Article Text

Abstract
Background Apolipoprotein E is polymorphic in the human population. APOE4 has previously been reported to correlate with symptomatic oral and genital herpes disease.
Methods APOE was genotyped in 182 subjects with herpes simplex virus (HSV) 2 and in 62 subjects with HSV-1, including 44 subjects with both viral types for a total of 200 adults. HSV shedding was measured by PCR from swab samples obtained daily from mucosa for at least 30 days. Participants also maintained a diary of oral or genital lesions.
Results The APOE genotypes observed reflected the US white population and the Hardy–Weinberg equilibrium. Genital and oral HSV shedding was detected on 17.2% and 3.7% of overall days, respectively, whereas genital and oral lesion rates were 10.1% and 2.9%. Using Poisson regression and adjusting for known correlates of HSV shedding, a significant association was not observed between the APOE genotype and genital or oral HSV shedding, or genital HSV lesions. However, the presence of the APOE4 allele was associated with a higher rate of oral herpetic lesions, with a relative risk of 4.64 (95% CI 1.32 to 15.05, p=0.016).
Conclusions Variation at the APOE locus may be associated with clinical manifestations of HSV-1 infection, but does not appear to correlate with herpes simplex viral reactivation in humans.
- Apolipoprotein E
- genital herpes
- genotype
- herpes
- herpes simplex virus
- PCR
- viral shedding
Statistics from Altmetric.com
Herpes simplex virus (HSV) types 1 and 2 are ubiquitous human pathogens, infecting approximately 60% and 20% of US adults, respectively.1 Both viral types have a tropism for epithelial and neuronal cells. Their ability to undergo latency and reactivation in neurons leads to a phenotype of recurrent clinical disease in some persons and detectable, intermittent viral shedding in infected individuals.2 HSV-1 clinical disease typically affects the orolabial and ocular areas and HSV-2 is usually detected in the anogenital region.3 Whereas most persons who have antibodies to HSV-1 or HSV-2 do not have a clinical history of mucosal ulcerations, the current consensus is that all seropositive individuals have lifelong latent infection in neural ganglia and at least occasional shedding of virus. One possible explanation for this is variation in host genes that interact with HSV replication, the immune response to HSV, or the generation of clinically apparent signs or symptoms of infection.
Apolipoprotein E is a protein involved in the transport of lipids that is strongly linked to Alzheimer's disease (AD) pathogenesis. It is encoded by the autosomal APOE gene. Among the three common alleles (E2, E3 and E4), which vary in amino acid sequence at residues 112 and 158, the E4 allele has a pathogenic association with the prevalence and age of onset of AD. HSV-1 DNA can be present in both normal and AD brain tissues. Investigations into the interaction between HSV-1 and APOE alleles have suggested an association between HSV-1 DNA detection in AD tissues and the presence of the E4 allele.4 An association between the E4 genotype and a history of symptomatic HSV-1 was also detected.4 Mouse models also support an interaction between HSV infection and the APOE genotype.5–8
We have used daily home collection of anogenital and oral swabs from persons with HSV infection to define objectively the frequency of mucosal viral shedding and prospective diaries to characterise the frequency of oral and genital lesions. The relationship between the virological and clinical severity of genital HSV shedding and APOE variants was studied in 200 genotyped individuals.
Materials and methods
Study participants and procedures
All participants were 18 years or older, had serological evidence of HSV-1 and/or HSV-2 infection and no clinical or laboratory evidence of HIV infection, and were enrolled into prospective studies at the University of Washington Virology Research Clinic in Seattle or Westover Heights Clinic in Portland. Participants provided signed informed consent. Study protocols were approved by the University of Washington (Seattle site) or Western (Portland site) institutional review boards. Subjects did not receive anti-HSV therapy during the study observation period. A standardised history of HSV infection and general health was obtained. Subjects received gender-specific instruction on how to obtain swabs of the oral and/or genital and rectal regions, as previously described.9 10 Participants kept a diary of genital and oral symptoms and were seen in the clinic every 2 weeks for the collection of samples and diary review. The analysis included participants with data for 30 or more days at genital, oral, or both sites. Blood for DNA was collected by venipuncture.
