Article Text

Abstract
Objective The development of a rapid immunofiltration (flow-through) test for the simultaneous detection of non-treponemal and treponemal antibodies in the serum of patients with syphilis.
Methods The assay is rapid, inexpensive, and requires limited expertise in interpreting the results. The test is based on the principle of immunofiltration, with two antigens and control material spotted on the membrane of a through-flow device. A positive test is characterised by the appearance of three red/magenta spots within 2–10 min.
Results A total of 376 banked serum samples obtained from the Georgia Public Health Laboratory was examined by the flow-through test, the rapid plasma reagin (RPR) test and the Treponema pallidum passive particle agglutination assay (TPPA). The sensitivity and specificity of the non-treponemal spot were 96.5% and 97.7%, respectively, when compared with the RPR test, and the sensitivity and specificity of the treponemal test spot were 97.3% and 99.1% when compared with the TPPA test. In addition, the test yielded equivalent results to those obtained in comparator tests when 104 sera from cases of syphilis of known stage, 49 sera from diseases other than syphilis and 23 sera known to exhibit biological false-positive reactions were tested in parallel.
Conclusions These results indicate that the dual treponemal and non-treponemal assay could be used as a screen and confirmatory test for the serological diagnosis of syphilis in remote or resource-poor settings where there is a need to provide counselling and treatment at the initial consultation.
- Serology
- syphilis
- Treponema pallidum
Statistics from Altmetric.com
Classically, the serological diagnosis of syphilis requires the detection of two distinct populations of antibodies, namely heterophile or non-treponemal antibodies (reagin) directed against lipoidal material released from damaged host cells and possibly from the treponemes themselves, and antibodies directed against Treponema pallidum-specific antigens. Traditionally, the antigen used in the non-treponemal assays is a mixture of cardiolipin, cholesterol and lecithin. When this antigen is placed in buffered saline, it forms a flocculate when combined with antilipoidal antibodies in serum obtained from individuals with syphilis.1 This reaction forms the basis for the Venereal Disease Research Laboratory (VDRL) and the rapid plasma reagin (RPR) serological tests that are used both as initial screening tests and, when quantified, to monitor the effect of therapy and possible relapse/re-infection.
In contrast, treponemal assays detect antibodies directed against T pallidum or its components, such as the 15, 17 or 47 kDa antigens. These specific antibodies are detected by indirect immunofluorescence; the fluorescent treponemal antibody-absorption test2 3 or agglutination reactions using sensitised erythrocytes; the T pallidum haemagglutination assay4 test or gelatin particles; the T pallidum passive particle agglutination assay (TPPA) test or in enzyme immunoassays. These tests have primarily been used to confirm the specificity of reactive non-treponemal tests, because false-positive reactions can occur with sera obtained from individuals with other conditions such as acute viral infections, malaria, pregnancy, etc. Treponemal tests may also be used to confirm a clinical impression of syphilis in patients with non-reactive non-treponemal test results, particularly in late syphilis,5 6 but they cannot be used to monitor the efficacy of treatment or indicate relapse or re-infection as they often remain reactive for life.
The detection of both non-treponemal and treponemal antibodies currently requires the use of specialised equipment, with testing being performed in a laboratory setting by trained technicians. In most cases, the test results may not be available for several hours, or even days, after the specimen has been collected. A serological test for syphilis that could be performed at a clinical site, while the patient waits for the result, offers the advantage of promoting immediate counselling and treatment, and would therefore increase the effectiveness of syphilis control efforts. Currently, the only commercially available rapid syphilis tests detect treponemal antibodies.7 In common with other treponemal tests, these immunochromatographic lateral-flow tests essentially measure lifetime exposure to syphilis and do not necessarily indicate active infection that requires treatment.8–11 In contrast, in this study we describe an immunofiltration (flow-through) device developed as a result of a collaboration between the US Centers for Disease Control and Prevention (CDC) and Span Diagnostics. The test is designed simultaneously to detect the presence of anticardiolipin antibodies and provide confirmation of positive results by also detecting specific antibodies to T pallidum. In point-of-care settings, the test results can be obtained within 2–10 min and patients can be counselled regarding treatment and the need to notify partners.
