Article Text

Abstract
Background In settings with poor sexually transmitted infection (STI) control in high-risk groups, periodic presumptive treatment (PPT) can quickly reduce the prevalence of genital ulcers, Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT). However, few studies have assessed the impact on HIV. Mathematical modelling is used to quantify the likely HIV impact of different PPT interventions.
Methods A mathematical model was developed to project the impact of PPT on STI/HIV transmission amongst a homogeneous population of female sex workers (FSWs) and their clients. Using data from Johannesburg, the impact of PPT interventions with different coverages and PPT frequencies was estimated. A sensitivity analysis explored how the projections were affected by different model parameters or if the intervention was undertaken elsewhere.
Results Substantial decreases in NG/CT prevalence are achieved among FSWs receiving PPT. Although less impact is achieved among all FSWs, large decreases in NG/CT prevalence (>50%) are possible with >30% coverage and supplying PPT every month. Higher PPT frequencies achieve little additional impact, whereas improving coverage increases impact until NG/CT becomes negligible. The impact on HIV incidence is smaller, longer to achieve, and depends heavily on the assumed NG/CT cofactors, whether they are additive, the assumed STI/HIV transmission probabilities and STI durations. Greater HIV impact can be achieved in settings with lower sexual activity (except at high coverage), less STI treatment or high prevalences of Haemophilus ducreyi.
Conclusions Despite the model's assumption of homogeneous risk behaviour probably resulting in optimistic projections, and uncertainty in STI cofactors and transmission probabilities, projections suggest PPT interventions with sufficient coverage (≥40%) and follow-up (≥2 years) could noticeably decrease the HIV incidence (>20%) among FSW populations with inadequate STI treatment.
- Periodic presumptive treatment
- sexually transmitted infections
- sex workers
- HIV
- STDS
- treatment
Statistics from Altmetric.com
Introduction
The prevalence of sexually transmitted infections (STIs) can be high among female sex workers (FSWs), and so interventions to control STIs among FSWs are of importance. Furthermore, as many STIs are asymptomatic, periodic presumptive treatment (PPT) has been used to quickly reduce the prevalence of STIs amongst FSWs.1 2 To some extent, these interventions are stop-gap measures until other services becomes sufficient.
So far, most PPT interventions have used azithromycin to reduce the prevalence of Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT),1–6 with one also impacting on Haemophilus ducreyi (HD).2 Although, many have shown reductions in STI prevalence amongst FSWs, few studies have adequately assessed the possible impact on HIV transmission, and none have observed a decrease.5 This could be due to a lack of power, insufficient follow-up or because the treated STIs may have a small effect on HIV transmission in that setting.
Typically in PPT interventions, FSWs are seen every 1–3 months, irrespective of symptoms, whereupon they are presumptively treated for specific STIs. However, none have explored the relative effectiveness of different frequencies or coverages of PPT, or explored how effectiveness varies by setting. This analysis uses mathematical modelling to explore the importance of these issues for the impact of PPT in a homogeneous population of FSWs and clients. Specifically, the analysis looks at the impact of PPT on NG, CT and HIV transmission in Johannesburg (South Africa), Cotonou (Benin) and Laos, and the additional impact on HD transmission in Free State (South Africa).1–4 7
Methods
Model development
A dynamic deterministic compartmental mathematical model was developed to model the impact of a PPT intervention on FSWs and their clients. To focus on the effect of different PPT intervention characteristics, and because of behavioural data limitations, the model did not incorporate heterogeneity in sexual risk behaviour and FSWs and clients were assumed to mix randomly to form commercial sex partnerships irrespective of intervention status.
The model includes the transmission of NG, CT, HD and HIV, and models their cofactor effect on HIV transmission.8 If either partner has an STI, the HIV transmission probability is multiplied by the corresponding STI cofactor. For partnerships with multiple STIs, cofactors are summed. Through treating these STIs, the effect of PPT on HIV transmission was modelled.
The STIs incorporated into the model were modelled differently. When an individual becomes infected with NG/HD they recover at a constant rate and then become susceptible again. Conversely, when an infected individual recovers from CT, a proportion become ‘resistant’ and are less susceptible to re-infection, whereas the remainder become fully susceptible again. This model structure is similar to other CT models9 10 and is included because of evidence for acquired CT immunity,11 12 although there is uncertainty about the nature of this immunity. Individuals in the ‘resistant’ state can still become infected but always return to the ‘resistant’ state after recovery and never lose this resistance. Lastly, when an individual becomes HIV-infected they enter the acute phase with higher viraemia, followed by the chronic infection stage, which continues until they leave the population due to HIV-related morbidity.