Laboratory testing
Antibodies to HSV-1 and HSV-2 were detected by the University of Washington immunoblot.5 Antibodies to HIV-1 were detected by screening ELISA. Swabs were placed into phials containing 1 ml transport medium and refrigerated until laboratory processing. HSV DNA was detected by PCR.6 The PCR assay uses type-common primers to the HSV gene encoding glycoprotein B.7 8 An internal control was included in the PCR reaction to ensure that HSV-negative findings were not caused by inhibition. Samples were considered positive for HSV if we detected more than three copies of HSV DNA per 20 μl of specimen (ie, >150 copies of HSV DNA per ml of transport media).9 Results were analysed both dichotomously and, among positive specimens, as HSV copies/ml. Laboratory personnel were blinded to clinical data. Genomic DNA was isolated from blood collection tubes (Paxgene; Becton Dickinson, Franklin Lakes, New Jersey, USA) and measured with a spectrophotometer. APOE genotyping was performed by standard PCR restriction fragment length polymorphism-based methods.10
Statistical analysis
We examined the association between APOE alleles and the outcomes: viral shedding and mucosal lesions, at both the oral and genital sites, using Poisson regression. The rate ratios due to specific APOE alleles were adjusted for known influences on HSV shedding, such as gender, HSV-1 infection among HSV-2-infected persons, and time since HSV acquisition.2 11 The duration of infection (categorised as greater than 1 year, less than 1 year, or unknown) was also considered, as viral shedding is higher in the first year after primary HSV-2 infection.11 To analyse the relationship of the APOE genotype with the HSV DNA copy number, linear mixed models were used, both without and with adjustment for the factors mentioned above. Genotype frequencies were examined for independent assortment (Hardy–Weinberg equilibrium12) with the polynomial (a+b+c)2=a2+b2+c2+2ab+2bc+2ac.
Results
Virological and clinical outcomes
We studied 200 participants. Among these, 78 had both HSV-1 and HSV-2 infection, 107 had only HSV-2 infection and 15 had only HSV-1 infection. Overall, 44% were male and 86% were white (racial data were available on 87% of participants). Genital swabs were obtained from 182 HSV-2-seropositive persons (table 1). Among these, 143 (79%) had a history of genital herpes. This rate is higher than noted in serological surveys of HSV-2-seropositive persons, probably reflecting the enrolment at our research clinics predominantly of individuals with symptomatic genital herpes. Seventy-five (41%) persons were also HSV-1 seropositive. Oral swabs were obtained from 62 HSV-1-seropositive persons, including 47 (76%) who were also HSV-2 seropositive. Both genital and oral swabs and history were obtained from 44 of these dually seropositive persons.
Participants enrolled in the study
The virological endpoints were mucosal HSV shedding rates. Overall, HSV shedding data were available from 13 417 swab specimens. Among the 182 persons and 10 425 days with genital swabs collected, 1788 (17.2%) were positive for HSV. The median observed shedding rate was 13% (range 0–80%) of days. Among the 62 persons participating in the oral shedding cohort, 112 of 2992 oral swabs (3.7%) were positive. The median observed shedding rate was 0% (range 0–28%) of days.
The clinical endpoints were the rates of oral and genital lesions as noted in participant diaries. The number of days with oral lesion reports was fewer than the number of days with genital lesion reports, reflecting the smaller oral lesion cohort. Of the 11 770 days containing diary entries, genital lesions were noted on 1192 (10.1%) days. Among the 3431 days containing diary entries, oral lesions were noted on 99 (2.9%) days. The median reported genital lesion rate was 5%, ranging from 0% to 67% of days, with the corresponding median rate for oral sites of 0%, ranging from 0% to 29% of days.
APOE genotypes
APOE allele frequencies (table 2) were similar to those reported in the US population. Among the 400 alleles from 200 persons, the allele frequencies were 7.5%, 74.0% and 18.5% for APOE2, APOE3 and APOE4, respectively. It is well known that APOE4 has high allele frequencies in African-heritage populations (up to 22%).15 As expected from our high proportion of white subjects, our observed APOE4 frequency was similar to those reported from predominantly white groups.15 APOE genotype frequencies reflected the allele frequencies, and displayed independent assortment by the Hardy–Weinberg equilibrium and were similar to those reported13 for white populations (not shown). Among the participants in the genital herpes study, each of the six possible APOE genotypes was represented, with between one and 99 persons having each genotype. Among the individuals with oral herpes data, three genotypes were not represented (APOE 2/2, APOE 2/4 and APOE 4/4), whereas between 11 and 31 persons per genotype were present in the other three genotypes (APOE 2/3, APOE 3/3 and APOE 3/4).
