Article Text

Abstract
What interventions are effective and cost-effective in increasing the uptake of HIV testing among men who have sex with men (MSM)? A systematic review was conducted of the following databases: AEGIS, ASSIA, BL Direct, BNI, Centre for Reviews and Dissemination, Cochrane Database of Systematic Reviews, CINAHL, Current Contents Connect, EconLit, EMBASE, ERIC, HMIC, Medline, Medline In-Process, NRR, PsychINFO, Scopus, SIGLE, Social Policy and Practice, Web of Science, websites, journal hand-searching, citation chasing and expert recommendations. Prospective studies of the effectiveness or cost-effectiveness of interventions (randomised controlled trial (RCT), controlled trial, one-group or any economic analysis) were included if the intervention aimed to increase the uptake of HIV testing among MSM in a high-income (Organization for Economic Co-operation and Development) country. Quality was assessed and data were extracted using standardised tools. Results were synthesised narratively. Twelve effectiveness studies and one cost-effectiveness study were located, covering a range of intervention types. There is evidence that rapid testing and counselling in community settings (one RCT), and intensive peer counselling (one RCT), can increase the uptake of HIV testing among MSM. There are promising results regarding the introduction of opt-out testing in sexually transmitted infection clinics (two one-group studies). Findings regarding other interventions, including bundling HIV tests with other tests, peer outreach in community settings, and media campaigns, are inconclusive. Findings indicate several promising approaches to increasing HIV testing among MSM. However, there is limited evidence overall, and evidence for the effectiveness of key intervention types (particularly peer outreach and media campaigns) remains lacking.
- AIDS serodiagnosis/psychology
- health behaviour
- health promotion
- HIV infections/diagnosis
- HIV testing
- homosexual
- homosexuality
- male
- systematic review
Statistics from Altmetric.com
- AIDS serodiagnosis/psychology
- health behaviour
- health promotion
- HIV infections/diagnosis
- HIV testing
- homosexual
- homosexuality
- male
- systematic review
There are estimated to be 33 300 men who have sex with men (MSM) living with HIV in the UK, of whom 8950 are undiagnosed (2008 figures).1 Strategies to prevent HIV in this population include public health education and community-based awareness raising about the risks of HIV, and the promotion of safer sex through condom distribution, outreach work and other means. Increasing the uptake of voluntary counselling and testing also has a potentially important role to play in reducing the incidence of HIV. Of MSM attending genitourinary medicine clinics in 2008, 3.1% were found to have a previously undiagnosed HIV infection.1 Promoting HIV testing has the potential to reduce undiagnosed infections, thus improving individual outcomes and reducing transmission. It may also be of value in raising awareness of HIV more broadly, and engaging MSM with sexual health services.
Promoting HIV testing may be of particular value in reducing late diagnoses. Of new HIV diagnoses among MSM in 2008, 43% had CD4 cell counts below the threshold at which treatment should normally be commenced (<350 cells/mm3 within 3 months of diagnosis) and 20% had CD4 cell counts less than 200 cells/mm3.1 Late HIV diagnosis is an important predictor of morbidity and mortality. Those who start treatment at a more advanced stage of disease respond less well to treatment, and remain at increased risk of death for many years following treatment initiation.2
Rates of HIV testing among MSM vary widely between countries3 and between subgroups of MSM within the UK.4 Rates have varied over time; survey data show a steady upward trend in numbers ever tested for HIV in samples of MSM in the UK since 2000.5 Testing policies also vary internationally, although there is a general trend towards recommending more routine testing.6 Current UK guidelines recommend that HIV testing should be offered to MSM annually, and more frequently if symptoms indicative of seroconversion or high-risk exposure are present.7 US guidelines recommend annual screening for MSM who themselves or whose sex partners have had more than one sex partner since their most recent HIV test.8 ‘Opt-out’ testing policies in sexually transmitted infection (STI) clinics are now widely implemented, having been recommended by WHO and UNAIDS in 2004,9 and by UK guidelines in 2006.10 Current UK guidelines also recommend opt-out testing in a much wider range of healthcare settings.7
We aimed systematically to review the evidence on the effectiveness and cost-effectiveness of interventions to increase the uptake of HIV testing among MSM. The study presented here is part of a larger review, which also included relevant qualitative evidence, commissioned by the National Institute for Health and Clinical Excellence (NICE) (the review protocol has not been published). The full methods and results are available at http://www.nice.org.uk/guidance/index.jsp?action=download&o=50931. This review includes only interventions that aimed to promote HIV testing, although it is clear that the promotion of HIV testing should form part of an integrated risk-reduction strategy aiming to change a range of sexual behaviours.11 12
