Article Text

Abstract
Background Few studies have estimated Chlamydia trachomatis (CT) prevalence in the general population, most prevalence studies being based on people already attending healthcare settings.
Objectives To estimate the prevalence of CT in France, assess the feasibility of home sampling without any face-to-face intervention and identify risk factors associated with CT infection using data from the Contexte de la Sexualité (CSF) survey on sexual behaviour; a national population-based survey, carried out by telephone in 2006.
Methods A random subsample of sexually experienced people aged 18–44 (N=4957) were invited to participate in a CT home-sampling study (NatChla study). Participants' samples were tested for CT by PCR. Percentages were weighted for unequal selection probabilities and post-stratified based on French population census data. Independent risk factors were identified by logistic regression.
Results CT prevalence in people aged 18–44 was estimated at 1.4% (95% CI 0.8% to 2.6%) for men, and 1.6% (95% CI 1.0% to 2.5%) for women. Increased rates were found in subjects aged 18–29: 2.5% (95% CI 1.2% to 5.0%) for men and 3.2% (95% CI 2.0% to 5.3%) for women. CT infection was associated, for both genders, with having their last sexual intercourse with a casual partner. Other risk factors were for men, having last intercourse with a new partner, living in the Paris area, and for women, multiple partners during the previous year, same sex partners and a low level of education.
Conclusions CT prevalence in France is similar to that in other developed countries. Home sampling proved feasible and useful to reach members of the population with limited access to traditional care.
- Chlamydia trachomatis
- prevalence
- population-based
- risk factors
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis (CT) infection is the most commonly reported bacterial sexually transmitted infection in industrialised countries. Most genital chlamydial infections are asymptomatic. This allows the infection to spread undetected, potentially leading to severe long-term complications in women's reproductive tracts.1 Such complications may be avoided by antibiotic treatment in the early stage of the infection.
Systematic screening may reduce complications and the transmission of CT in the population.2 However, the cost-effectiveness of a screening programme is controversial and depends mainly on the prevalence and adherence rates in the target population.3 Most prevalence studies have been based on people already attending healthcare centres, as genital samples are necessary to diagnose CT.4 The development of non-invasive self-collection sampling kits over the past 10 years has opened up opportunities for the screening of asymptomatic subjects and for the conduct of population-based surveys. Such surveys have rarely been carried out nation wide. Existing studies include surveys conducted in 2000 in Great Britain5 and Slovenia,6 in 1999–2002 in the USA7 and in 2002 in the Netherlands.8 A large national population-based survey, investigating sexual behaviour in France (Contexte de la Sexualité en France (CSF) survey), was conducted in 2006. This survey was the opportunity to carry out an epidemiological study estimating, for the first time, the prevalence of CT in the French general population and to investigate the feasibility of using a self-collection home sampling kit without requiring any face-to-face intervention. Data from the CSF survey were used to identify risk factors associated with CT infection.
Methods
Sampling design
The CSF survey, was a national random population-based survey investigating sexual behaviour, carried out by telephone between October 2005 and March 2006, using two-phase stratification sampling with unequal selection probabilities at each phase. The methodology is detailed elsewhere.9 Telephone numbers were selected randomly from the list of all non-commercial telephone numbers. Only one eligible person per selected household was randomly selected to record age stratification criteria (first-phase sample). Younger adults were given a higher probability of inclusion in the second-phase sample. The participation rate in the CSF survey was 74.6%. Overall, 12 364 men and women aged 18–69 were administered a 40 min standardised questionnaire.
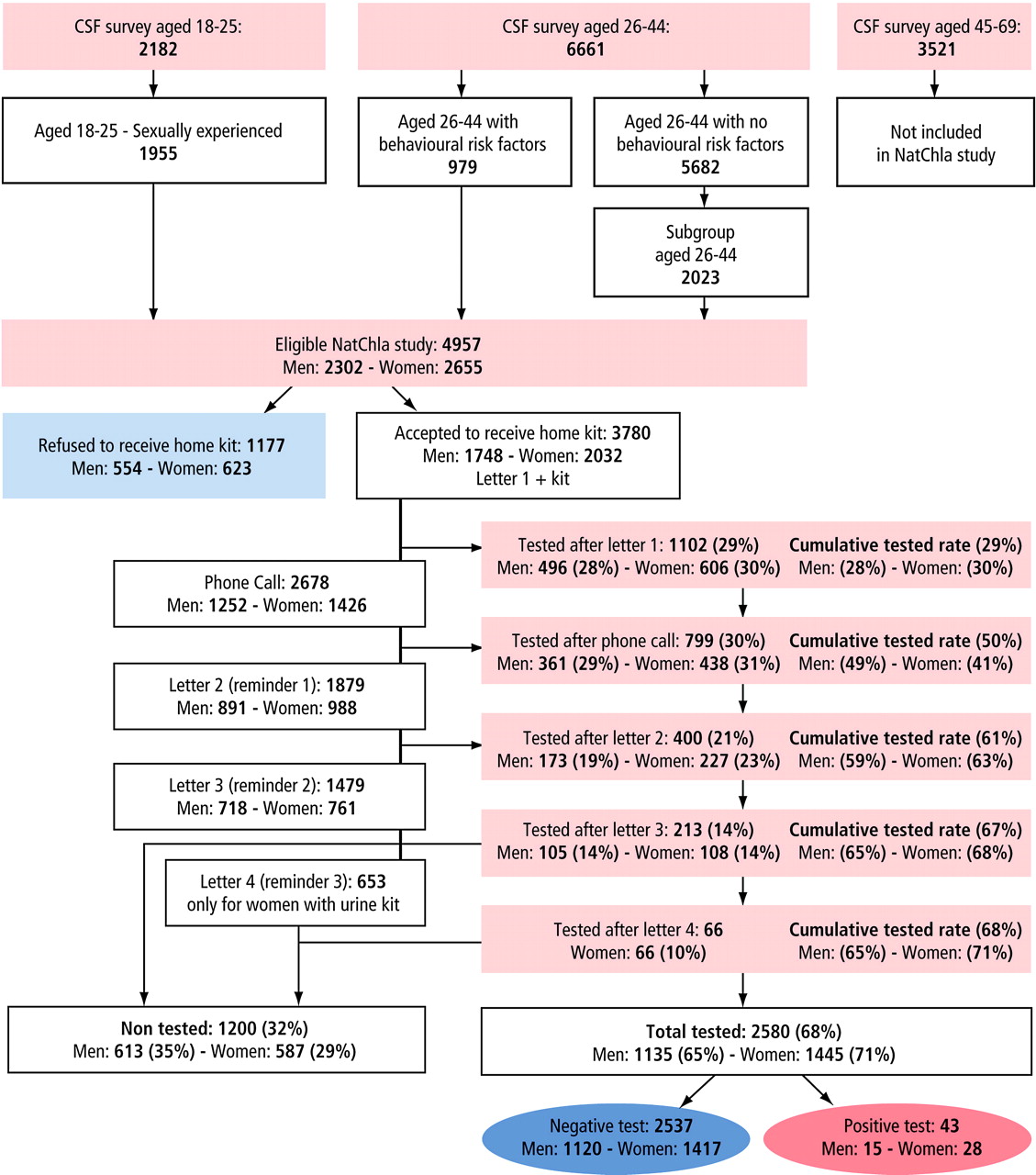
At the end of the questionnaire, a third-phase subsample was randomly selected among sexually experienced people aged between 18 and 44, using unequal inclusion probabilities according to age and risk behaviour stratification criteria: subjects aged 18–25 (n=1955), and subjects aged between 26 and 44 having had at least two sexual partners or one new partner over the past year (n=979) were all included; 2023 people were randomly selected from the remaining individuals aged between 26 and 44 (figure 1). All individuals included in that subsample (4957) were eligible to be invited to participate in a CT home-sampling programme (NatChla study).

{kind=link}
Flow chart of NatChla study.
The NatChla study
A home testing kit (urine for male and self-taken vaginal swab for women) was posted to participants. Participants then had to send their home sample by post to the Chlamydia Reference Laboratory (University Bordeaux 2). A test for CT was carried out by PCR Cobas TaqMan (Roche Diagnostics, Meylan, France). Participants who did not return the sample within 1 week were called to check that they had received the kit. Two postal reminders were sent, 10 days and 20 days after the phone call. A urine testing kit was sent to women who had not returned the swab after 1 month.
Each participant was directly informed of the results, through postal mail or by telephone from the laboratory, or by calling a free number using an anonymous code. All individuals with positive CT results were advised to undergo a medical examination, and received a letter addressed to a doctor, recommending treatment for the patient and their partners. The participation rate was defined as the proportion of the eligible population who were tested, the acceptance rate as the proportion of the eligible population who received a kit, and the tested rate as the proportion of people receiving the kit who had the test performed.
The study was approved by the French Data Protection Authority (Commission Nationale Informatiques et Libertés (CNIL)).
Statistical analysis
We calculated participation rates at each stage of selection for the NatChla study and estimated CT prevalence as a function of gender and age. Factors associated with a higher participation rate among eligible individuals, and factors associated with CT positivity among participants, were identified for each gender in univariate analyses.
The sampling design was intended to overselect individuals who lived alone (first-phase sample), who were younger and who had had multiple or new partners (second- and third-phase samples). Inverse probability-weighted estimates were used to obtain unbiased prevalences. These were also post-stratified for gender, age, level of education, marital status and region to align the distribution of the sample with the distribution of the French population census data, as was done in the previous French national survey on sexual behaviour.10
Logistic regressions were used to identify independent risk factors for participation and CT prevalence, including non-collinear factors showing a p value <0.25, in univariate analyses.
Confidence intervals, statistical tests and logistic regressions were performed according to the complex sampling design, with the svy module of the STATA software version 8.2 (StataCorps).
Analyses were conducted for the whole study population and for individuals aged between 18 and 29 years who had the highest prevalence and might be targeted by systematic screening programmes.
Results
Participation
Of the 4957 individuals eligible to participate in NatChla, 3780 (76%) agreed to receive a home testing kit. The tested rate among those who accepted the kit increased after the reminders were sent out (figure 1). The proportion of individuals tested increased from 29% to 50% after a first telephone call, to 61% after the first reminder letter, and to 67% after second reminder letter (men: 65%; women: 68%). An additional 3% of women were tested after receiving a third reminder letter with a urine sample kit, giving a final tested rate of 71% among women who accepted the kit.
In all, 2580 of the 4957 eligible individuals were tested, representing an overall participation rate of 52%, lower for men (49%) than for women (54%; p<0.0001) (table 1). The overall participation rate was independently associated with sexual orientation (higher in individuals with same sex partners) and risk behaviour at the last intercourse (higher in people who did not use a condom with a new or casual partner). These associations were stronger in women than in men (table 1). In men, the participation rate was also independently associated with age (higher for men aged >29 years). Among women, the participation rate was also associated with education level (higher in those with a higher education level).
Characteristics of participants in the NatChla survey: participation rate and factors associated with participation
Of 43 people (15 men, 28 women) with a positive CT test, information on follow-up was obtained for 38 of them (12 men; 26 women). All the men and 24/26 women had been treated adequately and 27 people (10 men; 17 women) informed their partners. Of the 27 partners informed, 22 (eight men's partner; 14 women's partner) were treated. Finally, 95% of participants to NatChla with CT infection were treated, 71% of their partners were informed and 58% treated.
CT prevalence and risk factors
The overall prevalence of CT among individuals aged between 18 and 44 was estimated at 1.4% (95% CI 0.8% to 2.6%) for men, and 1.6% (1.0% to 2.5%) for women (table 2). CT prevalence was higher for the 18–29-year age group (men: 2.5% (1.2% to 5.0%); women: 3.2% (2.0% to 5.3%), than for the 30–44-year age group (men: 0.7% (0.2% to 1.9%); women: 0.5% (0.2% to 1.1%)) (table 3).
Prevalence and risk factors associated with Chlamydia trachomatis infection in the French population for subjects aged between18 and 44 (NatChla study, Contexte de la Sexualité (CSF) survey)
Prevalence and risk factors associated with Chlamydia trachomatis infection in the French population for subjects aged between 18 and 29 (NatChla study, Contexte de la Sexualité (CSF) survey)
For both men and women, univariate analysis showed that the prevalence was higher for individuals who did not cohabit with a partner, for individuals who had had multiple partners (two or more) or a new sexual partner in the past year, and for those who had the last sexual intercourse with a casual or new partner (table 2). For men, increased prevalence was associated with living in the Paris area, not being born in France and not using a condom during their last sexual intercourse. In women, increased prevalence was associated in addition with young age, a low level of education and with having had homo–bisexual relations over the past year.
In the multivariate logistic regression analysis of men aged between 18 and 44 years, factors remaining significantly associated with CT infection were having had the last sexual intercourse with a casual or new partner, and having had several partners (two or more) in the past year. In women aged between 18 and 44 years, young age, a low level of education and a large number of sexual partners in the past year remained independently associated with CT (table 2).
When restricting the multivariate analysis to individuals younger than 30 years additional variables were associated with CT infection: for men aged between 18 and 29, living in Paris area, and for women aged between 18 and 29, having had homo–bisexual relations over the past year, and having had the most recent sexual intercourse with a casual partner (table 3).
Discussion
NatChla is the first national study estimating CT prevalence from a randomly selected sample of the French general population. The NatChla study differs from other population-based surveys in that subjects are recruited by telephone. The rate of participation in NatChla (women: 54%, men: 49%) was between the rate obtained using face-to-face contact (Great Britain National Survey of Sexual Attitudes and Lifestyles 2000 (Natsal): 71%,5 Slovenie: 83%6 or in the US National Health and Nutrition Examination Survey (NHANES): 92%7 and those obtained using methods based exclusively on posted items, including a mailed testing kit (UK Chlamydia Screening Studies (Class) project11: 38% in women and 28% in men; Danish study12: 38.6% in women and 26.8% in men; Dutch study8: 48% in women and 33% in men). Consistent with these studies, participation in NatChla was lower in men than in women.
NatChla was part of the CSF survey which aimed to investigate sexual behaviour in France. Strengths and limitations of the CSF survey were detailed by Bajos et al9 in a study comparing the CSF survey with two previous national French surveys of sexual behaviour completed in 1970 and in 1992. In the CSF survey, people not reached by phone represented around 20% of the general population. They tended to be younger, more often single and less educated than respondents. Post-stratifications were performed to limit potential bias due to factors associated with non-participation. Therefore, the subsample of people tested for CT was post-stratified according to gender, age, education level and region (see ‘Methods’). However, the NatChla study lacked statistical power to estimate prevalence precisely in small subgroups, such as men and women with homosexual or bisexual relations, giving wide confidence intervals around estimates.
The NatChla study was conducted to estimate the prevalence in sexually experienced individuals aged between 18 and 44 years from the French general population. Among them, prevalence rates were similar between men and women: 1.4% (95% CI 0.8% to 2.6%) for men and 1.6% (95% CI 1.0% to 2.5%) for women (table 2).
Comparisons with prevalence previously reported by other countries are not simple, owing to the use of different age groups to calculate rates. However, the age-specific Chlamydia prevalence was quite similar in NatChla and other national surveys in which it was estimated, with overlapping 95% confidence intervals. The prevalence in men aged between 18 and 24 years was 2.4% (95% CI 1.0% to 5.7%) in NatChla, 2.7% (1.2% to 5.8%) in the British Natsal survey5 and 4.1% (2.2% to 7.4%) in Slovenia.6 In men aged between 20 and 29 years, the prevalence was 2.9% (1.4% to 5.7%) in NatChla and 3.2% (2.4% to 3.4%) in NHANES.7 For women aged between 18 and 24 years, the prevalence was 3.6% (1.9% to 6.8%) in NatChla, 3.0% (1.7% to 5.0%) in the British Natsal survey and 4% (2.2% to 7.4%) in Slovenia. In women aged between 20 and 29 years, the prevalence was 3.2% (2.0% to 5.3%) in NatChla and 1.9% (1.0% to 3.4%) in US NHANES. As expected, the prevalence in our survey was lower than in surveys conducted in French medical settings such as STI and family planning clinics, where prevalence rates of around 8–12% have been reported for subjects between 18 and 24 years old.13
CT prevalence in our study decreased substantially in individuals older than 30 years old, for both genders, consistent with previous observations. In our study, CT prevalence in women aged 25–29 years did not differ much than the one found in women aged 18–24 years. High rates of prevalence in the 25–29 years age group is consistent with studies carried out in Belgium,14 Finland15 and the Netherlands.8 Data from the French Chlamydia Surveillance System, based on a laboratory sentinel network (Renachla), showed that 20% of cases of CT infection in women were identified in women aged between 25 and 29 years.16 In most policies, screening of asymptomatic women is recommended before the age of 25 years. The consequence of this recommendation is that older women are frequently left out by screening strategies. As prevalence in women aged 25–29 years does not differ in France from women aged 18–24 years, screening may be considered for women until the age of 29 years.
As expected, sexual behaviour—having had the most recent sexual intercourse with a new or casual partner or having had several sexual partners over the past few years—was strongly associated with risk of CT infection for both genders and for all age groups. In women aged between 18 and 29 years, having had both same and opposite sex partners in the last past year was also associated with CT infection.