APOE allele frequencies in the study population
Correlation between virological and clinical endpoints and APOE genotype
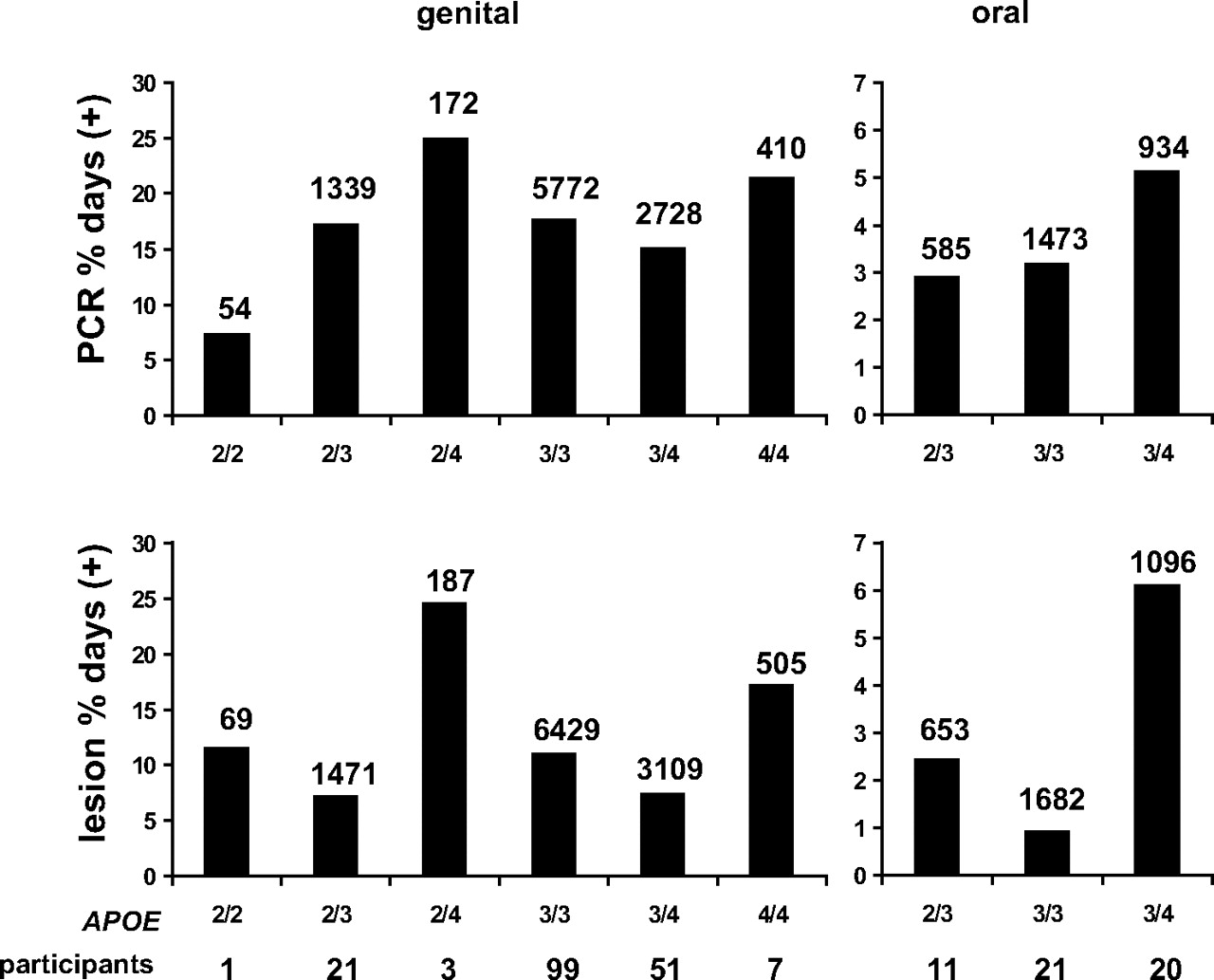
We examined the relationship between the APOE genotype and four distinct HSV outcomes: genital HSV shedding and lesions and oral HSV shedding and lesions (table 3). Bar graph representations of shedding and lesion data for (figure 1) show that genotypes containing APOE4 generally had the highest levels of HSV activity. The genital shedding rates over all days for genotypes 2/2, 2/3, 2/4, 3/3, 3/4 and 4/4 were 7.4%, 17.3%, 25.0%, 17.7%, 15.1% and 21.4%, respectively. The corresponding lesion rates were 11.6%, 7.2%, 24.6%, 11.1%, 7.5% and 17.2%, respectively. For participants with the 2/3, 3/3 and 3/4 genotypes in the oral herpes study, the oral shedding rates were 2.9%, 3.2% and 5.1%, respectively. The corresponding oral lesion rates were 2.5%, 1.0% and 6.1%. Within each genotype, large ranges were noted for shedding and lesion rates. Therefore, when the individual participants' shedding or lesion rates are analysed, overlap is present in both shedding rates and lesion rates between groups of participants with distinct APOE genotypes (not shown).