To our knowledge, no systematic review with this scope has previously been conducted. Two high-quality systematic reviews whose scope partly overlaps with that of the present review were located by our searches. One of these focused on mass media interventions to promote HIV testing, but included all populations, not only MSM.13 The other included HIV health promotion interventions for MSM in general, but did not have a primary focus on HIV testing, and did not include a separate synthesis of evidence relating to interventions promoting HIV testing.14
Methods
Identification of studies
We searched the following databases from 1996 to December 2009: AEGIS (AIDSLine and International AIDS Society abstract archives); ASSIA; BL Direct; British Nursing Index; Centre for Reviews and Dissemination databases (including DARE and NHS EED); Cochrane Library (including the Health Technology Assessment database and CENTRAL); CINAHL; Current Contents Connect; EconLit; EMBASE; ERIC (Education Resources Information Centre); HMIC; Medline; Medline In-Process; National Research Register; PsycINFO; Scopus; SIGLE; Social Policy and Practice; Web of Science (including Social Science Citation Index, Science Citation Index and Conference Proceedings Citation Index).
Whenever possible, searches were limited to studies of humans published in English. The Medline search strategy is presented in supplement 1 (available online only). Full search strategies are available in the complete review report.15 Searching was conducted simultaneously for this review and the review of qualitative evidence (the strategy was designed to locate both types of evidence, and all references were screened for inclusion in both reviews).
In addition, we hand-searched nine key journals from January 2005 to December 2009; scanned the citation lists of included studies and those of systematic reviews that met all other criteria for inclusion; and conducted ‘forward’ citation chasing on included studies using ISI Web of Knowledge. Finally, a call for evidence to experts and stakeholders was issued; all references arising from the call were screened for inclusion.
Inclusion criteria
The inclusion criteria were as follows: (1) Does the study include MSM, or focus on services aimed at MSM? (2) Does the study relate to HIV testing? (3) Was the study conducted in a country that is a current member of the Organization for Economic Co-operation and Development? (4) Was the study published in 1996 or later? (5) Does the study include MSM who are HIV negative or do not know their HIV status, and are competent to consent to an HIV test? (6) Does the study relate to an intervention that aims to increase the uptake of HIV testing? (7) Is the study a prospective outcome evaluation (randomised or non-randomised controlled trial (RCT), or one-group before-and-after study), or a cost–benefit or cost-effectiveness analysis, or any other type of economic evaluation?
For criterion (1), studies that either had a sample more than 50% of whom were MSM, or presented disaggregated outcome data on the MSM within the sample, or focused on services aimed at MSM, were included. Studies of the general population that did not present outcome data on MSM were excluded. Studies published before 1996 were excluded (criterion 4) due to the lesser relevance of data collected before the introduction of effective antiretroviral treatment for HIV.
For criterion (7), effectiveness studies were included if they either contained a comparison group receiving different interventions (randomised or non-randomised) and/or presented outcome data for both before and after the intervention, or both. Any economic evaluation was included regardless of the study design. Systematic reviews were not included; however, systematic reviews meeting criteria (1)–(6) were retained and their lists of included primary studies scanned for inclusion.
A random sample of 10% of abstracts was screened by two reviewers independently. Interrater reliability (Cohen's κ) was κ=0.627. Subsequently, all abstracts were screened by one reviewer alone. For all references included on abstract, the full text was retrieved and re-screened independently by two reviewers, with disagreements resolved by discussion and reference to a third reviewer if necessary.
Study quality
Study quality was assessed using a standardised tool.16 The full quality assessment tool is presented in supplement 2 (available online only). Both quality assessment and data extraction were conducted for a sample of 10% of studies (N=2) by two reviewers independently; subsequently, all references were quality-assessed by one reviewer and then checked in detail by a second reviewer. On the basis of this quality assessment, each study was assigned a rating: high (++), medium (+) or low (−). Quality ratings are presented for each study below; studies were not formally weighted by quality in the synthesis.