The model assumes that after a specific time the PPT intervention starts recruiting FSWs at a constant rate (α) until a certain predetermined ‘target’ coverage is reached. The remaining FSWs are never reached by the intervention and have the pre-PPT rate of STI recovery. Once a FSW is recruited they receive their first PPT dose, which treats any NG, CT or HD infection they may have and protects them from re-infection for a short duration (1/η) if the drug used has a long half-life, such as azithromycin.13 14 When they leave this ‘protected’ state they become susceptible again until they receive their next PPT, which occurs at a specific rate depending on PPT frequency (ω). FSWs and clients leave the population due to HIV-related morbidity or when they stop sex work or buying sex, and are replaced by susceptibles such that the population and intervention coverage remain stable. FSWs are assumed to not drop out from the PPT intervention.
The model structure for NG, CT and HIV are shown in supplementary figure 1 (HD has same structure to NG), the parameters are defined in table 1 (and more fully in supplementary table 1) and the model equations are in the supplementary equations file.
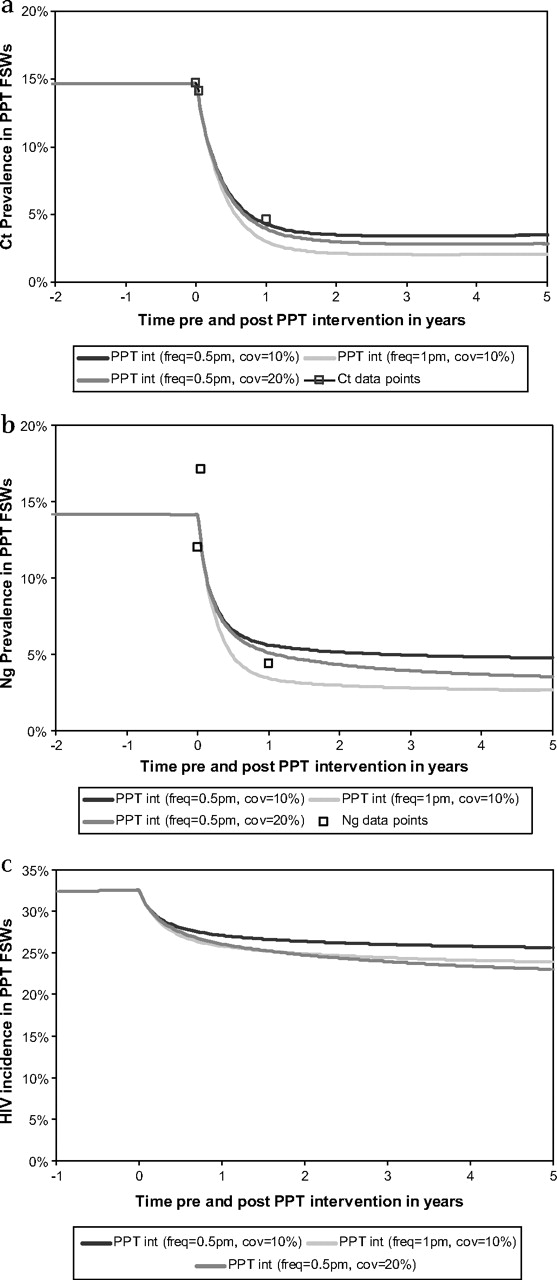
Projected impact of periodic presumptive treatment (PPT) on the prevalence of Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT) and HIV incidence among the female sex workers (FSWs) reached by the intervention in Johannesburg. (A) Prevalence of CT. (B) Prevalence of NG. (C) Incidence of HIV per year assuming cofactor of 3 for NG and 2 for CT.
Model inputs for the PPT model for different settings
Model parameterisation and fitting
The model was fit to epidemiological data from each setting with and without their PPT intervention (see epidemiological data in table 1). Two of these interventions have been described previously,1 2 with details for all four in table 1. All the interventions estimated the impact on NG/CT transmission, and HD transmission in Free State, of periodically treating high-risk women with azithromycin. All had ≤12 months of follow-up with treatment given every 1–2 months. Two studies were randomised controlled trials (Johannesburg and Cotonou) and the others were pre/post-intervention comparison studies (Laos and Free State).
