Article Text

Abstract
Objective To explore the risk factors underlying congenital syphilis (CS) and to build a hazards model to assess the risk of CS in offspring born to mothers with syphilis treated in gestation.
Methods This prospective study observed 554 pregnant women with syphilis and their offspring recruited from August 2002 to May 2007 in Shenzhen Centre for Chronic Disease Control and Prevention. After treatment, all the women were followed up until the diagnosis of CS in their offspring was confirmed or denied. Comparisons were made between women bearing infants with CS and women bearing infants without CS to reveal the risk factors for CS. ORs and their 95% CI were calculated for each risk factor by using logistical regression analysis.
Results Twenty-nine (5.2%) infants were diagnosed with CS. Univariable analyses showed that the reciprocal logarithm of the titre of non-treponemal antibodies in mothers (log (1/T); OR=11.18, p<0.001), gestational week (GW) at treatment (OR=1.10, p<0.001) and the interaction between these two variates (OR=1.09, p<0.001) was associated with CS. Multivariable analysis showed that only the interaction was significantly associated with CS (OR=1.09, p=0.047).
Conclusions The risk of CS could be predicted by the interaction between GW×log (1/T). Early treatment given to women with syphilis during antenatal care may be the only effective method to decrease the risk of CS.
- Congenital syphilis
- risk model
- maternal syphilis
- treatment
- prospective cohort study
- risk factors
- syphilis
Statistics from Altmetric.com
Introduction
Congenital syphilis (CS), a disease transmitted from mother to child by Treponema pallidum, can bring about systemic functional damage to fetuses and also spontaneous abortion and perinatal death.1 2 Screening and treatment for syphilis during antenatal care has been recommended as the minimum clinical package for preventing CS and this measure has been routinely implemented in many countries.3 Although the incidence of CS has been successfully reduced, this infectious disorder is still a large burden to society. In China, the incidence of CS has increased at a worrying rate of 71.9% per year from 0.01 to 19.68 cases per 100 000 live births from 1997 to 2005.4 It is estimated that over 500 thousand fetuses died owing to maternal syphilis in the area of sub-Saharan Africa.3
Currently, it is unclear why CS cannot be effectively treated.5 6 Previous studies that explored the risk factors of CS failed to reach agreement.7–17 Suspected factors reported previously include a higher titre of non-treponemal antibodies in mothers8 11 12 and a delay or lack of prenatal care,9 10 13 14 although the validity of these results was weak because of uncertainty in the diagnosis of CS.9–14 Other reported potential risk factors include low maternal socioeconomic status,7–9 multiple/unstable sexual partners7 8 and maternal cocaine use.10 These factors were, however, considered to be directly associated with the infection status of syphilis in mothers and not associated with the infection of CS in fetuses.7 18
By this prospective study, we explored the risk factors of CS in infants born to mothers with syphilis treated during pregnancy. In addition, we tried to develop a risk model to predict CS, which could supply helpful information to both clinical doctors and infected mothers.
Methods
The population in this prospective study comprised pregnant women diagnosed with syphilis for which they and their offspring were treated. The women were indentified by an antenatal screening programme conducted from August 2002 to May 2007 at the Shenzhen Centre for Chronic Disease Control and Prevention (SCCDC).18 19 The diagnosis of maternal syphilis was based on a non-treponemal serological test (toluidine red unheated serum test (TRUST); Shanghai Rongsheng Biotech, Shanghai, China) and a treponemal serological test (Treponema pallidum particle agglutination (TPPA)).18 19 The inclusion criteria were (a) maternal syphilis was untreated before gestation; (b) women were treated by three injections of 2.4 million units of benzathine penicillin G at a weekly interval during gestation; (c) women continued their pregnancy after treatment; (d) a live birth; (e) women consented to participate in the study. All the gravidas were followed every month in pregnancy and the titre tested by TRUST and their sex partners were invited to be tested, and treated if necessary. This study was approved by the research ethics review committee of SCCDC.
A standardised questionnaire was used to assess demographic characteristics of the recruited women, including age, resident status, education, vocation, times of pregnancies, extramarital sexual relations18 19 and the presence of other sexually transmitted diseases, including, gonorrhoea, non-gonococcal cervicitis, herpes genitalis and chancroid in the past 2 years. Adverse pregnancy outcomes, including spontaneous abortion, premature delivery, fetal death or stillbirth, were determined for all previous pregnancies. The gestational week (GW) at treatment for maternal syphilis was recorded. Maternal syphilis was categorised as early syphilis (<2 years) and late syphilis (≥2 years or syphilis of unknown duration). To maintain a normal distribution, the titre of maternal TRUST at treatment was transformed using the log of the reciprocal non-treponemal titre in the mother (log (1/T)). HIV antibodies were routinely detected at screening. In this study, we used TRUST instead of rapid plasma reagin to test non-treponemal antibodies in mothers. TRUST is used widely in China and is considered to have higher stability during storage and transport.18–20
All children were examined by a fluorescent treponemal antibody absorption test with a fluorochrome-labelled anti-human IgM on fractionated sera (FTA-ABS 19S IgM test). A positive IgM test showed the presence of CS. Offspring with a negative IgM test were followed up by serological tests until the 18th month after birth if they were considered as possible CS according to the Center for Diseases Control and Prevention (CDC) guidelines.1 A positive result with TPPA at the 18th month after birth was used as a retrospective validation of the diagnosis of CS.1 All cases with CS or presumptive CS were given an intramuscular injection of benzathine penicillin G 50 000 units/kg according to the CDC guidelines.1 Data of sociodemographic characteristics, obstetric history and results of the follow-up were collected by specially trained nurses. All serological test results for syphilis (TRUST, TPPA, and FAT-ABS 19S IgM) were read by two experienced technicians.
Comparisons were made between women bearing normal infants and those bearing infants with CS. The categorical variable was described by number and percentage and the continuous variables by mean±SE. χ2 Analysis was used to test for proportions and the t test was used for means. Univariate and multivariate logistic regression analyses were used to show the association between CS and the variables observed. Odds ratios (ORs) and their 95% CI were used to show the level of the association. Curve estimation was used to define the regression risk model for CS in which the dependent variable is the percentage of CS in infants and the independent variable is the specific value (or interval) of potential risk factors. The curve with the highest coefficient of determination (R2) was determined to be the most appropriate model. We used a type 1 error level of 0.05. All statistical analyses were performed using SPSS 10.0.
Results
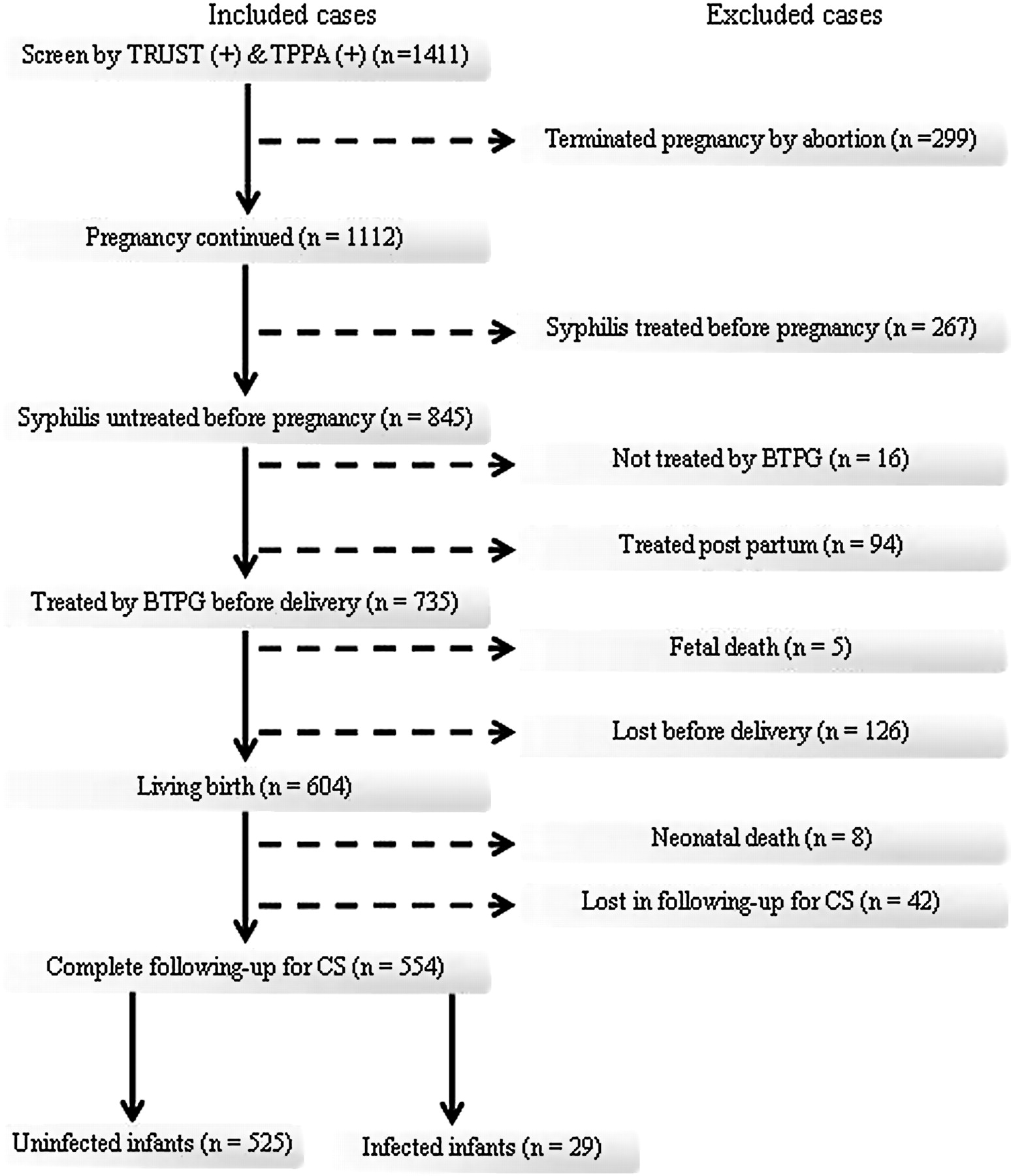
During the 5-year study period, we screened 825 443 gravidas and identified 3579 (0.43%) women with syphilis. Of these, 1411 pregnant women were interviewed at the SCCDC (figure 1). Two hundred and ninety nine pregnancies (21.2%) were aborted spontaneously (21 cases) or were induced (278 cases). Of the 1112 remaining, 845 had not been previously treated for syphilis. Of these, 16 (1.9%) cases were treated by azithromycin or other antibiotics but not penicillin. Ninety-four (11.12%) cases were diagnosed with syphilis at delivery and treated post partum. Thirteen deaths (1.5%) were reported, including five fetal deaths and eight neonatal deaths. One hundred and sixty-eight (19.9%) cases were lost to follow-up. Finally, 554 gravidas were included for analyses. At the end of follow-up, 29 (5.2%) infants were diagnosed with CS. Twenty-two infants were positively examined by FTA-ABS 19S IgM test and the other seven were retrospectively diagnosed by a reactive TPPA test 18 months after birth.

Flow chart for selecting mothers infected with syphilis. BTPG, benzathine penicillin G; CS, congenital syphilis; TPPA, Treponema pallidum particle agglutination; TRUST, toluidine red unheated serum test.
The mean age of the women was 27.7±0.2 (range 18–43) years, and the mean gestational age at treatment for syphilis was 22.2±0.4 (range 4–43) weeks. Most women (93.1%) in the cohort were married and 88.3% were temporary residents (table 1). About half of them were educated at the level of high school or above. More than 90% of these gravidas had no history of sexually transmitted diseases other than syphilis, although 50% of them acknowledged having a history of extramarital sexual relations. Eighty-two per cent of the mothers had no history of adverse pregnancy outcomes. Only three cases (0.5%) were diagnosed with primary syphilis and five (0.9%) were at the secondary stage. Five hundred and forty-three cases (98.1%) had no symptom of syphilis and 90% were late latent or did not know the duration of their syphilis. There was no significant difference in the demographic characteristics and obstetrics between the mothers having normal infants and those having infants with CS (table 1).
Characteristics of the gravidas with untreated syphilis recruited in Shenzhen from 2002 to 2007
Although most (69%) infants with CS were born to mothers with late syphilis, infants were at higher risk (p=0.001) of infection if the mothers were at the early stage of syphilis at treatment (table 1). Most infants with CS were born to mothers with higher titres (≥1:8) of non-treponemal antibodies (p<0.001). Four cases of CS were detected where the mothers' titre was l<1:8. For the group of mothers having CS infants, the treatment for syphilis was given 10 weeks later (p<0.001) than those having normal infants. No positive result was seen when antibodies to HIV were tested in all the mothers.
Univariable analysis showed that women with early syphilis had a five times (OR=5.01, 95% CI 2.15 to 11.69) higher risk of delivering a child with CS than women with late syphilis (p<0.001) (table 2). Mothers with a higher titre in the TRUST test were at a higher risk of transmitting the infection to their offspring than those with a lower titre (OR=11.18, 95% CI 5.16 to 24.24, p<0.001). Every week of delay in treatment to maternal syphilis increased the risk of infants becoming infected by 10% (OR=1.10, 95% CI 1.06 to 1.15, p<0.001). When interactions were examined, CS was associated with the interaction GW×log (1/T) (OR=1.09, 95% CI 1.06 to 1.11, p<0.001). The other variables did not change the risk of CS substantially (table 2).
Univariable logistic analyses of the risk factors for congenital syphilis
After correction for the stage of maternal syphilis, in multivariable analyses, the interaction between GW and log (1/T) remained significant in association with CS (OR=1.09, 95% CI 1.00 to 1.19, p=0.047) (table 3). The percentage of CS in infants was positive against an increasing product of GW×log (1/T). The stage of maternal syphilis, GW for treatment and log (1/T) were not associated with CS in the multivariable analysis (table 3).
Multivariable logistic analyses of the risk factors for congenital syphilis
Curve estimations for the percentage of CS in infants showed the TRUST titre (R2=0.95, p=0.006), gestational month at treatment (R2=0.98, p<0.001) fitted best using cubic equations. Consistent with the previous analyses, the model reached the highest coefficient of determination (R2=0.99, p=0.003) when only the interaction of GW×log (1/T) was included. The parameter estimates are listed in table 4. Figure 2 shows the curves of these three equations and the ratios of CS in infants. According to the best fitting model (figure 2C), no CS was seen if the product of GW×log (1/T) was ≤5. More than 98% of the mothers with a product <25 had normal infants, whereas the percentage of CS in infants increased sharply from 11% to 66% when the product was >25.
Curve estimations by cubic equations for the percentage of CS

{kind=link}
{kind=link}
Curve estimations for proportions of congenital syphilis in infants born to mothers with syphilis treatment in gestation by (A) the titre of maternal non-treponemal antibodies, (B) gestational month at treatment for maternal syphilis and (C) the interaction between gestational week and the reciprocal logarithm of maternal non-treponemal antibody titres (here the values of 5, 15, 25, 35, 45, 55 and 65 were used to represent the intervals of the independent variable). Log (1/T) is a reciprocal logarithm calculation of the TRUST titre in the mother. The numerators indicate the cases of CS and the denominators indicate the population of infants. CS, congenital syphilis; TRUST, toluidine red unheated serum test.
Discussion
CS has been a global burden and elimination of CS is one of the millennium development goals of the World Health Organization.21 The identification of risk factors of CS is important for the prevention of this infectious disease. In this study, for the first time, we quantified the effect of the titre of non-treponemal antibodies in mothers and late treatment in pregnancy on the incidence of CS. Our findings showed an association between the interaction of GW×log (1/T) and CS.
Strengths and weaknesses
Currently, it is difficult to diagnose CS because of the transplacental transfer of non-treponemal/treponemal IgG antibodies and asymptomatic or non-specific presentation of CS.1 22 23 Previous articles reported that a higher titre of non-treponemal antibodies in mothers was a risk factor for CS.8 11 12 These studies analysed presumptive cases according to the CDC guidelines24 rather than definite cases, which would increase the proportion of cases and weaken the association relationship. In addition, the titres of non-treponemal antibodies were previously analysed as a high (≥1:8) or low titre (<1:8). This dichotomous method would omit much information since the mother's infection is the direct cause of CS. In this study, we have shown how maternal antibody titres, as a continuous variable after transformation, alter the infection risk to their infants.
A delay or lack of prenatal care was formerly a reported association with CS.9 10 13 14 However, previous studies did not give a quantitative description. Alexander et al15 reported that maternal treatment was uniformly successful at all gestational ages based on a cohort of 340 gravidas. According to the results of our univariable logistic analysis, every week's delay in treatment would increase the risk by about 10%. More research is needed to clarify which results are more accurate. However, our results seemed consistent with the conventional understanding—namely, that the greater the exposure, the greater the risk of infection. It is well known that treatment given after 28 weeks' gestation may not be effective in preventing CS.15 The unusual finding in this study is that, as shown in figure 2B, five infants whose mothers had been treated before 28 weeks' gestation were infected. After re-inspecting the medical records, we found none of these cases had evidence for re-infection in the mothers. The antibody titres in these mothers were 1:2, 1:4, 1:8 (in two) and 1:32 and they stayed the same during pregnancy. So, failing to cure maternal syphilis would be a serious risk factor for CS.
In this study the main method for the diagnosis of CS was FTA-ABS 19S IgM, which had 100% specificity and 73% sensitivity.25 To avoid loss of the false-negative cases detected by the IgM test, we followed up the presumptive cases by TPPA test until the 18th month after birth for the ultimate diagnosis.1 This method of diagnosis for CS avoids confounding from presumptive cases and increases the sensitivity for finding risk factors. After effective treatment for syphilis in pregnancy, infection in the fetuses became uncommon.15 It therefore took 5 years to identify 29 cases of CS in our study. The small number of CS cases was a limitation for this study and the results will therefore need to be confirmed in other samples before clinical application of these risk models. Another limitation was that stillbirth and abortion were not included, which might weaken the association as CS is an important cause of fetal death.
Meaning of the study
It is difficult to analyse and predict the risk of CS with two independent variables. The finding of an interaction between log (1/T) and GW at treatment simplified the model. The curve estimate provides a simple visual model. If this model is proved, the clinical risk evaluation for CS could be conducted easily and CS could be prevented successfully.
Future research
Investigators should consider diagnosis methods for CS such as biopsy and PCR using infantile tissues in future studies in order to increase the accuracy of the diagnosis for CS. Meanwhile, every dead infant, stillbirth and abortion should be assessed for CS to avoid missing any case. Collaborations between clinical centres and prevention institutions are necessary in order to collect sufficient cases for analysis.
Key messages
Delayed treatment for maternal syphilis affects the risk of congenital syphilis (CS) in infants.
The titre of maternal non-treponemal antibodies has an impact on the risk of CS.
The risk of CS can be predicted by the interaction between the gestational week and log (reciprocal of maternal titre of non-treponemal antibodies) at treatment.
Acknowledgments
We thank all patients for participation in this study.
References
Footnotes
Funding This work was supported by the Programme of Prevention of mother-to-children transmission of Syphilis in Shenzhen (the PPSS) and grant B2006143 from the Fund for Studies on Medical Science and Technology in Guangdong Province.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the research ethics review committee of Shenzhen Centre for Chronic Disease Control and Prevention.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Whistlestop tour