Data extraction and synthesis
Data were extracted from the studies using a standardised tool.16 The list of variables for which data were extracted is presented in supplement 2, available online only. Outcome data were only extracted regarding the uptake of HIV testing and the number of new diagnoses; data on other outcomes (eg, condom use) were not extracted. Due to the heterogeneity of intervention types, quantitative meta-analysis was not carried out, and studies were synthesised narratively.
Results
A total of 4342 unique references was located by our searches (this figure includes studies for the qualitative review as well as those for this review). After screening, a total of 14 study reports on effectiveness and one on cost-effectiveness was retained in the review. Two of these were linked reports presenting data from the same study. Therefore, a total of 12 effectiveness studies and one cost-effectiveness study was included. The flow of literature through the review is presented in figure 1.
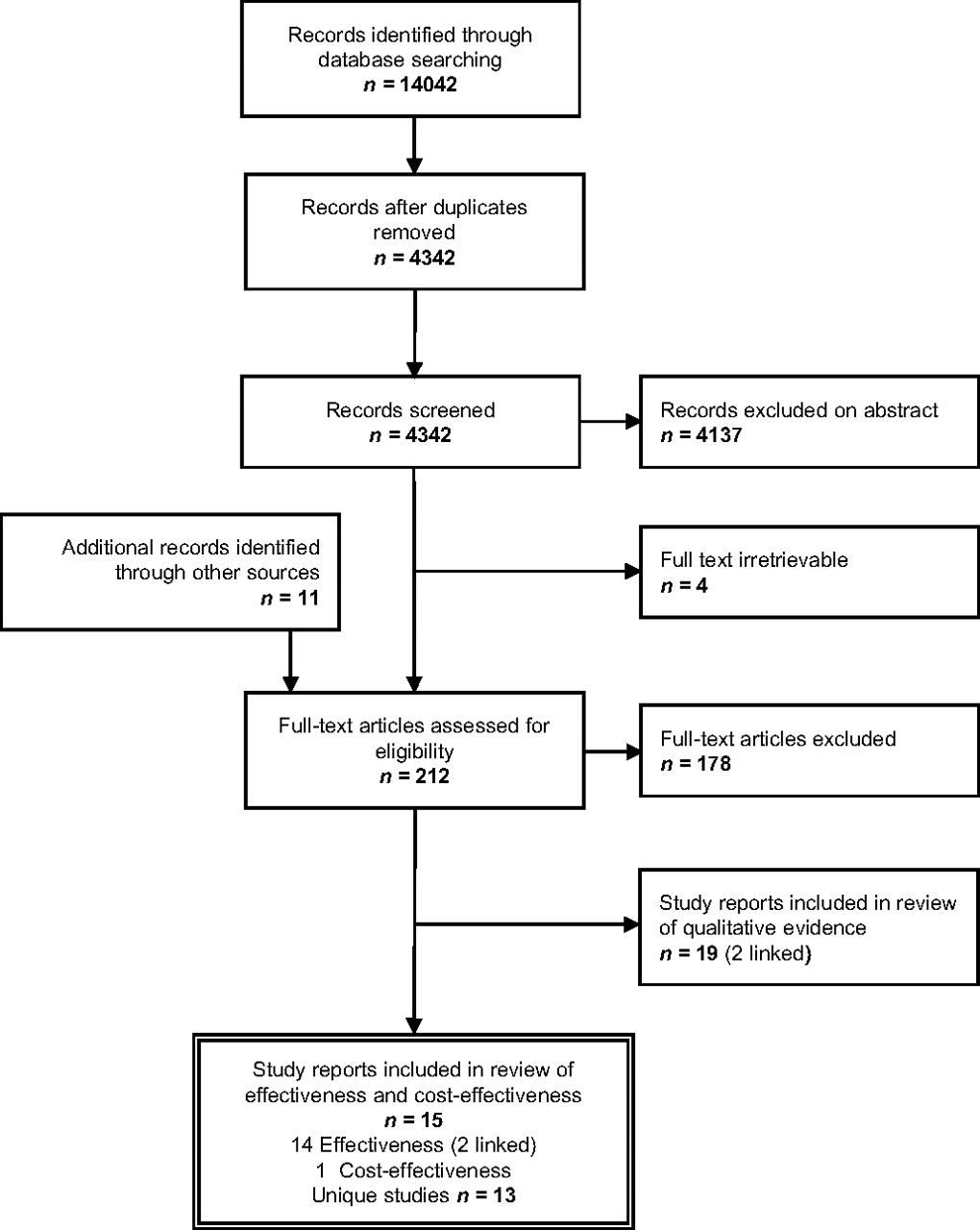
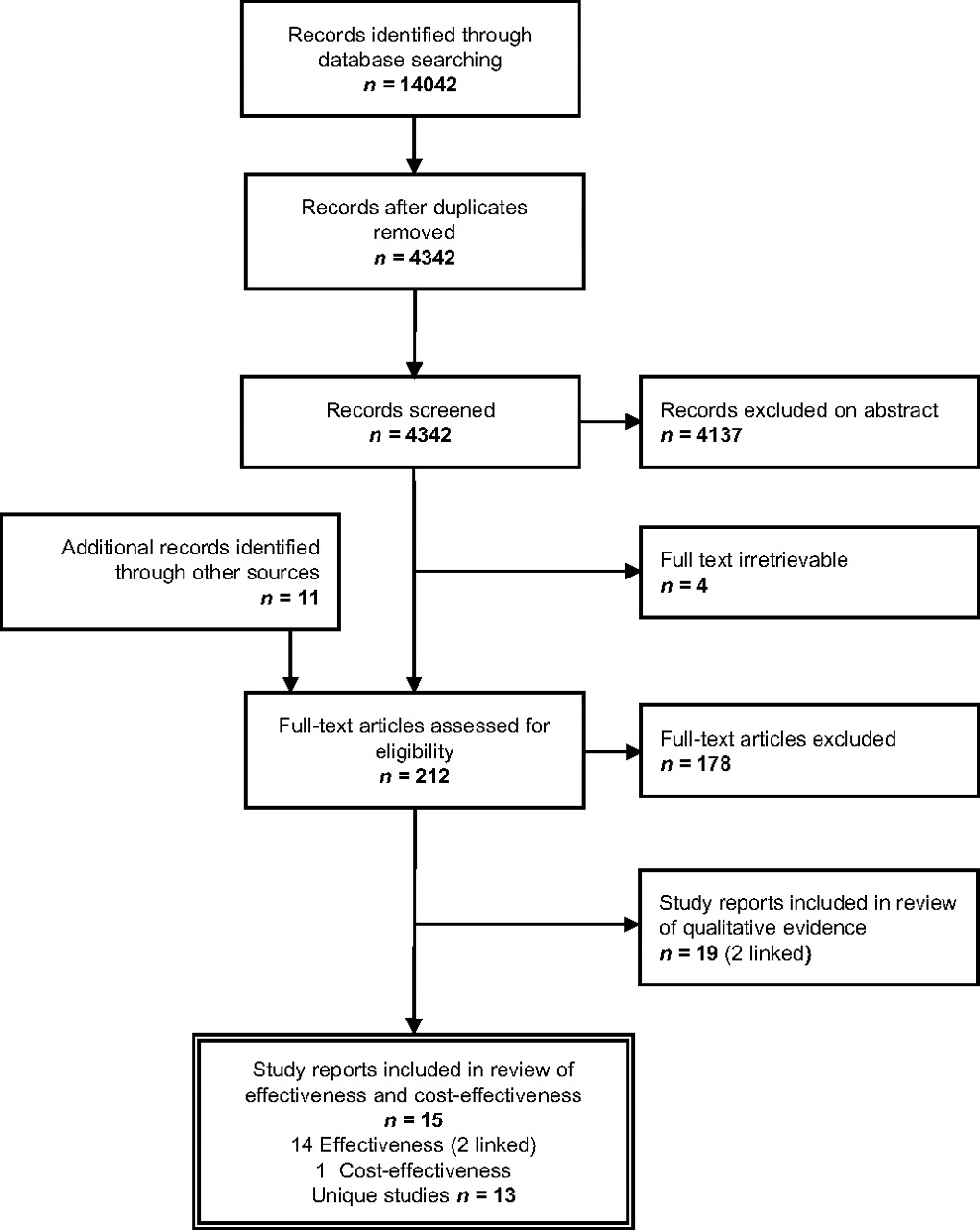{kind=link}
Flow of literature diagram.