To parameterise the model, biological inputs were obtained from the scientific literature and behavioural/epidemiological inputs were derived from different sources.1 2 4 7 15–17 Because of parametric uncertainty, the model was fit to available epidemiological data by varying certain parameters across their uncertainty bounds. These included the HIV/STI biological parameters and behavioural parameters such as the number of FSWs seen by a client per month. The model was first fit to HIV/STI data from Johannesburg and then to the other settings. To fit the model to HIV/STI data from the other settings, behavioural and epidemiological inputs from that setting were used, whereas most biological parameters were kept fixed to the values used for Johannesburg. HD was only modelled in Free State because the other settings had low or undocumented HD prevalences. All model fitting was done with the Berkeley madonna ‘curve fitting’ routine that minimises the root mean square deviation between the data points and model projections. Further details on the model fitting methods are in the supplementary methods file and the biological and behavioural model inputs for each setting are in table 1 (and more fully in supplementary table 1).
Impact projections
The Johannesburg model fit was used to produce baseline projections of the impact on FSW NG/CT prevalence and HIV incidence of the Johannesburg PPT intervention at its current coverage of the FSW population (10%) and frequency of PPT (once every 2 months), and if it had reached more FSWs, the PPT frequency had been higher or the intervention continued for longer.
Because of uncertainty in many model parameters, a sensitivity analysis was undertaken to explore how the baseline impact projections would vary for univariate changes in each model parameter (by ±10%), or if STI cofactors were not additive, CT immunity was non-existent or they had used a drug with a shorter half-life. The output for this analysis was the impact on NG/CT prevalence and HIV incidence of a range of PPT interventions after 2 years. In addition, the model fits for Laos, Cotonou and Free State were used to explore the impact on NG and HD (only Free State) prevalence and HIV incidence of the same range of PPT interventions.
Results
Baseline impact projections for Johannesburg
Figure 1 shows that the projected impact of the Johannesburg PPT intervention (10% of FSWs reached every 2 months) on NG/CT prevalence among FSWs reached by the intervention agrees with data from the intervention. They show that substantial impact can be achieved among reached FSWs at this PPT frequency, but that greater impact would have been achieved if more FSWs had been reached and PPT given more frequently. For the baseline NG/CT cofactors8 (3 and 2, respectively), figure 1c suggests the Johannesburg PPT intervention would have decreased the HIV incidence amongst reached FSWs by 20% after 3 years.