Poisson regressions for shedding and lesions

{kind=link}
Association of APOE genotypes and oral HSV shedding and oral lesions. The left bars refer to genital shedding rates (top) and lesion rates (bottom), whereas the right bars depict oral shedding (top) and lesions (bottom). The abscissa values differ between genital and oral sites. The numbers of days with data available are indicated over the bars for each genotype, anatomical site and study endpoint. The number of persons with each genotype is listed below the APOE genotypes across the ordinates.
Poisson regression was performed to examine what factors might be associated with shedding or lesions. The APOE genotype was not associated with genital HSV shedding or lesions. As expected, a history of symptomatic genital herpes was associated with genital lesion rates (table 3). For oral disease, the presence of any number of copies of APOE4 was associated with increased rates of oral lesions (relative risk (RR) 4.64, 95% CI 1.32 to 15.05, p=0.016), but not with oral shedding. Adjustment for gender, HSV-2 infection and time since the acquisition of infection (if known) yielded a RR of oral lesions of 4.04 (95% CI 1.09 to 15.01, p=0.037) for any APOE4 allele. Among participants with oral lesion data, each person with any copies of APOE4 also had a copy of APOE3. Therefore, it was not possible to examine whether the mechanism of association was dominant, recessive, additive or heterogeneous.
In 133 of 182 (73.1%) persons with genital herpes data and in 48 of 62 (77.4%) with oral herpes data, Toll-like receptor (TLR) genotyping was available.16 Previously, we have reported a relationship between TLR2 alleles and their associated haplotypes, and genital HSV shedding and lesion rates.16 Adjustment for the presence of TLR2-15607A/G did not alter the findings regarding the lack of association between genital shedding or genital lesions and the presence of APOE4, although TLR2-15607A/G remained predictive. Neither the presence of APOE4 nor TLR2-15607A/G were predictive of oral shedding in a multivariate model including gender, HSV dual infection and time since infection. After adjustment for these factors, the presence of any number of APOE4 alleles remained associated with a 3.53-fold increase in oral lesion rate (95% CI 1.35 to 9.22, p=0.010) while TLR2-15607A/G was not associated with oral lesions (p=0.75), although the size of the oral HSV cohort (62 persons) may have limited our power to observe an effect.
We also examined the relationship between the APOE genotype and the amount of HSV DNA detected using quantitative HSV DNA copy number data from 112 oral swabs and 1788 genital swabs. No significant difference in HSV copy numbers was noted between the most prevalent APOE genotype, 3/3, and any other APOE 3/3 genotype, and no difference was noted between individuals with and without any copies of APOE 4. These observations were true for both oral and genital quantitative virological measures.
Discussion
In a cohort of clinically and virologically well-characterised participants with genital HSV-2 or oral HSV-1, we observed an association between the APOE4 allele and higher rates of oral herpetic lesions. In contrast, we found no association between the APOE genotype and genital HSV shedding or lesion rates and no association with oral HSV shedding.
Our study had several strengths. We obtained objective viral shedding data in addition to collecting clinical information about lesions. Viral shedding represents the outcome of both neuronal reactivation and epithelial replication, and may occur with or without lesion formation. Shedding is important as it leads to the transmission of HSV. Our participants assessed lesions prospectively and were provided guidance in the assessment of lesions.2 Our primary endpoints, HSV lesion and shedding rates, were both studied as continuous rather than as dichotomous variables. Potential weaknesses of our study include the inclusion, among HSV-2-seropositive persons, of mostly subjects with a history of genital herpes. Previous studies have shown that the majority of HSV-2-seropositive individuals have asymptomatic or unrecognised infection17; as such further studies need to be done in persons with unrecognised HSV-2 infection.2 An inherent weakness is our limited power to exclude a relationship between the APOE genotype and shedding rates, related to the size of the cohorts. However, in the genital shedding cohort, we had 80% power to detect associations of either the shedding rate or lesions rate with APOE4, as long as the magnitude of the RR was at least as high as 1.4-fold, or smaller than 0.7-fold. In the oral shedding cohort, with fewer subjects, we had 80% power to detect RR either larger than 1.9-fold or smaller than 0.6-fold. Associations of smaller magnitude cannot be ruled out by this analysis.
