfy cost-effectiveness of no more than $50 000 per QALY saved
We then determined the frequency of testing that would be cost-effective (cost per QALY saved less than $50 000) under conservative assumptions about the present and if condom use declines and/or STI incidence increases. Table 2 shows the minimum time between tests that is cost-effective under current conditions and for the scenarios of condom use decreasing from 99% to 90% and/or incidence increases by threefold. Even under the extreme (and unrealistic) scenario of a substantial change in both condom use and incidence, the minimum time between tests that is cost-effective is over 16 weeks for HIV, approximately 24 weeks for syphilis and chlamydia, and almost 12 weeks for gonorrhoea. This is still markedly longer than current practice.
We also estimated the marginal (incremental) cost-effectiveness ratio of each screening frequency. Screening at the current recommended frequency costs over $A500 000 per QALY saved for HIV, and over $A10 million per QALY saved for Chlamydia (figure 3A). The Net Monetary Benefit (NMB) of screening at current frequencies is calculated using an assumed willingness to pay of $A50 000 per QALY gained.41 The NMB was a loss of $A356 000 per year for HIV and a loss of almost $A1.5 million for chlamydia (figure 3B); that is, none are cost-effective at current screening frequencies. Based on our model analysis, HIV testing should not be conducted less than approximately every 40 weeks for the cost per QALY saved to be less than $50 000, and the frequency of chlamydia testing should not be less than approximately once per year. Indeed, just in terms of financial aspects, screening costs are almost $A1 500 000 more expensive than the treatment costs saved by preventing chlamydia infections, and screening costs are over $A350 000 more expensive than the treatment costs saved by preventing HIV infections (figure 3). In order to break even financially, such that the cost of screening is not less than the costs saved on treatment (when the curves on figure 3 cross zero), based on our model we calculated that testing should not be less than every 36 weeks for HIV, 295 weeks for syphilis, 160 weeks for chlamydia and 446 weeks for gonorrhoea. These estimates are independent of the number of sex workers. Thus, if the incidence of STIs in sex workers remains low, there is a strong argument for relaxing regulations to less frequent testing, if not abandoning mandatory testing entirely. Notably, among representative population-based samples of female sex workers, more of the women in the voluntary testing environment in Sydney (53%) attended public sexual-health clinics than in the mandatory testing environment in Melbourne (29%, p<0.001)).42

Modelled relationship for HIV (blue-diamonds), syphilis (pink-triangles), chlamydia (green-circles) and gonorrhoea (purple-squares) of (A) the marginal cost-effectiveness ratio, and (B) the net monetary benefit (costs saved on treatment minus costs spent on screening) versus the testing frequency; note that the total savings curve appears the same for chlamydia and gonorrhoea.
Conclusions
Some previous studies have attempted to estimate the costs averted by STI-prevention programmes in various settings.2 43 44 Our study used a novel mathematical transmission model and conservative parameters, linked to a cost-effectiveness analysis, to examine current testing rates among commercial sex workers in Victoria. We show, for the first time, that the current testing rates are not cost-effective. Mandatory screening of sex workers as legislated in Victoria is not cost-effective for the prevention of disease in their male clients at current test frequencies. If screening occurs much less frequently, it may be cost-effective, although the benefit is still very limited. Expenditure on screening at the current frequency could be spent on more effective and cost-effective prevention programmes to produce more benefit for individuals and the health sector. Female sex workers have one of the lowest prevalences of HIV (and other STIs) in Australia, compared with levels in other groups of the general sexually active population.2 45 46 Legal climates and STI testing regulations for sex workers vary across Australian jurisdictions. Despite much more frequent testing of the women in Victoria, STI (gonorrhoea, chlamydia, trichomoniasis, and Mycoplasma genitalium infection) prevalences have been found to be uniformly low (0–3.6%) in representative samples of sex workers tested in brothels in Melbourne, Sydney and Perth.42 In Sydney and Perth, STI screening is voluntary, and the appropriate screening interval is negotiated between the woman and her clinician on an individual basis. This also suggests that relaxing STI screening requirements in Victoria may not result in a noticeable change in STI transmission rates. Since STI screening varies between jurisdictions, but epidemiology of STIs and client behaviour is relatively similar, a change in policy in Victoria could have little change in social perceptions or spread of STIs but could save considerable financial and time resources. Our study suggests that the current laws mandating regular screening in Victoria may be using valuable resources in ways that are not cost-effective and should be reviewed.