{kind=link}
{kind=link}
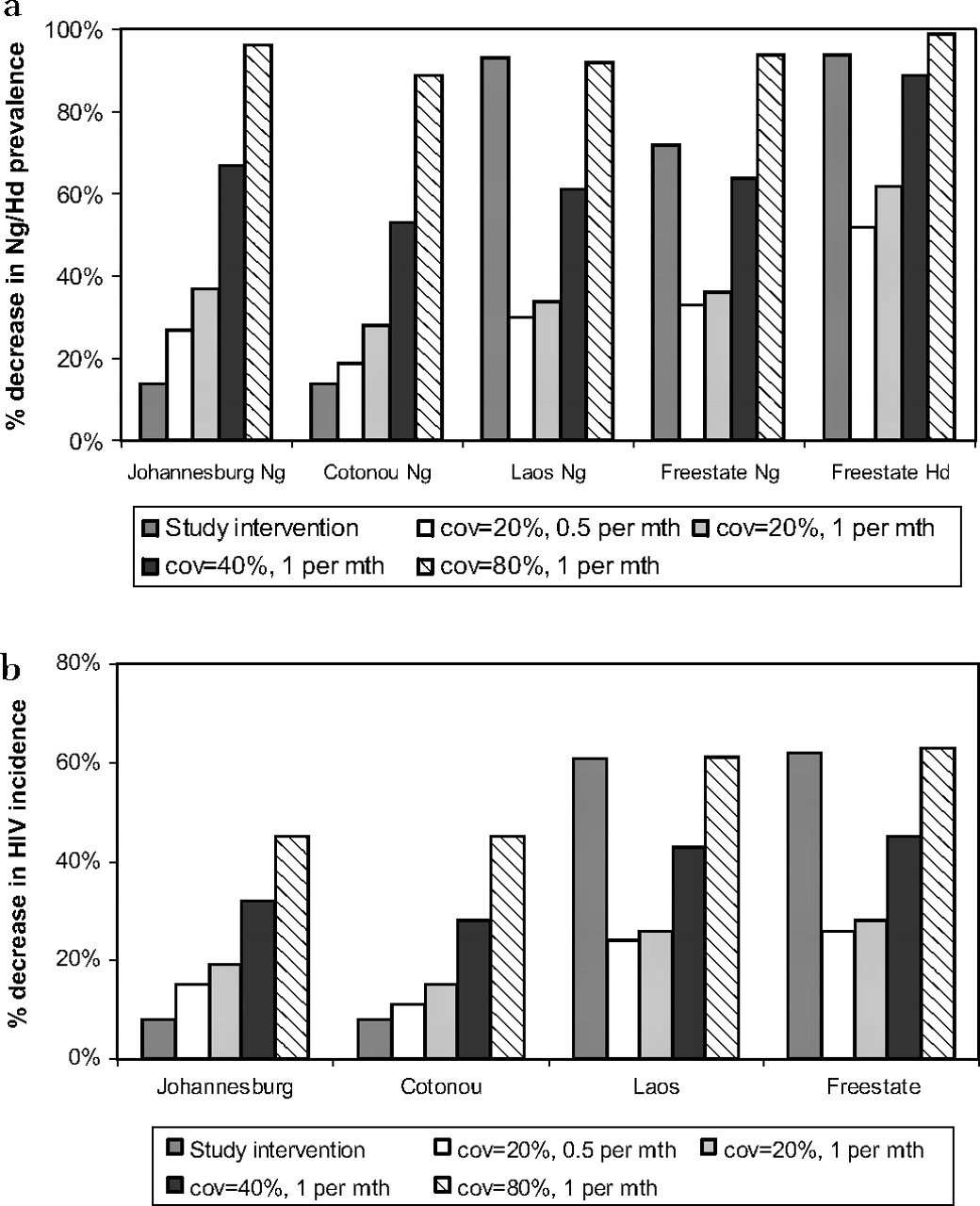
Projected 2 year impact of periodic presumptive treatment (PPT) on the relative decrease in Neisseria gonorrhoeae (NG) prevalence (and Haemophilus ducreyi (HD) prevalence for Free State) and HIV incidence amongst all female sex workers (FSWs) in Johannesburg, Cotonou, Laos and Free State (compared to no intervention) for each study site intervention and for other frequencies of PPT and coverage levels. a. Relative decrease in NG and HD (only Free State) prevalence compared to no intervention. b. Relative decrease in HIV incidence compared to no intervention.
The impact of PPT on the whole FSW population is smaller than among reached FSWs, depends more on the proportion of FSWs reached and takes longer to achieve. For instance, the model projects the current intervention attains a 10% decrease in HIV incidence after 3 years in the whole FSW population, with 40% of this being achieved after 1 year compared to 70% amongst reached FSWs.
Effect of frequency and coverage on impact projections
Supplementary figure 2 shows that if the PPT frequency is less than once every 2 months then small increases in PPT frequency substantially increase the intervention's impact on NG/CT prevalence and HIV incidence amongst all FSWs. However, little is gained from increasing the PPT frequency above once per month. Increasing the PPT coverage increases impact until the FSW NG/CT prevalence becomes negligible, with a ∼60% coverage being sufficient for NG and ∼75% for CT in Johannesburg. Above this coverage, the HIV incidence will not decrease further (47% for Johannesburg after 2 years with baseline NG/CT cofactors) dependent on how much NG/CT contributed to HIV transmission in that setting. The model also shows that impact is achieved if the PPT frequency is zero, because recruited FSWs still receive their initial PPT.
Sensitivity analysis
When the NG/CT transmission probabilities or duration of infection are increased by 10%, supplementary figure 3 (only shows parameters that resulted in ≥5% deviation in impact projections, see supplementary figure 4 for other parameters) shows that less impact (by up to 24%) is achieved on NG/CT prevalence. This also occurs for the impact on HIV incidence, except at high frequencies/coverages of PPT where greater impact can occur. Similar changes in NG/CT/HIV-impact occur when adjustments are made to other parameters that result in the baseline NG/CT prevalence increasing. These include increases in the frequency of commercial sex, increases in the condom failure rate (changes in the proportion of sex acts where a condom is not used has same effect and so is not shown here) or assuming no CT immunity. This suggests that less NG/CT impact will be achieved in FSW populations with greater unprotected exposures and similarly for the HIV impact except at high frequencies/coverages of PPT.