Basic characteristics of the study settings and populations are set out in table 1. Table 1 also shows the results of the quality assessment process (full details are given in the full report).15 Table 2 sets out the interventions evaluated and the findings of the studies. We have divided the interventions into four categories: (1) offering different types of test or testing protocols in outreach settings;17–19 (2) peer education or recruitment programmes, including intensive residential programmes24 and community-based programmes;20 22 25 (3) community-based media campaigns26 27 and web-based educational interventions;28 and (4) changes to the way in which services are delivered in STI clinics, including the introduction of opting-out schemes29 30 and the implementation of guidelines recommending regular screening.31
Summary of included studies: population characteristics
Summary of included studies: interventions and outcomes
Broadly, these four categories can be grouped as service delivery interventions (1 and 4) and community-level interventions (2 and 3).
Type of test and testing protocol
One study from the USA, published in 2006, compared the uptake of HIV tests included with a package of other tests (for other STI, alcohol and drug dependence and depression) offered in outreach settings (bars) with that of HIV tests alone.18 This study found no significant difference in uptake between the two groups. However, there were some promising but non-significant trends among high-risk subgroups towards greater acceptance of the packaged tests compared with the HIV test alone.
One study, also from the USA and conducted in 1999–2000, compared traditional serum testing and counselling with rapid serum testing and oral fluid testing offered in a gay bathhouse.17 This study found that both rapid serum testing and oral fluid testing were significantly more likely to be accepted than traditional testing. This study provides evidence that rapid testing modalities can increase uptake in an outreach setting compared with traditional testing.
A further US study, conducted in 1996–7, compared oral fluid and blood spot home testing kits, finding high levels of adherence to both types of test.19
Peer education and recruitment
Two studies from the UK, both from the late 1990s (1996–9), used non-randomised designs to investigate the effectiveness of peer-led community-based risk-reduction campaigns.20 22 Both of these studies found such campaigns not to be effective in increasing HIV testing among a community sample of MSM. However, there are limitations in the design and reporting of both these studies (see Discussion), so they arguably do not provide conclusive evidence for the ineffectiveness of peer-led strategies.
One RCT conducted in 2005–7 evaluated an intensive weekend residential programme for black MSM in the USA led by trained MSM peers.24 This study found a small but significant improvement in HIV testing rates among participants at the 6-month follow-up.
One economic analysis, conducted in 2002–5, looked at a peer recruitment programme to increase rates of HIV testing, finding a cost per new case of HIV identified of US$4929.25 According to the study authors, this compares favourably with costs per case for other interventions, although the analysis presented falls considerably short of a full cost-effectiveness analysis.
Media and web-based campaigns
Two non-comparative studies in Australia and England investigated community-based media campaigns to promote HIV testing among MSM, including components such as display advertising and websites and print media distributed to gay venues and organisations.26 27 One of these studies, conducted in 2004–6, found no increase in the numbers of MSM in the targeted location reporting an HIV test in the previous year.26 The other, conducted in 1999–2000, found a substantial increase in HIV tests conducted in the targeted clinic.27 However, there are flaws in the design of both these studies (see Discussion). Overall, the evidence for media campaigns must be regarded as inconclusive.
One further non-comparative study in the USA, conducted in 2005–6, evaluated an educational video that was accessed through a banner advert on a gay sexual meeting website.28 This study found a significant increase in HIV testing at the 3-month follow-up (and a substantial number of new diagnoses were made as a result). This finding is promising, although as the study is non-comparative, it does not permit strong conclusions to be drawn.
STI clinic service delivery
Two studies from the mid-2000s (2003–7), both non-comparative, investigated the introduction of ‘opt-out’ policies in STI clinics in The Netherlands, such that all clients attending the clinic received an HIV test unless they requested not to have one.29 30 Both the studies found substantial increases in HIV tests among MSM after the introduction of the opt-out policy. A finding of concern in both these studies was that certain groups, particularly older MSM and MSM with potentially STI-related symptoms, were more likely to opt out of testing after the introduction of the policy.
One study from 2000–2, also non-comparative, found that the implementation of guidelines promoting regular HIV testing in an STI clinic resulted in an increase in the proportion of MSM being tested, although it is unclear if the increase reached significance.31
Discussion
This review indicates that several promising strategies are available to increase the uptake of HIV testing among MSM. Opt-out policies in STI clinics can increase testing rates, although there remain concerns about high rates of refusal among certain high-risk subgroups (as well as about those MSM who do not attend STI clinics). Offering rapid testing in outreach settings can also increase the uptake of testing compared with traditional testing methods.
However, there is limited evidence for the effectiveness of community-level strategies. One study shows that a holistic group intervention, led by trained peers, can increase testing among a minority ethnic, socioeconomically disadvantaged group of MSM. While this is a promising result, such interventions are resource intensive and may be challenging to implement. Nonetheless, further research on such strategies would be valuable. There are also promising findings, warranting further research, regarding a web-based intervention.
Evidence regarding media campaigns and peer-led outreach strategies is inconclusive. Methodologically, evaluations of existing programmes would benefit from measuring individual-level outcomes among men exposed to the intervention, as well as population-level outcomes, and from indexing outcome measures to the timeframe of the intervention (ie, recent testing rather than lifetime testing). With regard to intervention content, more intensive programmes, sustained over longer timeframes and reaching a larger proportion of the population, are likely to have more impact, as studies of media campaigns in other fields have found.32 Using formative research, or the published qualitative literature, could also be of value in targeting the content of such interventions.
Several limitations in the evidence should be noted. The findings show that, even when interventions succeeded in increasing uptake, the numbers of new diagnoses were generally modest. Baseline rates of recent HIV testing in the targeted populations were often high: for example, the study by Spielberg and colleagues17 excluded 35% of potential participants because they had already had an HIV test within the past 3 months. In addition, most studies recruited primarily from gay venues and/or MSM-oriented services or organisations, and were unlikely to include less gay-identified MSM. These points raise the question as to whether evaluated interventions reach those MSM who are most at risk of having undiagnosed HIV.
Other limitations relate to the methods of the primary studies, particularly those evaluating community-level interventions. First, several studies used non-comparative designs and were conducted over several years. This makes it difficult to distinguish the effects of the intervention from longer-term upward trends in testing behaviour. Second, several studies measured outcomes at a population level (ie, different individuals were sampled pre and post-test), meaning that any measurement of effectiveness may be diluted by changes in the population. This is particularly an issue when the reach of interventions is limited; two studies found that relatively few of the targeted populations could recall direct contact with the intervention post-test (29%20 and 3%22). A third limitation relates to the measurement of outcomes: the use of lifetime HIV testing rather than recent testing,20 22 or the total number of HIV tests conducted by specific services,27 may not provide an accurate picture of changes in testing behaviour.
There are also some limitations in the review itself, primarily because of its intentionally restricted scope. This review did not consider evidence relating to HIV testing in populations other than MSM, although this evidence is potentially relevant; for example, there is evidence that mass media interventions are effective in the general population.13 It also did not consider the considerable evidence on other risk-reduction strategies among MSM. This evidence would be valuable in providing the context needed to understand the longer-term impacts of successful interventions to promote HIV testing among MSM. For example, the role of testing in serosorting strategies, which remain prevalent among some groups of MSM and may involve a substantial risk of infection,33 34 suggests that the relation between the uptake of testing, infection rates and health status is complex and unpredictable. Therefore, interventions to promote testing, in isolation, may not have a substantial impact on rates of infection. Such interventions are more likely to be effective as part of an integrated programme for reducing HIV infections and promoting access to antiretroviral treatment among MSM.
Key messages
Interventions to promote the uptake of HIV testing among MSM have the potential to reduce HIV risk and late diagnoses.
Opt-out testing policies, and offering rapid testing, can increase the uptake of HIV testing among MSM.
Evidence concerning the effectiveness of community-level strategies, such as media campaigns or peer education and recruitment, is inconclusive.
Strategies to promote testing should be seen in the broader context of a comprehensive approach to HIV prevention.
References
Supplementary materials
Web Only Data sti.2010.048280
Files in this Data Supplement:
Footnotes
Funding This review was funded by the National Institute for Health and Clinical Excellence (NICE). The authors would like to thank the NICE project team (Chris Carmona, Catherine Swann, Daniel Tuvey and Linda Sheppard) for their invaluable support and guidance throughout the review. The views and opinions expressed are those of the authors alone and do not reflect the official opinion of NICE, or any guidance issued by NICE.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.