Mandatory testing was introduced when the sex industry was decriminalised in Victoria in 1984 in the context of a general fear of the emerging AIDS epidemic and limited knowledge about transmission. However, sex workers have significant personal incentives to avoid the acquisition of STIs, so consistent condom use has been an industry norm since the 1980s. The majority of STIs that are transmitted to sex workers are now from their regular non-commercial partners, and not from their commercial sexual partners.2
There are also legal and ethical dimensions of STI screening of sex workers that require consideration. Regulation is carried out in other industries of goods and services in order to protect the public (eg, food/restaurants, medical devices, consumer products, health status of healthcare personnel, etc). There may be obligations and responsibilities for the government to ensure that sex workers do not have STIs. If clients acquire STIs from sex workers and then infect their regular partners, marital disruption (and attendant costs) could be significant. The acquisition of infections may produce psychological problems and cause other harm. Such outcomes could be grounds for awarding punitive damages in legal cases. Reviewing current regulations for screening in Victoria should consider the potential for such legal and ethical liabilities (and corresponding financial liabilities) as well as screening practices in similar settings where frequent testing is not mandatory.
Our study has a number of limitations. First, we only considered the health sector costs and outcomes related to mandatory screening for STIs. One could argue that there is a value related to reassurance for sex workers, clients and the wider community in regular STI testing. It is not clear whether or not the decision by a client to visit a sex worker is affected by knowledge that the sex worker has been screened for STIs in the last 4 weeks. Second, we used costs and outcomes of infections that were derived from the literature and an expected value analysis. This approach allows comparisons between our results and the cost-effectiveness of other interventions for HIV prevention such as antenatal testing of pregnant women. Third, we only included the infections occurring in the commercial sexual partners of sex workers, but not infections in the sex workers themselves or their non-commercial partners. However, such infections are personal health issues unrelated to the women's occupation. Fourth, our model simply investigated infections that remain between testing periods and did not consider other dynamic features associated with disease transmission such as possible clearance of bacterial infections due to the host immune response or background antibiotic use. Our simple static model does not take into account onward transmission in the population. This method is appropriate for analysis of low incidence settings, but if the methods were to be applied elsewhere to a location of high incidence, then this simple transmission model would underestimate the contribution to control and therefore overestimate the cost per case averted. However, this model would be appropriate for other settings of relatively low incidence. Fifth, there may be some sex workers who are not tested as frequently as required by law, or not tested at all. These women may have greater levels of infection, which is not accounted for in our analysis. However, the number of such women is believed to be small. Lastly, we did not carry out a detailed multivariate sensitivity analysis, although we did explore the impact of changes in STI incidence and condom use (table 2). We also determined that the most important factor in the model is the average time between tests. The influence of this parameter on the annual cost of screening, cost per infection averted, cost per QALY saved, marginal cost-effectiveness ratio and total savings was shown in figures 1–3. It is also important to note that if the screening programme were removed or if there were long intervals between testing, then it may be difficult to ascertain whether STI incidence changes. If there were outbreaks or local epidemics, then the cost–benefit estimates could also change substantially. Such changes may go undetected without a frequent screening programme; however, it is also possible that screening less frequently allows more sex workers to be screened.