Methods
Clinical specimens
Three hundred and seventy-six serum samples that had been submitted to the Georgia Public Health Laboratory for serological testing for syphilis, together with 104 serum samples from patients with known stages of the disease were selected from the CDC clinical syphilis serum panel. Of these, 10 had primary untreated, 15 primary treated, six secondary untreated, 29 secondary treated, 10 latent untreated and 50 latent treated disease. In addition, 23 serum samples known to exhibit biological false-positive reactions in the RPR test and 49 sera obtained from patients with diseases other than syphilis were also selected. All patient identifiers had been removed from serum specimens before receipt at the CDC where they were stored frozen at −70°C. On thawing, all sera were re-tested using a quantitative RPR test (Becton Dickinson, Sparks, Maryland, USA) and a qualitative TPPA assay (Fujirebio, Tokyo, Japan).
Immunofiltration device
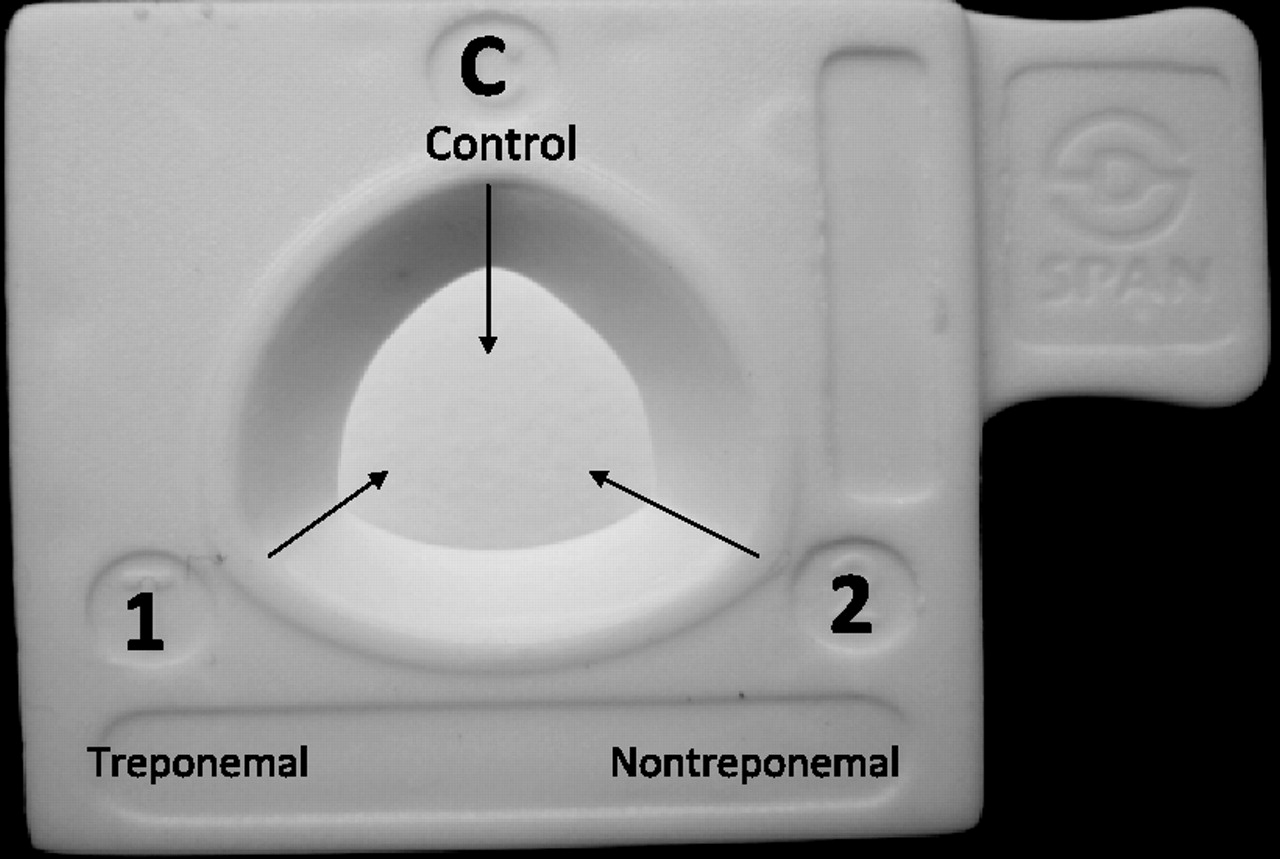
The flow-through device being evaluated was manufactured by Span Diagnostics Ltd, Surat, India. It comprises a nitrocellulose membrane with a nominal porosity of 0.6 μm laid on top of several layers of an absorbent cellulose paper pad (Advance Microdevices, Mumbai, India), within a plastic cassette (30×30 mm) with a window 8 mm in diameter that permits the application of the specimen and reagents (figure 1). Each membrane is spotted with three 0.2 μl antigen spots: one for the non-treponemal test, one for the treponemal test and one as a procedural control.