Supplementary figure 3 also shows that greater NG/CT-impact occurs when these parameters are decreased (by up to 38%). However, because NG/CT now contributes less to HIV transmission due to their lower baseline prevalence, the HIV impact is generally reduced except possibly at low PPT frequencies/coverages where the greatest increase in NG/CT-impact occurred. These projections show that the impact projections are sensitive to any parameter that has a large effect on NG/CT prevalence.
As expected, PPT has less HIV-impact when the NG/CT cofactors are reduced or they are not additive. If they are 10% lower, then 3–4% less HIV-impact is achieved by a range of PPT interventions, whereas similar increases in HIV-impact occur if they are 10% higher. If the STI cofactors are not additive then up to 13% less HIV-impact is achieved, with the reduction being most pronounced at lower PPT frequencies/coverages. Similar results occur when the HIV transmission probabilities are increased.
Azithromycin, a drug with a long half-life, was used in Johannesburg and other PPT settings. Using a drug with a shorter duration of protection (½ week instead of 1 week) could have reduced the HIV/NG/CT-impact by up to 10% after 2 years. All other parameters have a small effect on the HIV-impact projections.
PPT impact in other settings
Using the model fits for the other settings (supplementary figure 5) figure 2 suggests that the impact of PPT in Cotonou will be slightly lower than in Johannesburg due mainly to their higher NG prevalence. In contrast, PPT could achieve greater HIV-impact in Laos and Free State and PPT frequency is likely to be less important.
The increased HIV-impact in Free State is partly due to the substantial impact PPT has on HD transmission due to its short duration and azithromycin protecting against re-infection for ∼4 weeks14 and its large cofactor for HIV transmission. However, there is uncertainty around the HD cofactor8 18 with the projected HIV-impact being 25% lower if the HD cofactor was 5 instead of 15, and 13% higher if it was 25 as assumed elsewhere.9
Discussion
This mathematical modelling analysis explored the impact of different PPT interventions in four settings that have undertaken PPT interventions. The analysis has several limitations. Firstly, the model simplified the behavioural heterogeneity that occurs amongst FSWs. This was due to data limitations and because it was not the analyses main focus. This simplification probably resulted in optimistic impact projections because PPT will have less impact in more sexually active FSW sub-populations that have higher STI prevalences and contribute more to the epidemic. In addition, these FSWs may also be harder to reach and more easily lost to follow-up, so further reducing impact. Secondly, other than Johannesburg, singular model runs were used to make projections for each setting and so uncertainty was not incorporated into the projections. Thirdly, some settings had insufficient epidemiological data and so estimates were obtained from other sources. These limitations probably reduced the accuracy of our projections, but are unlikely to affect the general insights. Lastly, the study did not look at other PPT regimens, such as azithromycin plus cefixime, which would be more effective in areas where gonococcal resistance to azithromycin is emerging.
The model projections suggest that it is relatively easy to achieve substantial and rapid (∼1 years) decreases in NG/CT/HD prevalence among FSWs reached by a PPT intervention. However, although less impact is achieved in the overall FSW population, large (>50%) reductions in NG/CT/HD prevalence are still achieved with moderate coverage (>30%) and a PPT frequency of once a month. In addition, HD should be easy to control with a low coverage and PPT frequency, especially when azithromycin is used because it protects against re-infection for ∼4 weeks.14 Higher PPT frequencies are required for drugs with shorter half-life,14 such as cefixime.
The resulting decrease in HIV incidence due to these decreases in STI prevalence can be large (>40%), but takes longer to achieve (2–5 years) and is dependent on the assumed NG/CT/HD cofactors (3 for NG, 2 for CT and 15 for HD), whether the effect of multiple STI cofactors is additive and epidemiological setting, with more impact being achieved in settings with high HD prevalence. In addition, uncertainty in other parameters, especially the NG transmission probability (0.17 per sex act) and duration (2.6 months for Johannesburg), HIV transmission probabilities (0.0061 per sex act for female-to-male in Johannesburg) and nature of CT immunity (50% of resolved infections become resistant with their susceptibility reduced threefold) also heavily affect the accuracy of our projections. Although the parameter values used are similar to other modelling studies9 19 20 and data estimates for the NG transmission probability (0.19–0.25 per sex act21 22), duration of untreated NG infection (4 months23), HIV transmission probability in low-income countries (0.0087 per sex act for female-to-male24), NG/CT/HD cofactors (2 for NG and CT8 and <25 for HD18), it is likely that similar parameter estimates would have resulted in different impact projections. Additionally, uncertainty in the nature and existence of CT immunity11 12 will also have resulted in uncertainty in our model projections. This emphasises the importance of undertaking model sensitivity analyses to determine the robustness of a model's projections, and suggests that these model projections will have a degree of uncertainty associated with them.