The level of education was strongly associated with CT infection in women but not in men. CT prevalence was lowest in female graduates (1%), whereas it was conversely very high among women with a low level of education, particularly among women aged between 18 and 29 (12.5% (95% CI 4.1% to 32.4%)). A low prevalence rate was also reported in surveys on French university students.13 CT prevalence and education level were associated regardless of the sexual behaviour. Opportunities for asymptomatic screening are more common for women than men, mainly owing to routine gynaecological and obstetric follow-up. However, there are no official recommendations for screening asymptomatic women in France. CT tests are performed in public health settings or when they are prescribed by private gynaecologists. In private settings, patients have to pay to have the test and are reimbursed later. This may limit access to screening for women on low incomes, especially if they have no symptoms, with then a higher proportion of undiagnosed infection. Information collected during the CSF interview on previous testing by CT supports this opinion. For the question ‘Have you already been tested for Chlamydia?’, 3.3% (95% CI 2.9% to 4.9%) of women with a low education level answered yes, whereas the result was 14.5% (95% CI 12.8% to 16.3%) for those with a high education level. In men, the lack of association with educational level is probably because systematic screening is rarely proposed in the routine care setting, CT being mainly diagnosed because of symptoms. Living in the Paris area was associated with CT infection in men aged between 18 and 29 years. Surveillance data in general practice show that urethritis which acts as an indicator of STIs in men, is more common in this region. Thus, men living in the Paris area seem to have a higher risk of contracting STIs than men living in other areas.
Our NatChla survey showed that self-collection of samples at home is feasible in the French population. This method may allow high-risk subgroups to be reached more easily; indeed the participation rate observed was higher for individuals with recent risk factors of STIs. The participation rate was lower in men belonging to the youngest age group (39%) and in women with a low level of education (41%). The participation rates are still quite satisfying given that these individuals have more limited access to the traditional healthcare system and are generally more difficult to reach. The National Chlamydia Screening Programme (NCSP), implemented in England since 2003, has demonstrated that a wide variety of strategies must be used to reach this population for screening.17 Web-based methods and offering to send a test kit have been recently introduced to screen target populations in this programme and in others countries.18 19
In a previous study conducted in Sweden using an internet-based method, the authors concluded that this could be a valuable additional tool to use in opportunistic screening to reach people who do not attend healthcare facilities.20 These methods may help to reduce health costs, as kits are only sent to those who request them, and doctor intervention is limited to people who test positive.
Previous sentinel surveillance studies of sexually transmitted infections (STIs), and behavioural surveys, have shown increases in STIs21 and sexual risk behaviour in France and in other European countries.22 Estimating the prevalence of CT in the general population though the NatChla survey assists us in evaluating the number of people infected in France at the time of the study. Thus, we estimated that between 71 000 and 203 000 women and between 47 000 and 197 000 men, aged 18–29 years, were infected in France in 2006. The absence of a national screening programme in France, partly owing to a lack of evidence of cost-effectiveness and feasibility of such a programme, could cause CT infection to spread, subsequently increasing the number of cases of infertility in the population.
It is the first time that estimates of national prevalence, overall and in various subgroups, have become available to estimate costs and sensitivities of different screening strategies in general population. Systematic screening in STI clinics and in HIV testing sites is the strategy currently supported by the French government. The next step will be to promote screening in other high-risk subpopulations who do not attend such settings. Further studies, including economic assessments, are necessary to evaluate various approaches, such as the internet-based invitations, to reach these high-risk subpopulations.
Key messages
Prevalence of C trachomatis (CT) infection in the general population in France is similar to that in other European countries.
The highest rates are reported in people aged 18–29 years, or those having had multiple or new partners in the past year.
Women with a low educational level are at higher risk of undiagnosed CT infection.
Home sampling is well accepted by the French population and useful for reaching members of the population with limited access to traditional healthcare.
Acknowledgments
We thank interviewers of the CSF survey for their contribution to this substudy and for achieving a good acceptance rate to the NatChla study. We thank Hélène Haguy who sent the kits, Catherine Sale who was in charge of the follow-up of the participation to the test and Danièle David who organised the pilot study. We also thank members of the scientific committee of NatChla who are not authors of this paper for their advice: Annie Velter, Judith Cytrynowicz.
CSF group Nathalie Bajos and M Bozon (principal investigators), N Beltzer (coordinator), A Andro, M Ferrand, V Goulet, A Laporte, Ch Le Van, H Leridon, Sh Levinson, N Razafindratsima, L Toulemon, J Warszawski
References
Footnotes
Funding The NatChla survey was funded by the Agence Nationale de Recherche sur le Sida et les hépatites (ANRS) and the French Institute for Public Health Surveillance (Institut de veille sanitaire – InVS). The Institut de veille sanitaire is funded by the French Ministry of Health. The National Reference Centre is funded by a grant from the Institut de veille sanitaire.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the CNIL (Commision Nationale Informatiques et Libertés).
Provenance and peer review Not commissioned; externally peer reviewed.