Antigen location in the dual rapid test cassette. (C) control; (1) treponemal antigen; (2) non-treponemal antigen.
Non-treponemal antigen
The non-treponemal antigen was prepared by using synthetic VDRL antigen made from an ethanolic solution of 0.03% tetramyristoyl cardiolipin, 0.14% 1-palmitoyl-2-oleolyl-sn-glycero-3-phosphocholine, lecithin and 0.9% cholesterol (Avanti Polar Lipids, Alabaster, Alabama, USA).12 A 1:10 emulsion of this antigen in phosphate buffered saline was prepared according to the standard VDRL procedure13 and centrifuged at 4360g for 45 min and resuspended in 10 mM phosphate buffer pH 6.9 containing 0.25 M EDTA, 0.72 M choline chloride and 0.01% sodium azide. A 0.2 μl aliquot of a 1% micelle emulsion was attached directly to the membrane.14
Treponemal antigen
The treponemal antigen used in the test is a recombinant T pallidum 17 kDa protein, expressed as Escherichia coli constructs (Span Diagnostics Ltd). A 0.2 μl aliquot containing 60 ng of antigen was applied to the nitrocellulose membrane. Nitrocellulose binds proteins by the strong dipole of the nitrate esters interacting with the strong dipole of the peptide bonds of the protein.15
Procedural control antigen
The procedural control antigen comprised a 0.2 μl spot of 50 μg/ml of goat antihuman IgG (Pierce Biotechnology, Rockford, Illinois, USA) in phosphate buffered saline, pH 7.2.
Detection conjugate
The detection conjugate consisted of purified recombinant protein A/G (Pierce Biotechnology) conjugated to 20 mM colloidal gold (Span Diagnostics Ltd), pH 7.2 at an optical density of 4.
Wash buffer
The wash buffer solution contained 0.5% gelatin (Bio-Rad, Hercules, California, USA), 0.5% polyethylene glycol (Sigma, St Louis, Missouri, USA), 1% choline chloride, 1% sodium chloride and 0.01% sodium azide (Fisher Chemicals, Fair Lawn, New Jersey, USA) in 50 mM phosphate buffer, pH 7.2. This solution was used both as a blocking agent and as a wash buffer.