Although this analysis seems to contradict existing PPT studies that did not observe decreases in HIV incidence,5 the results actually suggest that these studies may have been too optimistic in the expected drop in HIV incidence that would occur during their PPT interventions. Specifically, in the Kenyan trial,5 azithromycin was given once per month for 2 years to ∼25% of the screened FSWs. At this coverage, the baseline model projections for Johannesburg suggest a 27% decrease in HIV incidence among the reached FSWs over 2 years and a 13% decrease in HIV incidence among the not reached FSWs. Therefore, the difference in HIV incidence between the FSWs receiving or not receiving PPT would have been ∼14%—much lower than the hypothesised 50% decrease in HIV incidence and well within the confidence intervals for their observed decrease in HIV incidence.
With increasing PPT frequencies, the model projects that the impact on NG/CT/HD prevalence and HIV incidence increases until the PPT frequency is about 0.5–1 per month, above which little additional impact is achieved. This is dependent on setting, with a lower PPT frequency being required in Laos and Free State where FSWs have fewer unprotected client exposures and/or a longer duration of NG/CT infection due to less underlying STD treatment. In contrast, an intervention's impact consistently increases with coverage until the NG/CT/HD prevalence becomes very low. This occurs at sub-optimal coverage if the PPT frequency is sufficient—∼75% coverage for CT in Johannesburg and ∼50% coverage for HD in Free State. These coverage thresholds can be viewed in a similar way to herd immunity coverage thresholds, but caution should be taken generalising them because they will be elevated by the introduction of STIs by migrating FSWs/clients or the general population. The maximum impact of PPT on HIV incidence occurs at these coverage thresholds.
The analysis also showed that higher coverage levels and PPT frequencies may be required to achieve the same impact in settings with higher frequencies of unprotected sex. However, if high PPT intensity (coverage and frequency) is achieved, greater impact on HIV incidence can be expected. The reduced impact at lower PPT intensity is due to more STI re-infection occurring in populations with higher frequencies of unprotected sex, whereas the increased impact at higher PPT intensity results from STIs contributing more to HIV transmission in populations with higher STI prevalences.
In conclusion, although our projections are likely to be optimistic because FSWs are assumed to have homogeneous risk behaviour, the results still suggest that PPT interventions can be effective at rapidly reducing the prevalence of NG/CT/HD among FSWs if sufficient coverage is achieved (>30% of FSWs). However, any resulting reductions in HIV incidence will be smaller and take longer to occur. Little can be expected over 1 year, and only small reductions in HIV incidence will occur in the whole FSW population over 2 years unless ∼40% of FSWs are reached or HD is prevalent. Lastly, PPT interventions should be part of a comprehensive package of prevention interventions because, otherwise, any reduction in STI prevalence and HIV incidence will quickly return to pre-intervention levels when PPT is stopped.6
Key messages
Periodic presumptive treatment (PPT) interventions can be effective for rapidly reducing the sexually transmitted infection (STI) prevalence among female sex workers (FSWs) reached by the intervention.
If sufficient coverage is achieved (>30% of FSW population), then PPT interventions can effectively reduce the STI prevalence among all FSWs.
Large impact gains are achieved from increasing the PPT frequency when less than once every 2 months, but little is gained above once per month.
PPT interventions with sufficient coverage (≥40%) and follow-up (≥2 years) could noticeably decrease the HIV incidence (>20%) among FSW populations with inadequate STI treatment.
References
Supplementary materials
Web Only Data sti.2008.034678
Files in this Data Supplement:
Footnotes
Linked articles 40329.
Funding The analysis was funded by the World Health Organization (WHO). Peter Vickerman also received funding from the UK Department for International Development (DFID) funded Research Programme Consortium for Research and Capacity Building in Sexual and Reproductive Health and HIV in Developing Countries. The views expressed are those of the authors and cannot be taken to reflect the official opinion of the London School of Hygiene and Tropical Medicine, DFID or WHO.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.