Article Text

Abstract
Objective To perform a European sentinel surveillance study for antimicrobial resistance (AMR) in Neisseria gonorrhoeae as part of the European Surveillance of Sexually Transmitted Infections Programme.
Methods From 2006 to 2008 17 countries participated in the AMR surveillance programme. The susceptibility of a total of 3528 consecutive isolates was tested using the agar dilution breakpoint technique or Etests for ciprofloxacin, penicillin, tetracycline, azithromycin, spectinomycin and ceftriaxone. Nitrocefin was used to detect β-lactamase activity.
Results Rates of resistance to ciprofloxacin, the previously recommended treatment, were high across Europe (42–52%), indicating that usage is no longer appropriate. Although resistance to the currently recommended treatment, ceftriaxone, was not demonstrated, a concerning upward drift in the minimal inhibitory concentration (MIC) distribution was identified since an earlier European study in 2004. No resistance to spectinomycin was seen, whereas azithromycin resistance varied from 2% to 7% and isolates from Scotland (n=4) and Ireland (n=1) showed high-level resistance (MIC >256 mg/l). High-level resistance to tetracycline and penicillin remained relatively constant at 16% and 12%, respectively.
Conclusions AMR is an ongoing problem in Europe, with high rates of resistance to many previously recommended therapeutic agents observed in many European countries. Continual European and global surveillance of AMR in N gonorrhoeae is essential to monitor for increasing, emerging and high-level resistance to therapeutically relevant agents and to inform treatment guidelines so optimum treatments are administered.
- Neisseria gonorrhoeae
- Gonorrhoea
- antimicrobial resistance
- surveillance
Statistics from Altmetric.com
Introduction
Neisseria gonorrhoeae is the causative agent of gonorrhoea, a sexually transmitted infection (STI) which continues to present a significant public health problem across Europe and world wide, with approximately 62 million new cases diagnosed globally each year.1 Gonorrhoea primarily presents as a mucosal infection of the lower genital tract, which is predominantly symptomatic in men presenting as urethritis but is thought to be asymptomatic in about 50% of women. N gonorrhoeae can ascend to the upper genital tract, if undiagnosed or inadequately treated, leading to complications such as infertility, which occur more frequently in women, or can invade the blood causing disseminated infections (eg, septic arthritis, meningitis, endocarditis). Gonorrhoea is associated with an increase in the acquisition and transmission of HIV.2 Treatment of gonorrhoea, therefore, is essential for individual patient management and also to intercept transmission chains and so reduce the overall disease burden. However, successful treatment of gonorrhoea is severely compromised by the propensity of N gonorrhoeae to develop resistance to antimicrobial agents used for treatment, and the subsequent worldwide spread of resistant gonococci is well documented.3–8 Therefore, surveillance of antimicrobial resistance (AMR) for N gonorrhoeae is of paramount importance to inform prescribing policy to ensure that patients receive appropriate treatment.
The European Surveillance of Sexually Transmitted Infections (ESSTI) project was established in 2002 to develop and coordinate epidemiological and laboratory surveillance of STIs in the European region in order to better inform about STI prevention, care and control. Surveillance data collected by ESSTI demonstrated that the number of cases of gonorrhoea, from 1998 to 2007, rose in Western Europe, remained steady in Central Europe and declined in the two Eastern European countries that supplied data.9 However there was wide variation in the rate of gonorrhoea diagnoses in individual countries—for example, 0.3/100 000 in Italy to 30.8/100 000 in the UK in 2007,9 although this may be due to heterogeneity in the different surveillance and laboratory systems.9
Euro-GASP (European Gonococcal Antimicrobial Surveillance Programme), the laboratory component of ESSTI, performed the first European sentinel surveillance study for AMR in N gonorrhoeae in 2004.10 This initial study disclosed high resistance rates to ciprofloxacin (31%), which was used by most countries for treatment at that time, and tetracycline (60%) and penicillin (21%), together with azithromycin resistance of >5% was observed for the first time. Surveillance studies are essential to demonstrate when resistance rates to antimicrobial agents exceed 5%, the level at which a therapeutic agent should no longer be recommended as first-line treatment.11 In addition, it is of particular importance to monitor emerging resistance to the currently recommended treatment across Europe, the third-generation cephalosporins.12
Euro-GASP has subsequently performed sentinel surveillance studies in 2006 to 2008 to continue to monitor the prevalence of antimicrobial-resistant N gonorrhoeae across Europe.