APOE is a reasonable ‘target gene’ candidate for HSV genotypic association research. In 1997, Itzhaki et al4 measured APOE genotypes in adult subjects with and without cold sores, and found an odds ratio (OR) of 5.7 for having any copies of APOE4 among persons with cold sores compared with persons without cold sores. A subsequent follow-up report analysed 146 adults, divided into those with and without cold sores. A similarly raised OR for APOE4 for cold sores was reported, as was a trend to the earlier onset of symptomatic oral herpes among a separate cohort of children who had the APOE4 allele.18
Subsequently, Jayasuriya et al19 studied 96 HSV-2/HIV co-infected individuals in a clinic serving predominantly African immigrants and found a significant association between the APOE4 allele and symptomatic genital ulcers. In multivariate analyses, ethnicity, CD4 cell count and anti-HIV therapy were not associated with recurrent ulceration. In contrast to Jayasuriya et al,19 we did not find any association between the APOE genotype and genital herpes history. The cohorts obviously differ with regard to immunological status. In contrast to focussing on candidate genes, Hobbs et al20 used a genome-wide scan to look for human chromosomal loci associated with symptomatic oral herpes (defined as two or more episodes per year). They found a susceptibility allele on chromosome 21 but, using a nearest marker approximately 0.8 Mb from APOE on chromosome 19, did not detect a signal from the region of APOE.
Mechanistic biological links between APOE and HSV have not been rigorously described. APOE has biological activities linked to HSV replication.21 22 Burgos and colleagues23–26 studied HSV-1 pathogenesis in mice deleted for endogenous APOE, or in which murine APOE was replaced by specific human APOE alleles. Murine APOE generally enhanced HSV infection compared with APOE deletion. Higher levels of acute and latent infection were detected in APOE4 transgenic mice, including in the brain and trigeminal ganglia, than in APOE3 mice. We observed an association between the APOE genotype and oral lesions, most of which are caused by HSV-1, but not with recurrent genital lesions, most of which are caused by HSV-2. While the genomic structures of the two viral types are similar, HSV-1 reactivates more efficiently from craniofacial ganglia and HSV-2 reactivates better from sacral ganglia. Host genetic loci could be associated with the severity of both viral types, or distinct for HSV-1 versus HSV-2. HSV-2 pathogenesis has not yet been studied in APOE-recombinant mice. HSV-1 and HSV-2-encoded proteins differ at myriad amino acid-coding loci, including loci in genes reported to interact with host immune or inflammatory molecules and cells such as glycoprotein D,27 glycoprotein B,28 the Us5, Us3 and γ34.5 gene products29 30 and ICP47.31 Spontaneous recurrences, the topic of this report, are difficult to study in murine models. This limits the potential for currently available murine models to address the mechanism for the type-specific association between the APOE genotype and the lesional recurrences that we observed.
In summary, we found that the APOE4 allele was significantly associated with a higher rate of oral lesions reported by HSV-1-seropositive study participants. Neither genital lesion rate, nor oral or genital HSV DNA detection, were correlated with the APOE genotype. Because HSV shedding is strongly correlated with transmission, it is unlikely that the APOE genotype has had a significant effect on shaping HSV dissemination in the population. It remains possible that other genetic loci in linkage disequilibrium with APOE determine oral lesion formation, or that APOE cooperates with other host genes to modulate HSV-1 or HSV-2, requiring further research in genetic host–pathogen relationships for these common infections.
Key messages
Human APOE genotypes were not associated with HSV-1 or HSV-2 mucosal shedding rates as measured by daily swabs and a sensitive PCR assay.
Human APOE genotypes were not associated with the rate of self-reported genital lesions.
The human APOE4 allele was associated with an increased rate of self-reported oral lesions.
Acknowledgments
The authors would like to thank Dr Rhoda Morrow and the University of Washington Clinical Virology Laboratory for performing HSV serology, Dr Meei-li Huang and the University of Washington Molecular Virology Laboratory for performing HSV PCR, Christopher McClurkan for overseeing DNA processing, and the staff of the Virology Research Clinic and the Westover Heights Clinics.
References
Footnotes
Funding Funding was provided by National Institutes of Health grants U19 AI031448 and PO1 AI30731.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the University of Washington and Western Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour