Article Text

Abstract
Objective The aim of this study was to quantify differences in patterns of sexual behaviour among men who have sex with men and women (MSMW) compared with men who have sex with men only (MSMO), and to examine the extent to which bisexual behaviour may act as a bridge for introducing HIV infection into the general population.
Methods A cross-sectional survey in Bangalore city in 2006, which sampled men seeking sex with men in public places and hammams (bath houses where transgender individuals sell sex to men).
Results Among a sample of 357 men reporting same-sex behaviour; 41% also reported sex with a woman in the past year and 14% were currently married to a woman, only two of whom had informed their wives about having sex with men. Condom use was very inconsistent with all male partners, while 98% reported unprotected vaginal sex with their wives. MSMW reported lower rates of risky behaviour with other men than MSMO: fewer reported selling sex (17% vs 58%), or receptive anal sex with known (28% vs 70%) or unknown (30% vs 59%) non-commercial partners.
Conclusion Bisexual behaviour was common among men seeking sex with men sampled in this survey. Although MSMW reported lower rates of risky sexual behaviour with male partners than MSMO, inconsistent condom use with both male and female partners indicates a potential means of HIV transmission into the general population. HIV prevention programmes and services should reach bisexual men who potentially expose their male and female partners to HIV.
- Bisexuality
- bridging behaviour
- HIV
- homosexuality
- India
- men who have sex with men
Statistics from Altmetric.com
Approximately 2.5 million people in India were living with HIV in 2006, with the predominant mode of HIV transmission through sexual activity.1 2 At the national level, the overall HIV prevalence continues to suggest a concentrated HIV epidemic in India with, for example, a very high prevalence among men who have sex with men (MSM) (7.4%), which is more than 15 times the prevalence among antenatal clinic attendees (0.48%).2
Several studies in India have shown that MSM are a highly complex and diverse group, many of whom may have frequent sexual relations with women.3–9 A study in Andhra Pradesh found that 42% of MSM were married and that 50% reported sexual relations with a woman in the past 3 months.10 Some men might turn to men for sex due to difficulties accessing women. On the other hand, given the stigma associated with homosexual behaviour and the Indian penal code, which until recently cited sodomy as an offence,11 the pressure to deny male-with-male sex is pronounced, and many MSM marry women.12
It has been reported that condom use by MSM with spouses tends to be low, even more so than with male partners, which suggests that through bisexual behaviour, men could link circuits of high-risk male-with-male activity with the general female population.13 Some studies have shown that the number of cases of women infected with HIV through heterosexual transmission within marriage is increasing in India, and that the behaviour reported by the husband was an important risk factor for infection among many of these women.14 The frequency of bisexual behaviour among MSM, coupled with low condom use, high HIV prevalence and increased transmission efficiency of anal sex, means that the contribution of men who have sex with men and women (MSMW) to the HIV epidemic, through transmission to their female partners, could be substantial.15
Despite high rates of marriage among MSMW, prevention efforts have tended to consider bisexual and homosexual men as a single group, with less attention given to understanding the impact of their sexual relations with women. This may be partly because bisexual men tend not to identify socially with the MSM community.
There is evidence from Latin America that MSMW are more likely than men who have sex with men only (MSMO) to engage in insertive rather than receptive anal sex with other men; they also have unprotected sex with their female partners.16–19 Some have argued that MSMW with a non-‘gay’ identity may be at higher risk of HIV infection because of a lack of peer support and limited access to prevention services that are available to MSM who are more open about their sexuality.20
In order to develop more effective preventive responses, we need to understand sexual risk behaviour better, and the extent to which bisexual behaviour serves as a bridge for infection into the heterosexual population. The definition of identity among MSM in India is very complex and is increasingly the focus of qualitative12 21 22 and quantitative studies.23 24 Elsewhere, we have explored the identities of MSM, including transgender individuals, and how their sexual behaviour is related to identity.23 The objective of the current study was to disentangle the risk behaviour of MSMO compared with those who reported sex with men and women, which has important implications for both the HIV epidemic and prevention interventions in India. First, we quantified differences in the characteristics and sexual risk of MSMW and MSMO, and then explored differences in the risk behaviour of MSMW with their female partners compared with that with their male partners.