Methods
Participating laboratories
Seventeen N gonorrhoeae reference or specialist laboratories participated in the ESSTI N gonorrhoeae AMR surveillance study, as previously described.9 Three participating laboratories had complete coverage of all diagnosed gonorrhoea in the country (Denmark, Scotland and Sweden). Eight laboratories had good national coverage, defined as representations from all areas of the country but not every case of diagnosed gonorrhoea (Belgium, England and Wales, France, Greece, Latvia, Malta, Portugal and Spain). Six laboratories had good coverage of a particular region of the country but not national coverage (Austria, Germany, Ireland, Italy, The Netherlands and Slovenia).
Collection of N gonorrhoeae isolates
The aim of the isolate collection was to obtain a minimum of 1000 isolates across Europe, where possible, to maximise the ability to detect changes over time. Each country was asked to contribute 100 isolates from 1 June each year. Some laboratories (Austria, Portugal, Slovenia, Germany, Greece, Malta, Italy and Latvia) collected isolates before the start date owing to a low collection rate. Laboratories were requested to collect one isolate from each patient.
Pure cultures, 18–24 h old, were saved on Microbank beads (Pro-lab Diagnostics, Richmond Hill, Canada) and stored at −70°C. The isolates were then sent frozen on dry ice to one of three laboratories for susceptibility testing (Health Protection Agency, London, UK; Statens Serum Institut, Copenhagen, Denmark and Outpatients' Centre for Diagnosis of Infectious Venero-Dermatological Diseases, Vienna, Austria).
For each isolate the following data, where available, were collected: date specimen obtained, sex and age.
Antimicrobial susceptibility testing
Isolates were retrieved on GC agar (Becton, Dickinson and Co, Le Pont de Claix, France) with 1% Vitox (Oxoid, Basingstoke, UK) and incubated for 18–24 h at 36°C in 5% CO2. Isolates were confirmed to be N gonorrhoeae by Gram stain, oxidase test and either the Gonogen II test (Bioconnections, Leeds, UK) or the Microtrak test (Trinity Biotech, Wicklow, Ireland), according to the manufacturer's instructions. Susceptibility testing was performed at the three centres using the agar dilution breakpoint technique for ciprofloxacin, azithromycin, penicillin and tetracycline. In addition, spectinomycin was tested for the 2008 isolates.
The isolates were subcultured once before susceptibility testing was performed. Suspensions of cultures aged 18–24 h were prepared equivalent to McFarland's standard 0.5 (approximately 104 cfu/μl) in saline. Using the Multipointelite multipoint inoculator (Mast Group Ltd, Bootle, UK), suspensions were inoculated onto GC agar plates with 1% Vitox, containing a panel of antimicrobial agents at the following breakpoint concentrations: penicillin (1 mg/l), ciprofloxacin (0.5 mg/l), tetracycline (1 and 8 mg/l), azithromycin (0.5 mg/l) and spectinomycin (64 mg/l). Plates were incubated for 18–24 h at 36°C in 5% CO2 and the presence of bacterial growth was recorded for each isolate. All isolates were tested for penicillinase production using the chromogenic reagent, nitrocefin (Oxoid), following the manufacturer's instructions. The ceftriaxone minimal inhibitory concentration (MIC) of isolates was determined using Etests (AB bioMérieux, Solna, Sweden), according to the manufacturer's instructions. Azithromycin MICs were determined by Etest for isolates displaying resistance by the agar dilution breakpoint technique.
The Clinical and Laboratory Standards Institute breakpoints for susceptibility or resistance,13 as widely used in European countries, were used for ciprofloxacin, penicillin, tetracycline and spectinomycin. The European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints14 were followed for azithromycin and ceftriaxone, as Clinical and Laboratory Standards Institute have not yet recommended a breakpoint for azithromycin and the lower EUCAST breakpoints for ceftriaxone ensure that levels of decreased susceptibility are not underestimated. In summary, strains were categorised according to the following definitions: ciprofloxacin resistant (MICs ≥ 1 mg/l); penicillinase producing N gonorrhoeae (PPNG) (β-lactamase positive); tetracycline resistant N gonorrhoeae (TRNG) (MICs ≥16 mg/l); chromosomally resistant N gonorrhoeae (CMRNG) (penicillin MICs≥2 mg/l and β-lactamase negative and tetracycline MICs 2–8 mg/l); azithromycin resistant (MICs ≥1 mg/l); spectinomycin resistant (MICs≥128 mg/l) and ceftriaxone decreased susceptibility (MICs>0.125 mg/l).
Statistical analysis
Fisher's exact test was used to assess the significance of difference between the resistance rates from 2006 to 2008. The significance of difference between all countries and countries that participated in all of the 3 years was assessed using Fisher's exact test. The differences between the resistance rates of each antimicrobial agent between all participating countries in each year was assessed using the χ2 test for penicillin, tetracycline and ciprofloxacin, and Fisher's exact test for azithromycin and fully susceptible strains. p Values <0.05 were categorised as significant.
Quality assurance and control
Laboratory personnel from each of the three testing centres were trained at a single centre (the Health Protection Agency) to ensure consistency of technique. Quality control strains (WHO A (spectinomycin resistant), WHO G (penicillin and tetracycline resistant), WHO J (PPNG, ciprofloxacin and tetracycline resistant), and G06-1153 (azithromycin resistant clinical strain) were included in each susceptibility testing run. To ensure consistent quality assurance, two different panels of 10 strains were tested by the three centres each year using all methods and the results from all three centres were compared.
Results
Isolate and patient data
A total of 3645 isolates were collected over the 3-year period (table 1) and after removal of duplicate specimens, 3528 isolates were retrieved and confirmed to be N gonorrhoeae. The overall retrieval rate was 97% (3528/3645). The number of isolates tested from each country varied from 12 (Germany 2008) to 114 (Spain 2006) (table 2). Of the 3528 isolates tested, further data were available for 3494 isolates. The majority of gonococci (80%; 2798/3494) were collected from men whereas 19% (675/3494) were from women. Gender was unknown for the remaining 21 isolates (table 1). The age range of the patients was 6 to 81 years, with a mode and median age of 24 and 31 years, respectively.
Isolate and patient characteristics
Resistance rates by ciprofloxacin and azithromycin antimicrobial agents and percentage of strains that were fully susceptible in each participating country
Antimicrobial susceptibility
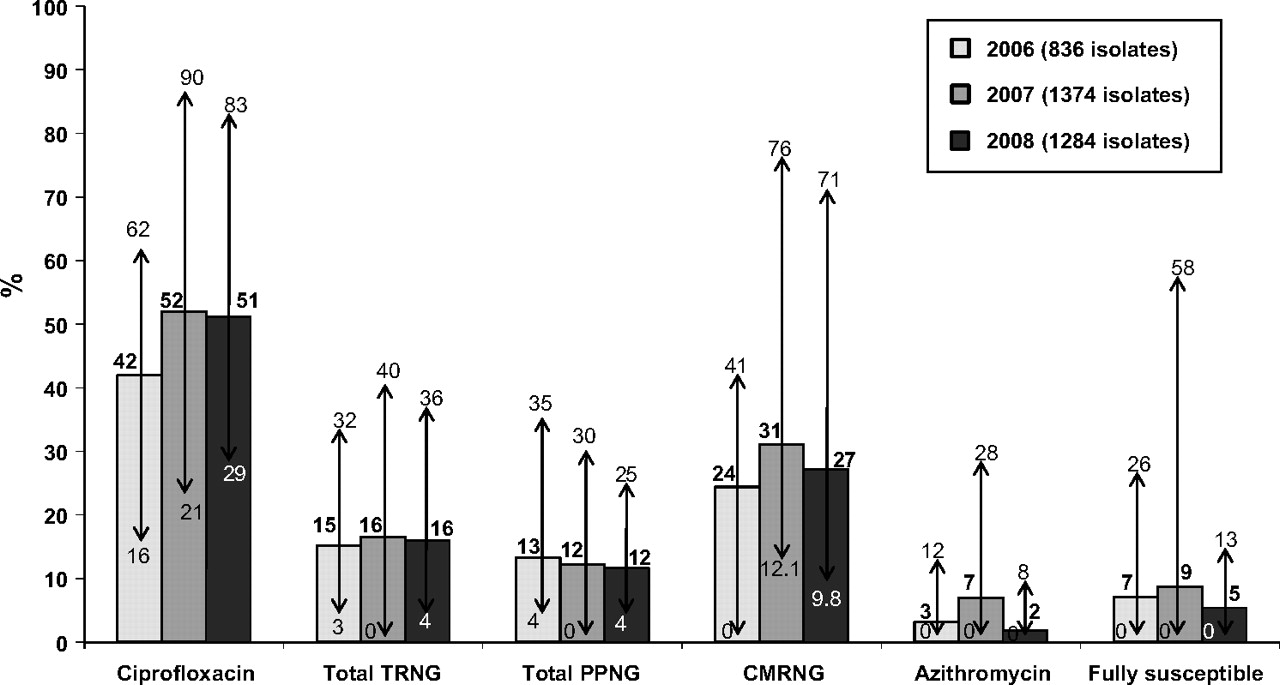
Data from all countries for each year were combined to determine the overall resistance rates (figure 1). The list of participating countries varied slightly for each year (table 2). However, there were small, non-significant differences (Fisher's exact test p>0.05) when the resistance rates from the countries that participated in all 3 years were compared with all countries in each of the 3 years (table 2 and online supplementary table 3). For each antimicrobial agent in each year there was considerable variation in the resistance rates between the countries (χ2 and Fisher's exact test p≤0.01) (table 2 and online supplementary table 3).
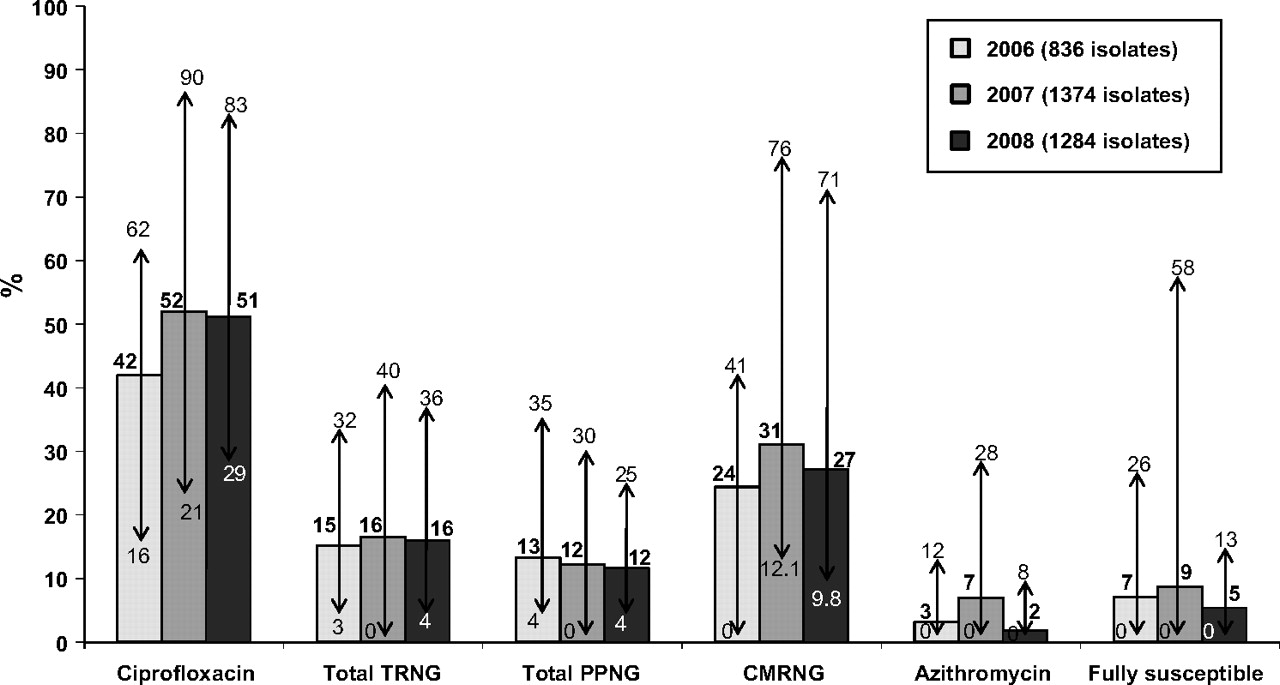
Overall incidence of resistant and fully susceptible N gonorrhoeae (arrows indicate the lowest and highest percentage from participating countries (see table 2 and online supplementary table 3). CMRNG, chromosomally resistant N gonorrhoeae; PPNG, penicillinase producing N gonorrhoeae; TRNG, tetracycline resistant N gonorrhoeae.
The overall level of ciprofloxacin resistance significantly increased from 42% in 2006 to 51% in 2008 (Fisher's exact test p<0.001). All countries displayed more than 5% resistance to ciprofloxacin in each year tested (table 2). No apparent trend for azithromycin resistance rates was evident (table 2). The modal MIC of azithromycin resistant isolates in all 3 years was 1.0 mg/l. Four isolates in 2007 from Scotland and one from Ireland in 2008 were highly resistant to azithromycin (>256 mg/l). High-level resistance to penicillin (PPNG) and tetracycline (TRNG) remained fairly constant over the study period (online supplementary table 3) and there was no apparent trend from 2006 to 2008 for chromosomally mediated resistance to both penicillin and tetracycline (CMRNG).
No isolates demonstrated decreased susceptibility to ceftriaxone. The modal MIC of isolates to ceftriaxone was 0.008 mg/l in 2006 and 2007 and 0.004 mg/l in 2008 (figure 2).

{kind=link}
{kind=link}
Ceftriaxone minimal inhibitory concentration (MIC) distribution.
Quality assurance
The overall concordance for the agar dilution breakpoint technique was 94% (94/100). For the agar dilution technique the same category of resistance was not achieved on six occasions—for penicillin (n=4), ciprofloxacin (n=1) and azithromycin (n=1) for each quality assurance isolate. However, all these six strains had an MIC on a breakpoint. There was 100% concordance for 10 strains tested by azithromycin Etest. Eighty-five per cent (17/20) concordance was achieved for the 20 strains tested by ceftriaxone Etest, where the MICs differed by less than two doubling dilutions. The internal quality control strains results were within one dilution of the expected ranges.
Discussion
This study provides the first longitudinal study of data on antimicrobial resistance in gonococci across Europe to inform European treatment guidelines, building on the original surveillance study conducted in 2004.10 High levels of resistance to ciprofloxacin, the preferred treatment until recent years, and a drift in modal MIC to ceftriaxone, the currently recommended treatment in most countries, has been detected by this surveillance programme.
Ciprofloxacin resistance has increased dramatically since the first European N gonorrhoeae AMR sentinel study was performed in 200410 (31% to 51% in 2008) despite the fact that ciprofloxacin is no longer recommended for treatment in Europe.12 The rates are above the recommended 5% cut-off point11 in all participating countries. Similarly high rates have been demonstrated in individual European countries conducting national surveillance of antimicrobial resistance.6 15–21 It is evident that ciprofloxacin resistance in N gonorrhoeae confers no selective disadvantage to the organism as resistance has persisted in countries where relatively little ciprofloxacin is now prescribed for treatment of gonorrhoea.6 This high level of ciprofloxacin resistance clearly indicates that this antimicrobial agent is not an appropriate choice for use in any of the countries which participated in this study, unless isolates are known to be susceptible or local resistance rates are known to be <5%.
It was encouraging to note that there were no examples of decreased susceptibility to ceftriaxone over the sampling period, and there was also little change in the ceftriaxone modal MICs from 2006 to 2008. However, the observation that the modal MICs of ≤0.002 mg/l documented in 200410 had increased to 0.008 mg/l in 2006 and 2007, and 0.004 mg/l in 2008 may indicate drift in the susceptibility of the gonococcal population in Europe. It should be noted that ceftriaxone MICs were determined by agar dilution in the 2004 study10 and by Etest in this study. Although these two methods have been shown to be comparable in our laboratory (data not shown), the possibility that differences in modal MIC are partially due to differences in methodologies cannot be fully excluded. However, a similar drift in the population susceptibility to ceftriaxone has been documented recently in England and Wales,6 and this study may indicate an emerging problem across Europe, which raises the possibility that MICs may reach a level which leads to treatment failure. The data from this study show that ceftriaxone is still an appropriate treatment for gonorrhoea in Europe, and as yet, treatment failure of urogenital gonorrhoea has not been documented, although treatment failure for pharyngeal infection has been recorded.22 Ceftriaxone is administered parenterally and this has the advantage of ensuring patient compliance and preventing misuse of the agent, which may delay emerging resistance. In contrast, third-generation cephalosporins administered orally, such as cefixime, have already resulted in suspected treatment failures23 24 This study did not examine resistance to cefixime, but a review of the susceptibility testing panel for European surveillance of gonococcal antimicrobial resistance in 2009 has led to the amendment of the testing strategy to include cefixime to ensure that all therapeutically relevant agents are monitored in future years.
The threat of emerging resistance to third-generation cephalosporins highlights the need to consider future therapeutic options. Azithromycin is not currently a recommended treatment for gonorrhoea12 but it is proposed that it might be effective as part of a dual treatment in the treatment of pharyngeal gonorrhoea.25 26 It is therefore important to monitor azithromycin resistance, particularly as the gonococcal population is frequently exposed to this drug as the recommended treatment for Chlamydia trachomatis co-infection. The azithromycin resistance rates fluctuated over the study period, which is consistent with surveillance studies from the United Kingdom.6 19 The modal MIC of resistant isolates to azithromycin was 1 mg/l, which is a proposed breakpoint for categorising resistance.14 Isolates with an MIC on the breakpoint are just one doubling dilution from giving a susceptible category, which is still technically valid, but may explain the inconsistent resistance rates from 2006 to 2008. The numbers, however, are small and more longitudinal data are required to establish a trend. Of great concern were the five isolates from Scotland and Ireland exhibiting high-level resistance to azithromycin (>256 mg/l). This resistance phenotype in N gonorrhoeae was first detected in Scotland in 2004,27 and has since been reported from England and Wales,28 Italy29 and Argentina.30 Widespread dissemination of high-level azithromycin resistant strains would eliminate azithromycin as a future treatment option. While no resistance to spectinomycin, another therapeutic option, was seen in this study, problems with availability of this drug in many European countries limits the utility of this as a therapeutic option.
Development and continuation of a European scheme for surveillance of gonococcal antimicrobial susceptibility is a significant achievement which has clear public health benefits. This is now an ongoing programme and the focus for the future will be to include more European countries and to overcome some of the acknowledged limitations of this study such as the variability in numbers submitted from each country annually and differences in the representativeness of the selected isolates for each country. In this study, there was no difference when the rates of resistance from the countries that participated in all 3 years were compared with all countries in each of the 3 years. However, the overall trends may be biased by the variable number of isolates a country submits in each of the 3 years and the level of representativeness from each country. Further development of this programme will also focus on increasing sampling numbers from countries with high rates of gonorrhoea and on increasing the frequency of testing so that changes in gonococci antimicrobial susceptibilities can be detected more rapidly. In addition, future European surveillance work will focus on ensuring the panel of antimicrobial agents is therapeutically relevant and has the potential for use in the future. Continued efforts to reliably link epidemiological data to the antimicrobial susceptibility data will be critical in establishing which core groups carry the burden of resistance to help focus intervention strategies.
This study has identified continuing high rates of ciprofloxacin resistance, high-level azithromycin resistance and an upward ceftriaxone MIC drift in the European gonococcal population. This demonstrates that N gonorrhoeae AMR surveillance studies are essential to inform treatment guidelines, thereby preventing onward transmission and reducing patient morbidity. These studies should continue to monitor increasing, emerging and high-level resistance, and assist in the decision-making process about future antimicrobial agent options.
Key messages
Longitudinal surveillance of antimicrobial resistance in gonorrhoea showed that ciprofloxacin is not suitable for treatment in Europe because of continuing high levels of resistance.
The emergence of high-level azithromycin resistance is of great concern as widespread dissemination of these strains would eliminate azithromycin as a future treatment option.
Ceftriaxone is an appropriate treatment for gonorrhoea in Europe as all isolates tested were susceptible.
An upward ceftriaxone MIC drift was detected in the European gonococcal population, demonstrating that this situation needs to be monitored carefully.
Acknowledgments
We thank all the ESSTI collaborators for their contribution to the ESSTI project (http://www.essti.org/). A special thanks to John Anderson, Lene Berthelsen and Maria Haller for performing the laboratory work and Tom Nichols for his statistical advice.
References
Footnotes
Members of the European Surveillance of Sexually Transmitted Infections, listed in alphabetical order by countries, are (in addition to the authors): Austria: Reinhild Strauss, FM for Health, Family and Youth; Belgium: Tania Crucitti, Institute of Tropical Medicine, André Sasse, Scientific Institute of Public Health; Cyprus: Chrystalla Hadjianastassiou, Ministry of Health; Denmark: Susan Cowan, Statens Serum Institut; Estonia: Anneli Uusküla, Tartu University Clinics, Rutta Voiko, West Tallinn Central Hospital; Finland: Eija Hiltunen-Back, National Public Health Institute; France: Véronique Goulet, Institut de Veille Sanitaire, Patrice Sednaoui, Institut Alfred Fournier; Bertille de Barbevrac, National Reference Centre of Chlamydia Infection; Germany: Peter Kohl, Dept. of Dermatology and Venerology, Vívantes Klinikum Neukölln, Osamah Hamouda, Robert-Koch Institute; Greece: Vasileia Konte, Hellenic Centre for Infectious Disease Control, Eva Tzelepi, National Reference Center for N.gonorrhoeae, Hellenic Pasteur Institute; Iceland: Guðrún Sigmundsdóttir, Centre for Infectious Disease Control, Directorate of Health, Guðrun Hauksdottir, Landspitali University Hospital; Ireland: Aidan O'Hora, Health Protection Surveillance Centre, Helen Barry, St. James Hospital; Italy: Paola Stefanelli, Barbara Suligoi, Istituto Superiore di Sanità; Latvia: Judite Pirsko, Elvira Lavrinovica, State Centre of Sexually Transmitted and Skin Diseases; Malta: Christopher Barbara, St Luke's Hospital, Jackie Maistre Melillo, Infectious Disease Prevention and Control Unit, Department of Health Promotion and Disease Prevention; Netherlands: Ineke Linde, GGD Amsterdam, Marianne van der Sande, Rijksinstituut voor Volksgezondheid en Milieu; Norway: Hilde Klovstad, Norwegian Institute of Public Health, Vegard Skogen, UNN Tromsø Universitetssykehuset; Portugal:Jacinta Azevedo, General Directorate of Health (DGS), Maria-José Borrego, Instituto Nacional de Saude Dr Ricardo Jorge; Slovak Republic; Jan Mikas, National Public Health Agency of the Slovak Republic; Slovenia: Irena Klavs, Centre for Communicable Diseases, Institute of Public Health of the Republic of Slovenia, Alenka Andlovic, Institute of Microbiology and Immunology, University of Ljubljana; Spain: Julio Vazquez, Mercedes Diez, Instituto de Salud Carlos III; Sweden: Anders Blaxhult, Inga Velicko, Swedish Institute for Infectious Disease Control, Hans Fredlund, Magnus Unemo, Swedish Reference Laboratory for Pathogenic Neisseria, Orebro University Hospital; Turkey: Peyman Altan, General Directorate of Primary Care Services, Ministry of Health; United Kingdom: Lesley Wallace, Health Protection Scotland, Hugh Young, Scottish Bacterial Sexually Transmitted Infections Reference Laboratory, Mike Catchpole, Gwenda Hughes, Emma Savage, Health Protection Agency.
Funding Financial support for this study was provided by the European Commission (DG SANCO), Agreement No 2004210: ESSTI European Surveillance of Sexually Transmitted Infections.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.