Flow-through assay procedure
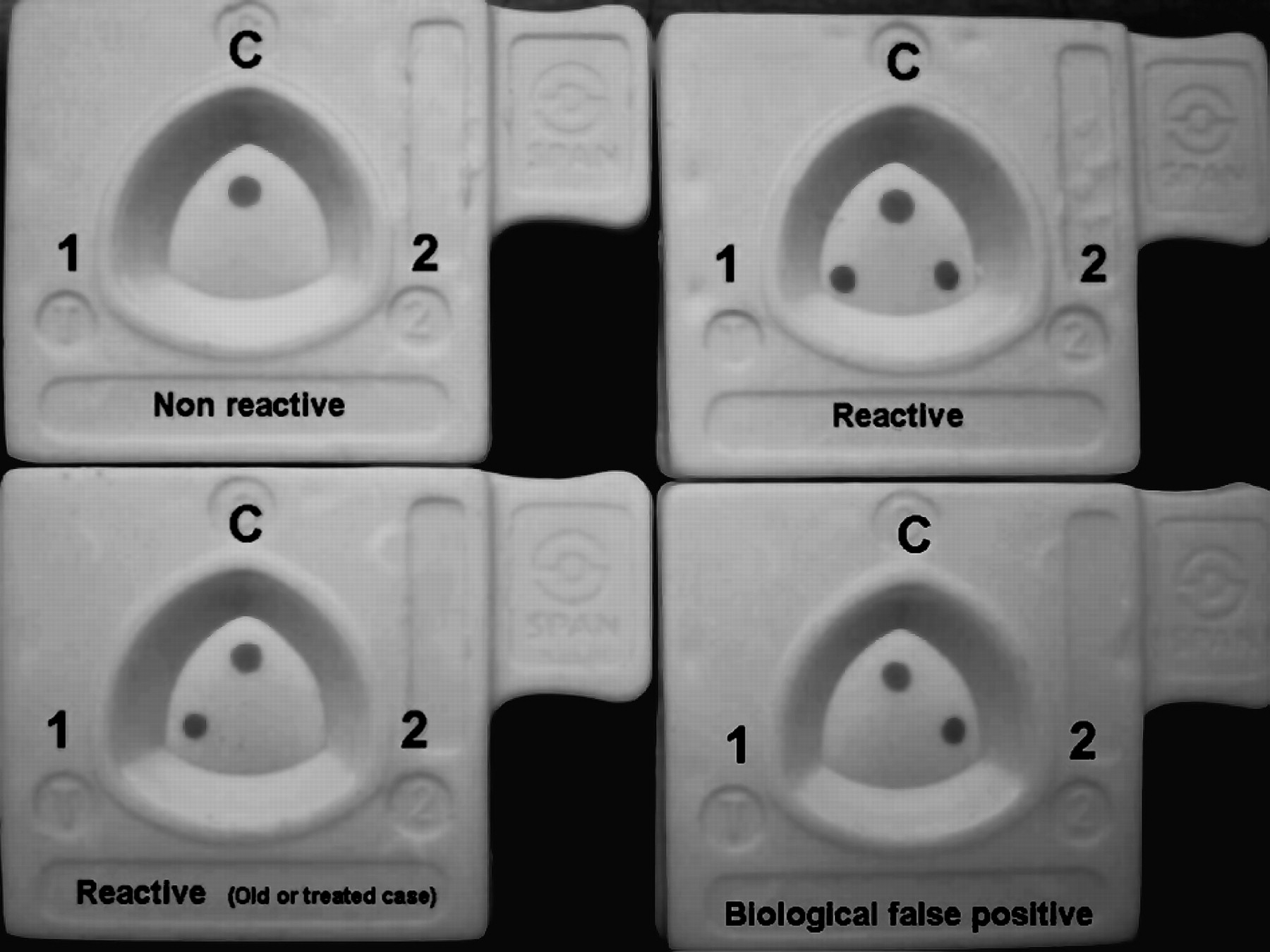
The flow-through assay was performed at room temperature. Two hundred microlitres of the wash buffer was placed into the test window and allowed to pass completely through the membrane (approximately 30 s). One hundred microlitres of the serum under test was then added and allowed to pass completely through the membrane, followed by 200 μl of buffer and 100 μl of the protein A/G gold conjugate. Finally, 200 μl of the wash buffer was added and allowed to pass through the membrane and the test results read within 2–10 min. A positive screen and confirmatory test was characterised by the appearance of three red/magenta spots a negative result was viewed as the absence of spots where the treponemal and non-treponemal antigens had been applied. The presence of a control red/magenta coloured spot was indicative of the validity of the test. A visible treponemal antigen spot (1) and control spot (C) and no detectable cardiolipin antigen spot (2) was interpreted as probably an early primary or an old or previously treated case of syphilis. A visible cardiolipin (2), and control spot (C) with no visible treponemal spot (1) was interpreted as a false-positive non-treponemal reaction. A completely negative reaction with no history of syphilis or other disease was demonstrated by the appearance of only a red/magenta control spot (C) (see figure 2).

Reactivity pattern of the dual treponemal and non-treponemal test for syphilis with positive and negative sera.
Results
Of the 376 serum samples obtained from the Georgia Public Health Laboratory, 115 were found to be reactive in both the RPR and TPPA tests. The results obtained in the dual rapid test compared with those obtained in the comparator tests for both non-treponemal and treponemal tests gave a sensitivity of 96.5% and a specificity of 97.7% for the non-treponemal test spot and a sensitivity of 97.5% and a specificity 99.1% for the treponemal test spot, respectively (table 1).
Comparison of the performance of the rapid dual syphilis test with the RPR and the TPPA assay
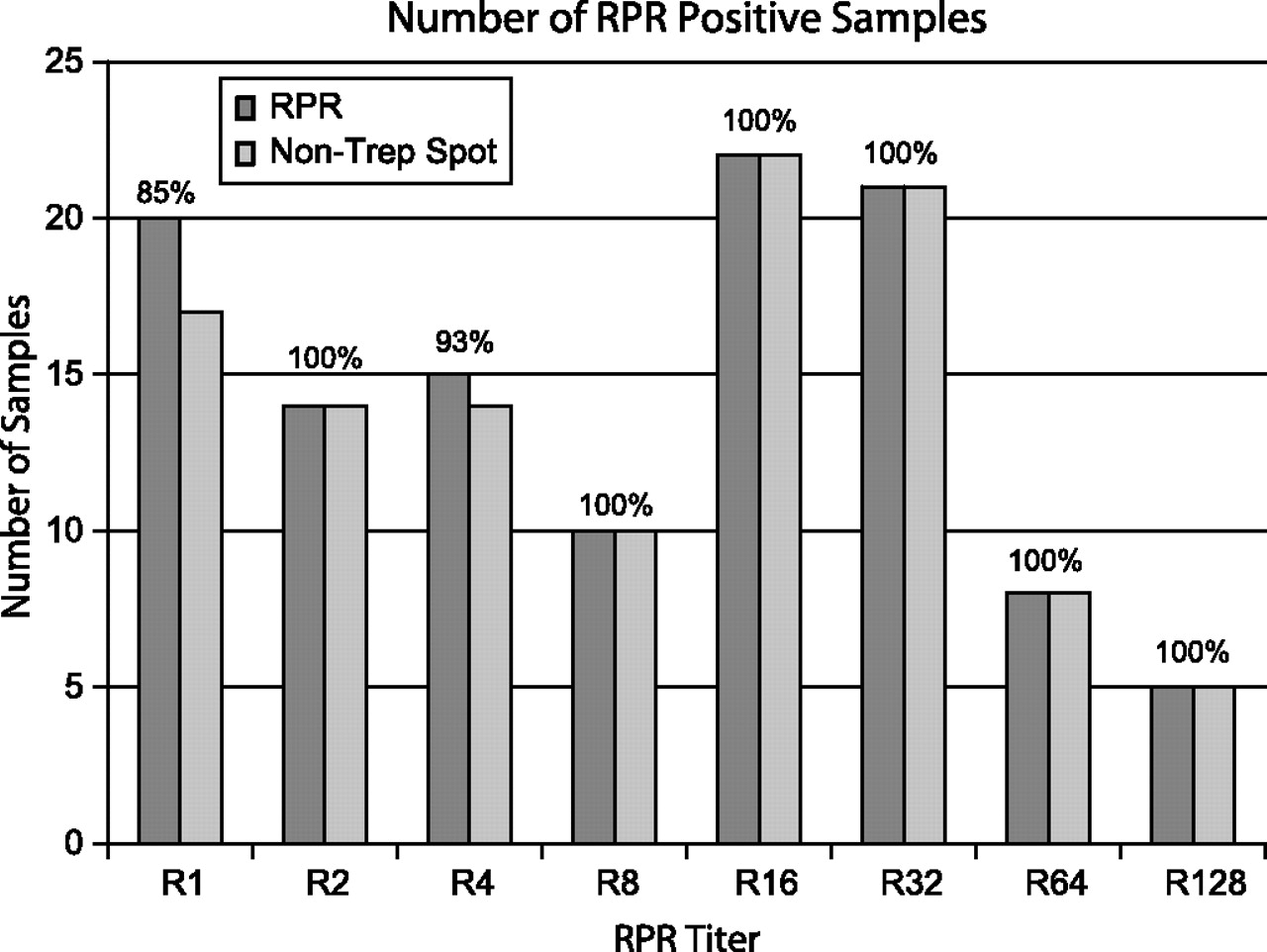
The distribution of RPR titres obtained following quantitative RPR testing of these sera is shown in figure 3. Seventeen of 20 samples classified as R1 (neat) following RPR titration were found to be reactive in the dual rapid test, yielding a sensitivity of 85.0%. All 14 sera with an endpoint titre of R2 were positive in the dual test giving a sensitivity of 100%, while 14 of 15 sera with a titre of R4 were positive in the dual test with a sensitivity of 93%. All other sera, with titres ranging from R8 to R128 proved to be positive when tested using the dual test with a sensitivity of 100% (figure 3). All these RPR/TPPA-positive sera were found to be treponemal spot-positive when tested by the rapid dual test.

{kind=link}
{kind=link}
{kind=link}
Sensitivity of the rapid dual test non-treponemal spot by rapid plasma reagin (RPR) titre.
In addition, 120 serum samples from patients with known stages of syphilis were selected from a CDC clinical serum panel. With the exception of sera obtained from two cases of untreated latent disease and one case of treated latent disease there was complete concordance between the results obtained with the rapid dual test and the comparator tests (table 2).
Documented cases of syphilis tested with the rapid dual test and the comparator RPR and TPPA tests
A further 23 sera were selected that were known to be RPR positive but negative by the TPPA. These sera have been classified as biological false positives. Of these, 16 were found to be non-treponemal spot-positive in the rapid dual test, but showed no reactivity in the treponemal spot. Forty-nine serum samples obtained from patients with diseases other than syphilis were also tested. One sample, from a patient with pinta (a non-venereal treponematosis) was, as expected, found to be reactive in both the dual test as well as the comparator RPR and TPPA tests. One serum from a case of malaria was found to be reactive in the RPR test, but negative in the non-treponemal spot in the rapid dual test. In addition, four further serum samples from malaria cases were positive in the non-treponemal spot in the rapid dual test but negative in the RPR test. As the same samples were negative in both the TPPA and the treponemal spot test in the dual test, none of these patients would have been selected for treatment for syphilis. Similarly, among the 22 serum samples obtained from patients with leprosy, six were positive in the non-treponemal spot test in the dual test, but negative in the RPR test, but all treponemal tests (both TPPA and treponemal spot tests) proved negative (table 3).
Serum samples obtained from patients with diseases other than syphilis tested with the rapid dual test and the comparator RPR and TPPA tests.
Discussion
Screening and confirmatory serological testing for syphilis are usually performed in laboratory settings, which require appropriate equipment and trained personnel to perform the test and interpret the results. As a result, serum samples are often sent to laboratories for analysis where they are screened with a non-treponemal test such as a RPR or VDRL. Ideally, the reactivity of the sera is then confirmed using a treponemal test such as a fluorescent treponemal antibody-absorption test, TPPA or enzyme immunoassays. If both the non-treponemal and treponemal tests show reactivity, then the patient is counselled and treatment provided. However, as there is often a considerable lag time in obtaining the results, the patient may not return to the clinic site for treatment. In such cases, not only does the patient remain untreated, but there are opportunities for further spread of disease.
Making the assumption that the stored sera used in this study were actual patients in a clinical study, then if the conventional laboratory approach, namely a confirmed positive RPR test and a positive dual rapid test (both non-treponemal and treponemal spots positive) are compared on the basis of whether treatment would be provided, of the 376 sera tested in this study, 115 patients would have been treated based upon the traditional testing, 111 would be treated based upon the dual test. Conversely, 111 of 115 patients who would be treated based upon the dual test would be treated based upon the traditional serology. This yields a sensitivity of 96.5% and a specificity of 98.5% for the dual rapid test when compared with the standard laboratory-based testing algorithm (table 4).
Comparison of the overall performance of the rapid dual syphilis test with laboratory-based testing using the RPR and TPPA tests
At present, the only commercially available rapid tests for syphilis detect antibodies directed against treponemal antigens. As treponemal test positivity reflects lifetime exposure to treponemal disease rather than active infection, the use of such tests invariably results in significant rates of overtreatment, particularly in high prevalence settings. In contrast, the use of the dual rapid test for syphilis described here would result in the ability both to screen and confirm the serological status of patients within 2–10 min and give a better indication of active disease. It would therefore permit the healthcare provider to initiate treatment and partner notification activities at the initial consultation. The dual rapid test exhibits remarkable performance characteristics when compared with the standard laboratory-based testing algorithm. When sera have RPR titres of 1:8 or greater, the dual rapid test has a sensitivity and specificity of 100%. As, during pregnancy, transplacental transmission of syphilis from mother to baby rarely occurs at confirmed maternal RPR titres less than 1:8,16 17 the dual rapid test should prove a useful screening/confirmation test to prevent congenital disease.
In its present format, the dual rapid syphilis test has been shown to perform adequately as a rapid test that qualitatively detects both non-treponemal and treponemal antibodies in serum, and therefore could prove to be a useful tool for the serological diagnosis of syphilis, particularly in resource-poor settings. In this particular study the test was a proof of concept requiring laboratory conditions utilising stored banked sera. However, in order for the test to be considered as a true point-of-care test, it should be able to detect these antibodies in whole blood specimens. As a result, the cassette is currently being modified by Span Diagnostics to incorporate a screen to filter cellular material from whole blood and the current five-step procedure is being reduced to one or two steps.
Key messages
This is the first study to describe a rapid dual serological test capable of detecting simultaneously both treponemal and non-treponemal antibodies in patients with syphilis.
The assay is rapid, inexpensive, and requires limited expertise in interpreting the results.
The test can be performed at a clinical site, while the patient waits for the result, aiding the clinician to make an immediate judgement on counselling and treatment.
Acknowledgments
The authors would like to thank the Institute of Medical Technology, Surat, India and Span Diagnostics Ltd for the use of their facilities, their contribution in resources and counselling. Thanks to the Georgia Department of Health Laboratories for supplying specimens for the study.
References
Footnotes
Funding The Centers for Disease Control and Prevention (CDC) provided financial support for this study in the form of allowing the principal investigator to devote time, materials and effort for the development of a non-treponemal antigen suitable for attachment to a solid support. This effort culminated in the filing of a US and international patent application no 1200700496 titled ‘Methods, Immunoassays and Devices for Detection of Anti-lipodal Antibodies’. Through a cooperative research and development agreement, Span Diagnostics obtained a licence agreement from CDC to utilise the principles of the invention to develop a working prototype. Span Diagnostics funded the developmental phase of the final commercial product.
Competing interests Span Diagnostics will market the rapid test developed cooperatively with CDC under a cooperative research and development agreement. ARC through a technology transfer agreement between CDC and Span Diagnostics may receive residuals as the inventor for the use of the CDC patent ‘Methods, Immunoassays and Devices for Detection of Anti-lipodal Antibodies’ US Patent Application Publication no 2009/0263825 A1.
Ethics approval This study was performed on archived sera from which all patient identifiers had been removed. Protocols for studies using these sera for the development of new serological test for syphilis were reviewed by the institutional review board of the CDC (protocol no 2018) and determined to be exempt from further review.
Provenance and peer review Not commissioned; externally peer reviewed.