Methods
From July to August 2006, men/hijras from Bangalore city were sampled using a two-stage cluster sampling method described in detail elsewhere.23 In brief, following presurvey mapping of cruising sites, time–location cluster sampling was used for the selection of ‘floating’ populations in public-place cruising sites (locations where men seek other men for sex such as bus stops, train stations and public parks) to eliminate systematic bias of people with different levels of risk cruising at different days/times at a particular site. Conventional cluster sampling was used for the sampling of hammams (bath houses where transgender persons sell sex to men) as the population under study is ‘stable’ in these locations. In total 12 hammams and 112 public-place cruising sites were identified. Each of the 112 public-place cruising sites was divided into peak and off-peak periods and each cluster multiplied by the number of days sampled. A total of 5528 time–location clusters were defined, from which 77 were randomly selected. From a list of 12 hammams, eight were chosen at random. Within each cluster the aim was to achieve five interviews, resulting in a total of 400 interviews. The objective of the survey was to measure changes in selected behaviour over two time periods in years 1 (2006), 3 and 5 of the intervention, calculating the sample size accordingly.25 A power calculation was carried out to ensure the available sample size would provide enough power. In this example the outcome of interest was ‘ever reporting non-commercial sex with a man’, between MSMW and MSMO. The α level was set at 0.05, corresponding to a type 1 error, with a 5% probability. This resulted in 88% power in the survey.26
Men were eligible to participate in the study if they had had sex with a man at least once in their lifetime and were at least 18 years of age. In our analysis, men were classified as MSMW if they reported sex with a woman within a year before the interview. In this paper, the term ‘MSM’ is used to describe a behavioural phenomenon that encompasses both men and male-to-female transgender individuals (hijras). Although hijras do not socially and psychologically identify themselves as men, they are included in this study for two reasons. First, the programme through which respondents were recruited targets men and hijras, thereby creating a degree of overlap between their social networks and, second, many hijras engage in receptive anal intercourse.23
In India different categories of MSM, generally associated with different HIV risk behaviours, are often used and interpreted as characterising different identities of MSM. Five categories of MSM identities, all of which have been described in previous publications,12 23 27 were defined by the local non-governmental organisation at the outset of the study and were confirmed by a pilot study. The question asked in the interview was open-ended: ‘How do you identify yourself?’ with possible answers being hijra, kothi, double-decker, bisexual, panthi and ‘no identity’.
Mixing western notions of identity (homo–heterosexual) is unlikely to be recognised by Indian men unless they are of higher or middle class and have been exposed to western gay men or environments.12 Despite this, ‘bisexual’ was a term recognised and used by respondents during the pilot study. The interviewers were trained only to give examples of identities but not to probe the respondent or eliminate categories according to sexual behaviour.
Statistical analysis
The association between sociodemographic characteristics and bisexual behaviour was examined using the Wald test for continuous variables and Pearson χ2 tests with the Rao–Scott correction for categorical variables.28 Each outcome was related individually to the outcome, bisexual behaviour. A logistic regression model was created, adjusting for sociodemographic variables known to be important risk factors (or confounders) for bisexual behaviour based on the published literature. In constructing the multiple regression models for the adjusted analyses, all important sociodemographic variables were included, with the variable with the smallest p value chosen as the first independent variable in the multivariate model. There were no significant interaction terms and any missing data were excluded from the analysis. All statistical analyses took into account the survey design (clustering), in order to take into account the correlation between individuals when estimating variance and confidence interval, using SVY commands in STATA, version 10.29
Results
In total, 357 of the 572 men approached agreed to be interviewed, giving a participation rate of 62%. Figure 1 shows the extent of lifetime and current (past year) bridging behaviour by partner type. Over half of the sample (55%) reported sex with men and women in their lifetime; 45% reported sex only with men, and 3% reported sex only with men and hijras. No men reported having had sex only with hijras.

Lifetime and current (in the past year) bridging behaviour. MSMO, men who have sex with men only; MSMW, men who have sex with men and women.
Over the past year, 41% reported sex with men and women, of which 30% reported sex with men and women and 11% reported sex with all partner types—men, women and hijras. On the other hand, 12% of those reporting lifetime bisexual behaviour reported sex only with men in the past year, whereas 2% reported sex only with men and hijras (figure 1).
In our analysis, men were classified as MSMW if they reported sex with a woman (and man) within a year before the interview. MSMO were defined as men who reported having had sex with men only in the past year.
Sociodemographic characteristics
Over a third of MSMW (38%) and MSMO (33%) were recruited into the survey in public parks, and 12% of MSMO were recruited in hammams due to the higher proportion of hijras in this group (table 1). Those who reported bisexual behaviour in the past year were older on average than exclusively homosexual men. Age at first sex was significantly higher among MSMW than MSMO (19 vs 17 years).