Our simple model has been useful to provide insight into the magnitude of the expenditure and effectiveness in preventing infections in male clients with respect to the frequency of testing for STIs in female sex workers. In conclusion, we show that mandatory regular screening of sex workers for STIs and HIV is not cost-effective. We propose that resources could be better spent on more cost-effective interventions instead. Furthermore, screening intervals for sex workers in any jurisdiction around the world should be based on local STI epidemiology. Specifically, the cost-effectiveness of screening for STIs in any setting is highly dependent on the incidence of the infections which are likely to be geographically specific and the behaviour of sex workers in that setting.
Key messages
Commercial sex is licensed in Victoria, Australia, such that sex workers are required to test regularly for STIs, despite very low incidence and prevalence.
It was determined that mandatory screening of sex workers at current frequencies is not cost-effective, and costs are well beyond normal willingness to pay thresholds.
Screening intervals for sex workers should be based on local STI epidemiology and not locked by legislation.
Appendix 1 Expected value analysis for costs and utilities for gonorrhoea and chlamydia
Introduction
There are no published data of the costs or utilities of chlamydia and gonorrhoea infection in men. We use an expected value analysis to estimate the costs and utilities of infection, and associated complications in men who acquire infection over a 12-month period, from a health perspective. The costs are undiscounted in Australian dollars and based on costs for 2006–2007.
Method
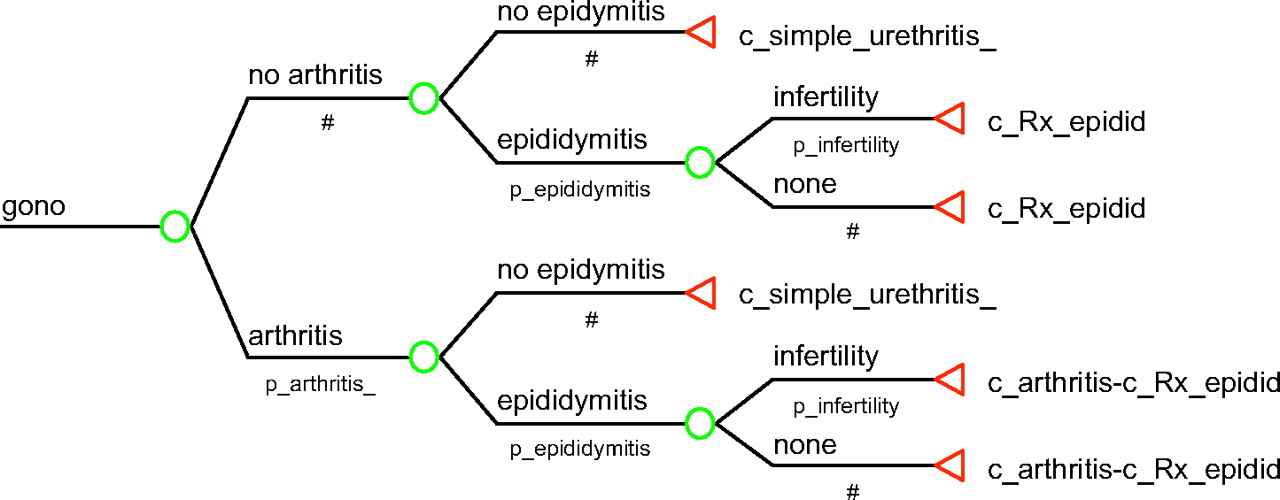
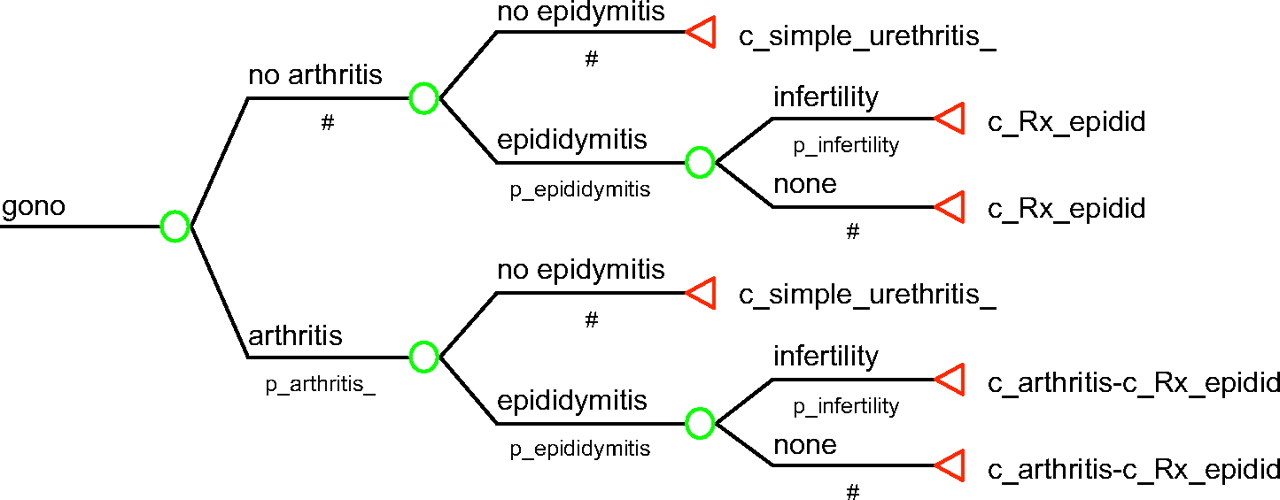
An expected value tree was constructed using TreeAge, with input variables drawn from Australian government medical and pharmaceutical rebates and the published literature; when variables were not available, we use the assumptions of an experienced sexual health physician (BD) and primary care doctor (JA); for epididymitis we adapt the utility loss associated with erectile dysfunction to mimic the loss of quality of life associated with sexual dysfunction. No utility loss is assumed for simple uncomplicated cases of infection. The variables include costs, probabilities and the decrements in utility over a 12-month period associated with specific complications.
The expected value analysis tree for both conditions is represented in figure AI. Input variables for chlamydia are in table AI and for gonorrhoea in table AII. The components for reactive arthritis related to chlamydia and septic arthritis for gonorrhoea are calculated from the clinical pathways described in tables AIII, AIV respectively.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Expected value analysis tree for gonorrhoea and chlamydia.
Costs associated with chlamydia infections
Costs associated with gonorrhoea infections
Costs associated with reactive arthritis (chlamydia)
Costs associated with septic arthritis (gonorrhoea)
We assume that 3% of men will experience arthritis and/or epididymitis associated with each condition. In the chlamydia tree, arthritis is reactive arthritis; in the gonorrhoea tree, it is septic arthritis. We also assume that 10% of men with epididymitis will become infertile.
To estimate the costs of admission with septic arthritis due to gonorrhoea, a multistep approach is taken: the International Classification of Diseases version 10 classifies septic arthritis due to gonorrhoea as A54.4+47; using this code we search the clinical profiles of National Admitted Patient Care Collection (NAPCC)48 to identify the diagnostic related group (DRG) codes associated with admission for septic arthritis, I67A/B; with these DRG codes, we search the 2006–2007 National Admitted Patient Care Collection49 to discover the number of separations for each DRG; the values of both DRGs are contained in Round 11 (2006–2007) Cost Report49; a weighted-average cost per separation is calculated using the proportions of each type of DRG to produce a cost per inpatient separation with septic arthritis.
Conclusion
Our expected value analysis estimates the cost per case of chlamydia infection of $57 and the cost of gonorrhoea of $82. The utility lost in a year for each case of disease is 0.0085 quality-adjusted life years, or just over three quality-adjusted life days.
The estimate is only slightly sensitive to the cost of treatment of arthritis and epididymitis; for example, the cost of gonorrhoea falls by $3 when the cost of inpatient care is 50% of the base-case value.
References
Footnotes
Funding The National Centre in HIV Epidemiology and Clinical Research is funded by the Australian government Department of Health and Ageing, and is affiliated with the Faculty of Medicine, University of New South Wales.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour