Article Text

Abstract
Background Since May 2004, 10 central and east European (CEE) countries have joined the European Union. While HIV rates remain low among men who have sex with men (MSM) in CEE countries, there is no research on the sexual behaviour of CEE MSM in the UK.
Methods CEE MSM living in the UK (n=691) were recruited for an online questionnaire by two popular MSM websites.
Results The majority of men had arrived in the UK since May 2004. A previous sexually transmitted infection (STI) diagnosis was reported by 30.7%, and 4.8% reported being HIV positive, the majority diagnosed in the UK. Unprotected anal intercourse with a casual partner of unknown or discordant HIV status was reported by 22.8%. Men who had been in the UK for longer (>5 years vs <1 year) reported more partners in the past 5 years (67.2% vs 50.4% had >10 partners, p<0.001) and were less likely to report their most recent partner was from their home country (14.9% vs 33.6%, p<0.001). Among migrant CEE MSM living in London, 15.4% had been paid for sex in the UK and 41.5% had taken recreational drugs in the past year.
Conclusion CEE MSM in the UK are at risk for the acquisition and transmission of STI and HIV through unprotected anal intercourse with non-concordant casual partners. Sexual mixing with men from other countries, commercial sex and increased partner numbers may introduce additional risk. This has important implications for the cross-border transmission of infections between the UK and CEE countries.
- Gay men
- HIV
- migration and health
- sexual behaviour
- STD
Statistics from Altmetric.com
On 1 May 2004, the Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Slovakia and Slovenia (the Accession 8 or A8) joined the European Union (EU), followed by Romania and Bulgaria (A2) on 1 January 2007. The accession of these 10 central and eastern European (CEE) countries resulted in a large influx of predominantly young economic migrants to the UK.1
The levels of syphilis reported across the CEE region are varied. In 2007, new syphilis diagnoses (per 100 000) were 22.7 in Romania, compared with 6.2 in the UK and 2.2 in Poland. However, new diagnoses of HIV (per 100 000) were higher in the UK (12.0) than all CEE countries, with the exception of Estonia (40.7) and Latvia (15.8),2 where the HIV epidemic is largely driven by injecting drug use.3 Within the population of men who have sex with men (MSM), the number of new HIV diagnoses in all 10 CEE countries has remained lower than in Europe as a whole (with rates of HIV diagnoses per million men aged 15–64 years ranging from 1.1 in Romania to 35.1 in Slovenia). The UK has the highest rate of newly diagnosed cases of HIV infection among MSM in Europe (130.1 per million men).4
Although homosexuality is no longer a criminal offence in CEE countries, stigmatisation and discrimination are widely reported in the region.5 6 This may impact upon the sexual knowledge and behaviours of CEE MSM, as well as their willingness to access sexual health services. Furthermore, migrants are characterised as risk-takers, with the risks that they take in moving from one country to another filtering through to other areas of their lives.7 The extent to which sexual risk behaviours are practised by CEE migrant MSM in the UK therefore requires investigation.
As part of the sexual attitudes and lifestyles of London's eastern Europeans (SALLEE) project, this study set out to examine the risk for HIV and sexually transmitted infections (STI) and the use of sexual health services among migrant CEE MSM in the UK.
Methods
Participants and procedure
The SALLEE project was based on a cross-sectional survey and semi-structured in-depth interviews with CEE men and women living in London. The methods are described in detail elsewhere.8 The analysis presented here is based on the cross-sectional survey and used a specific strategy for recruiting CEE MSM from across the UK, as described below.
Data source
We conducted an anonymous, online questionnaire in 12 languages (the 10 official languages of the CEE countries plus English and Russian), which took approximately 10 minutes to complete. No financial incentive to take part was offered. After respondents ticked a box to indicate consent, they were asked questions on background information, including sociodemographic characteristics and the use of general practitioner (GP) services; sexual health, including sexual practices, numbers of partnerships, use of condoms, paying for sex, STI and HIV and the use of sexual health services, and questions on injecting and recreational drug use. When possible, questions from previously validated questionnaires were used in order to maximise their reliability and validity.