Sociodemographic characteristics and behaviours of MSMW and MSMO
Most of the sample was Hindu and literate (71%), and this did not vary significantly between MSMW and MSMO. A third (34%) of all respondents had been married to a woman at some stage in their life. There were some differences among identities. More masculine identities such as panthis, double-deckers and bisexuals were more likely to have ever been married (38%, 27% and 63%, respectively) compared with 22% of kothis and no hijras. More details on the characteristics of different identities have been published elsewhere.23
The majority of MSMW were currently married (68%), and most married MSMW (66%) lived with their wife. Among men not reporting sex with a woman in the past year (MSMO), 3% were currently married.
Slightly fewer MSMW originated from Bangalore (47% vs 52%) and had ever had sex with another man outside Bangalore (25% vs 28%). Considerably more MSMW concealed their same-sex behaviour from their families than MSMO (96% vs 74%). Significantly fewer MSMW than MSMO perceived themselves to be at risk of contracting HIV (32% vs 46%).
Sexual identity and bisexual behaviour
HIV intervention programmes in India have tended to assert MSM identities typically described as passive (receptive) or active (insertive) in terms of sexual role in anal sex21 (see table 2). In brief, hijras are male-to-female transgender individuals; kothis have feminine characteristics and may cross-dress but remain biologically male; double-deckers and bisexuals are more masculine or neutral than kothis. Panthis have a masculine identity and may not self-identify as such although they are identified so by kothis or hijras. As previously described23 and in the present study, self-reported sexual identity was strongly associated with having sex with women. Although MSMW did not identify as bisexual: 43% self-identified as bisexual; 23% as panthi; 12% as double-decker; 11% as kothi, whereas 11% of MSMW did not self-identify with any group. No hijra reported sex with women.
Sexual risk behaviour of bisexual (MSMW) versus homosexual (MSMO) men
Sexual risk behaviour of MSMW and MSMO
As shown in table 2, there was no significant difference between MSMW and MSMO in terms of the type of male partner they first had sex with, or reporting anal sex with known or unknown non-commercial partners.
Men who sold sex were less likely to be MSMW than those who did not sell sex; whereas those who had ever bought sex from men and hijras were more likely to be MSMW. Men who reported ever having had non-commercial male partners were more likely to be MSMW than those who did not. Men who reported receptive anal intercourse were less likely to be MSMW than those who had insertive anal sex, with both known and unknown non-commercial male partners.
The results of the multiple logistic regression model are shown in table 2. After controlling for sociodemographic characteristics, the association between sex with men and women, and buying sex from male and hijra sex workers, remained significant, as did selling sex and receptive sex with known non-commercial partners. On the other hand, ever reporting non-commercial sex with men, as well as the type of anal sex with unknown non-commercial male partners, were confounded, and after controlling for sociodemographic variables, such as marital status and sexual identity, did not remain significant.
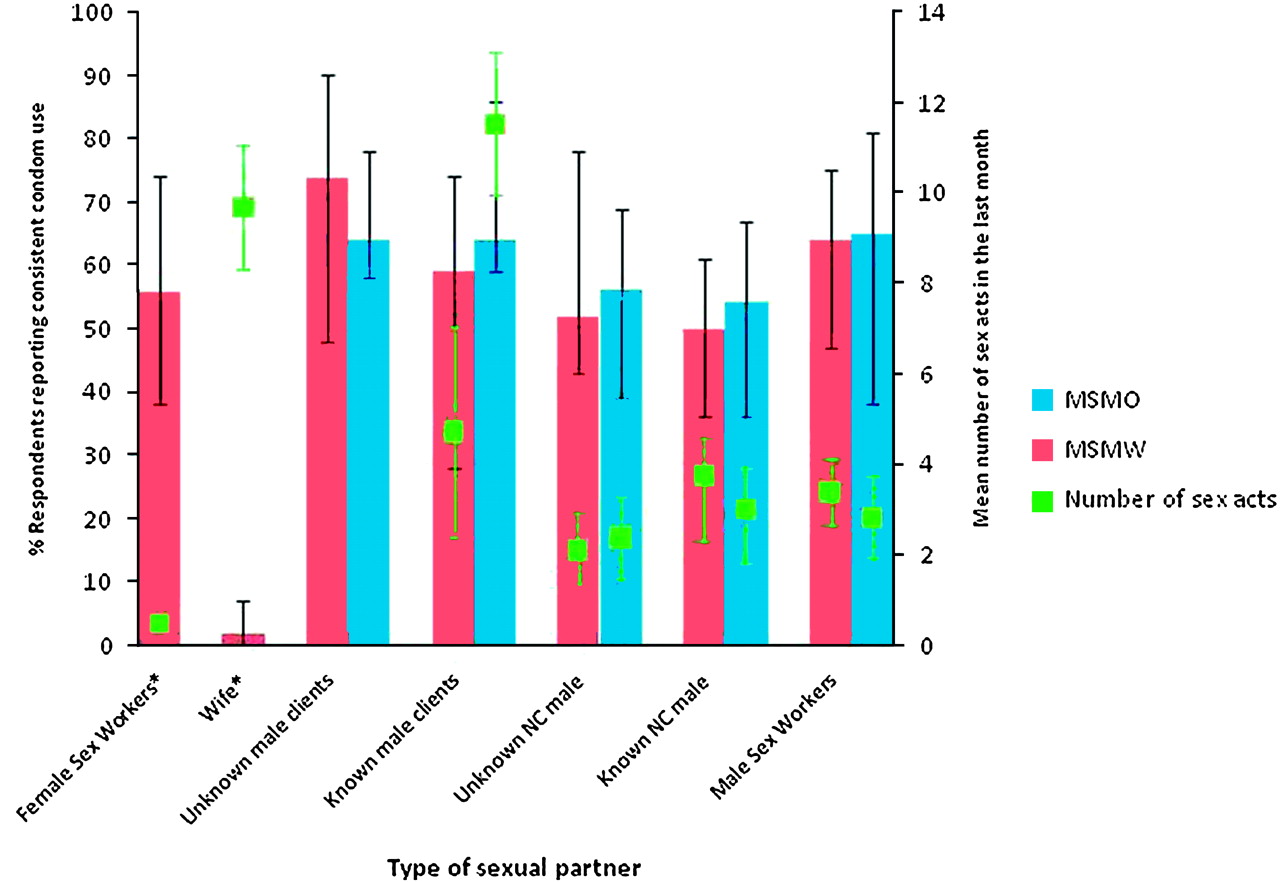
Consistent condom use and mean number of monthly sex acts by different types of partner
Consistent condom use was defined as ‘always’ using a condom with that partner or partner type. There were no significant differences in the rates of consistent condom use between MSMO and MSMW with different types of male partners, whether commercial or non-commercial (figure 2).

{kind=link}
{kind=link}
Percentage of respondents reporting consistent condom use and mean number of monthly sex acts by different types of sexual partners for men who have sex with men and women (MSMW) and men who have sex with men only (MSMO). NC, non-commercial.
Condom use was particularly low with wives (only 2% always used a condom with wives), even though the highest average number of monthly sex acts took place with wives (average 10 acts per month). Of those who had ever bought sex from a male sex worker (MSW), condoms were used consistently by 64% and 65% of MSMW and MSMO, respectively. This was higher than condom use with female sex workers (FSW; 56%).
MSMW reported significantly fewer sex acts with known clients (five per month) than MSMO (12 per month; p=0.05). However, the mean number of monthly sex acts with both unknown and known non-commercial male partners was similar for MSMW (two and three, respectively) and MSMO (two and four, respectively). Both MSMW and MSMO who bought sex reported an average of three sex acts per month with MSW (p=0.82). As shown in figure 2, inconsistent condom use did not necessarily correspond with the partner with whom they have the least number of sex acts.
Sexual behaviour patterns of MSMW with female partners
Among MSMW, the mean age at first sex with a woman (22 years) was higher than the mean age at first sex with a man (19 years; see table 3). This is consistent with the majority of MSMW reporting that their first sexual partner was male (66%). Most men reported vaginal sex with their wives (95%) and FSW (100%), and few reported anal sex with wives (5%), although this proportion was higher for anal sex with FSW (20%). Consistent condom use was lower for anal sex with both wives (0%) and FSW (33%) than for vaginal sex (see figure 2: 2% and 56%, respectively), although the numbers reporting anal sex with women were low. Twenty-two per cent of all MSMW were currently having sex with other female partners (besides cohabiting women and FSW).
Bisexual behaviour of MSMW in the past year
Discussion
MSM link circuits of high-risk activity with the general population. Bisexual behaviour was commonly reported among men who seek sex with men in the public places sampled in this survey. The findings from this paper are consistent with other research findings from India, with the proportions of MSM currently married to women ranging from 23% to 42%.8 10
Some differences were found between sexual identity and behaviour reported in this study, compared with others. It has previously been reported in qualitative research in Chennai (India) that engaging in sex with women is a source of stigma within the kothi community.29 In this study 11% of MSMW self-identified as kothis and only 43% as bisexual. The selection of participants based on self-identification as bisexual, rather than on the basis of current sexual practices, would thus have underestimated the true prevalence of bisexual behaviour.