Eligible respondents were literate men aged 18 years and over who self-identified as migrants from one of the 10 CEE countries. The men in the present study were recruited by means of two popular dating websites for gay men in the UK. The questionnaire was posted online and a link to it was placed on banners that appeared when men were browsing the personal profiles of London men in Gaydar (http://www.gaydar.co.uk) for 6 weeks (March to April 2009). A link was also placed on the homepage of GayRomeo (http://www.gayromeo.com) for 4 weeks (April to May 2009). While the SALLEE project was primarily interested in CEE migrants in London, the online invitation in Gaydar and GayRomeo was extended to respondents throughout the UK.
Statistical analysis
Standard statistical tests including χ2, Student's t test and Mann–Whitney U test were used to examine associations between the place of residence and background characteristics, risk behaviour and health service use. Linear-by-linear associations were examined to assess the effect of the length of time in the UK on risk behaviour and health service use, by grouping respondents' length of stay into yearly intervals up to 5 years (eg, up to 1 year, 1–2 years), then over 5 years. Logistic regression modelling was used to obtain OR and adjusted OR (aOR) to examine the association between unprotected anal intercourse (UAI) with a casual partner and background characteristics, commercial sex, recreational drug use and HIV status (which are associated with UAI in other MSM populations). Analysis was performed using SPSS version 12.0.
The study was granted approval from the Camden and Islington Community Research Ethics Committee (07/H0722/110).
Results
Background characteristics
Over the course of the recruitment by Gaydar and GayRomeo, 691 online responses were submitted by men who were eligible for the study. Eligibility was restricted to men reporting one or more male sexual partners in the past 5 years, so that only men who were homosexually active were included in the analysis. More men were recruited from GayRomeo (65%, n=449) than Gaydar (35%). Men living outside London were more likely to be recruited from GayRomeo than men living in London (80.1% vs 58.6%, p<0.001) (table 1).
Background characteristics, by place of residence
The majority of men (70.2%) lived in London and the rest (n=206) were distributed throughout the UK: 42.2% in the south of England, 18.0% in the Midlands, 18.0% in the north of England, 15.5% in Scotland, 3.9% in Northern Ireland and 2.4% in Wales. The mean age of all men was 29 years (SD 6.9 years). The majority were working, educated to degree level, came from one of the A8 countries rather than Bulgaria or Romania, completed the questionnaire in their native language and had been in the UK for more than 1 year. Most men had arrived in the UK since May 2004 (73.0%). Sex with women in the past year was reported by 6.5% of men. There were no significant differences between London men and those who were living outside London on any of these variables (table 1).
Men who had been in the UK for longer were more likely to live in London: 65.0% of men who had been in the UK for up to 1 year compared with 80.3% of men who had been in the UK for more than 5 years (p=0.008).
Risk behaviour
Compared with men living outside London, London men were significantly more likely to report that they had been paid for sex in the UK (15.4% vs 6.8%, p=0.005), had ever been diagnosed with an STI (34.1% vs 22.5%, p=0.003) and had taken recreational drugs in the past year (41.5% vs 25.2%, p<0.001) (table 2). They were more likely to have ever paid for sex with a man (15.0% vs 9.8%, p=0.068). They were also less likely to report assortative sexual mixing (whereby their last partner was from their home country) (18.6% vs 29.1%, p=0.003). Almost half the men reported that their most recent partner was from the UK (47.6%) and a further 15.4% of most recent partners were from another European country.
Risk behaviour and health service use, by place of residence
The majority of men living in London and elsewhere in the UK reported anal intercourse with a man in the past year (92.4% and 89.8%, p=0.269). London men reported more anal intercourse partners in the past year than men living elsewhere (median five vs three, p<0.001).
Health service use in the UK
Compared with men living elsewhere, London men were more likely to have attended a sexual health clinic in the UK (53.2% vs 36.6%, p<0.001), to have obtained condoms from health services in the UK in the past year (32.6% vs 21.1%, p=0.004) and to have tested for HIV (83.0% vs 68.3%, p<0.001) (table 2). A somewhat larger proportion of men living outside London were registered with a GP (79.3% vs 72.3%, p=0.053) but they were not more likely to have attended the GP for reasons related to sexual health in the past year (18.3% vs 17.2%, p=0.722).