MSMW reported lower rates of risky behaviour than MSMO, with lower proportions reporting selling sex to men and receptive anal intercourse, in both unadjusted and adjusted analyses. This is likely to be a reflection of the many MSMO that are kothis and hijras, who have previously been shown to be more likely than other identities to sell sex.23 However, a significant proportion of MSMW buy sex from sex workers (male, female and hijra), and of those who reported insertive and receptive anal sex with unknown non-commercial partners, 60% were MSMW. It was not possible to examine the frequency of sex acts by type (insertive, receptive or insertive/receptive) as the question was not asked at the interview; however, it would be interesting to look at this in future.
Condom use by MSMW with their wives was extremely low. A study carried out recently in Bangalore showed a high HIV-1 prevalence in both MSMO (20%) and MSMW (19%), so the risk of HIV transmission to the wives of MSMW is high (Karnataka Health Promotion Trust, Bangalore. Integrated Behavioural and Biological Assessment among MSM-T in Karnataka). In addition, many MSMW reported sex with FSW as well, with 20% reporting anal sex with a FSW in the past year. Given high HIV prevalence among FSW,30 this indicates a significant risk of HIV infection through sex with FSW.
An interesting finding was that MSMO were younger than MSMW (median 28 vs 33 years). This raises the question of whether some of the MSMO would go on to have sex with women, particularly through marriage. It would be worthwhile for future studies to examine this question in more detail, through, for example, examining the future intentions of young MSMO with regard to marriage or sex with other women.
A limitation of this study is that it included only men who seek sex with men in public places, and this may not reflect the population of MSM in the larger community. Furthermore, the overall participation rate was approximately 62%, which raises concerns over the representativeness of the study, and consequently the generalisability of the results. For example, many MSMW are unlikely to identify themselves as ‘MSM’, as reflected by the few respondents who had informed their families that they had had sex with men, and the substantial proportion married to women; it is likely that such men would have been less amenable to study participation. Nevertheless, the study does highlight the diverse range of homosexual and bisexual behaviours among MSM in India, which may have significant implications for the risk of HIV transmission to female sexual partners. Changing behaviour in this bridging population could slow the progression of the HIV epidemic. Previous studies have critically examined the use of indigenous sexual ‘identities’ that have been popularised by HIV-prevention programmes in India.21 23 Although the politics of such categories is not the focus of the current paper, it is noted that bisexual behaviour among MSM is correlated with identity, with nearly half of MSMW self-identifying as bisexual.
In this regard, at least two prevention efforts must occur: one that focuses on MSM who identify as such and another that reaches out to men who have male and female partners, but who may not identify as MSM or bisexual, and who seek sex in locations such as public parks. The latter group could be better reached by outreach workers with more behaviourally bisexual (and generally more masculine) MSM identities, such as panthis and bisexuals, rather than the often used kothi and hijra outreach workers.31
It is also important to focus on increasing condom use rates with the female partners of MSMW, who are generally perceived as low risk. This may be difficult to achieve and sustain, however, because the desire for children may compete with the concern to protect partners from HIV infection. Bridging to the general population will, however, continue to contribute to the HIV epidemic unless condom use with higher-risk partners becomes more consistent.
Key messages
Bisexual behaviour was common among this sample of men who seek sex with men in Bangalore.
Men who reported having sex with both men and women (MSMW) reported lower rates of HIV-related sexual risk behaviours with male partners than men reporting sex with men only (MSMO).
Inconsistent condom use by MSMW with both male and, in particular, female partners indicates a potential means of HIV transmission into the general population.
HIV prevention programmes and services, particularly those targeting MSM, need to ensure that they reach bisexual men who potentially expose their male and female partners to HIV.
Acknowledgments
The authors would like to thank the field team, as well as the men and transgender individuals who participated in this study, as well as Sangama and the Karnataka Health Promotion Trust for supporting and facilitating this study.
References
Footnotes
Funding The research project was supported in part by the Bill & Melinda Gates Foundation. The India AIDS Initiative, including this study, is supported by a grant from the Bill & Melinda GatesFoundation. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the Bill and Melinda Gates Foundation. MA is a national researcher of the Fonds de la Recherche en Santé du Québec, Canada (grant # 8722).
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Université Laval, Québec, Canada, Imperial College, London, UK and St Johns Medical College, Bangalore, India.
Provenance and peer review Not commissioned; not externally peer reviewed.