Migration and integration
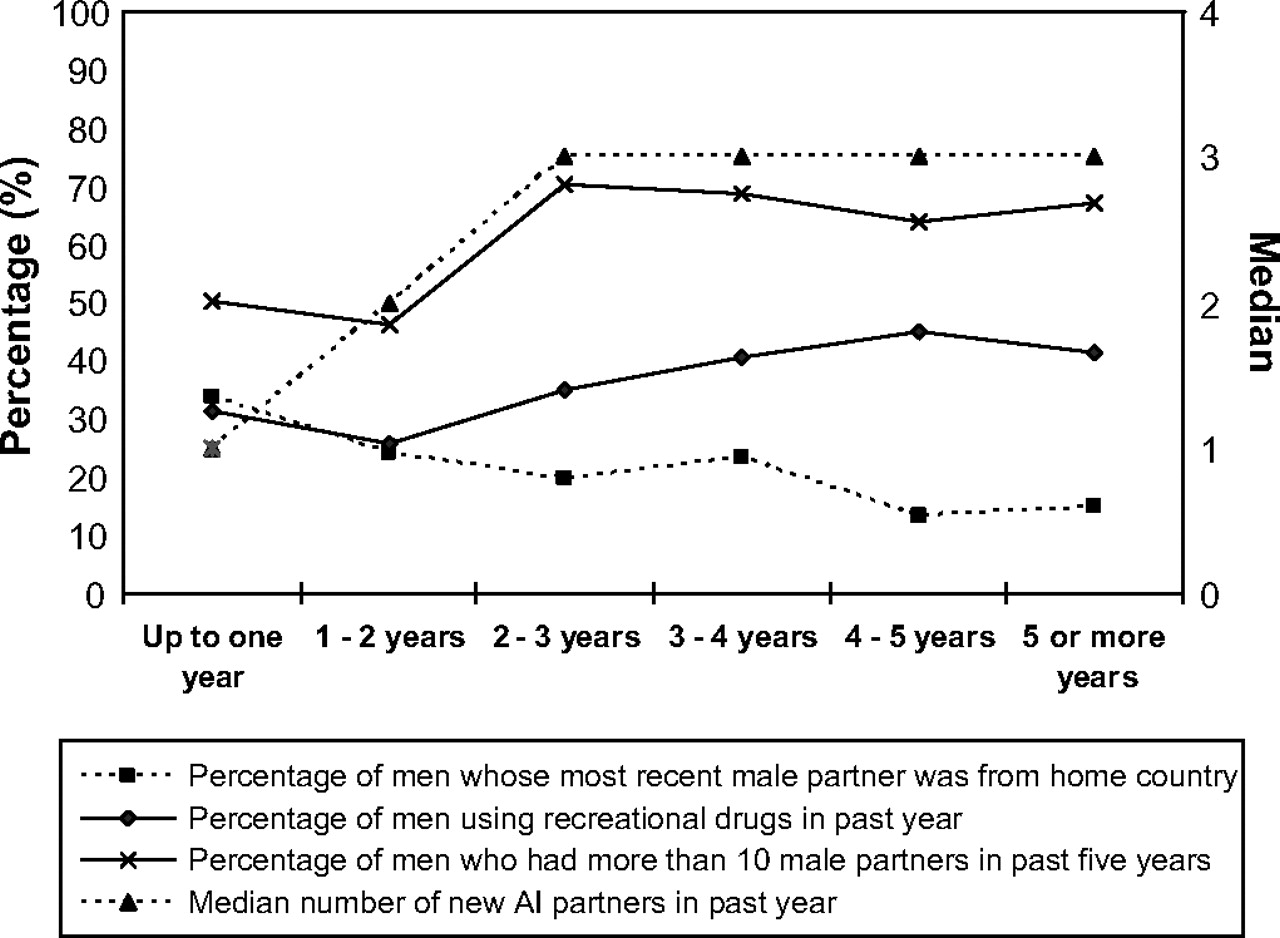
The longer men had been in the UK, the less likely they were to report assortative sexual mixing (33.6–14.9%, p<0.001) and the more likely they were to report recreational drug use in the past year (31.4–41.4%, p=0.005) (figure 1). Figure 1 also illustrates how men who had been in the UK for longer reported more partners and more new partners. Men who had been in the UK for over 2 years reported more than 10 male partners in the past 5 years more frequently than men who had been in the UK for less time (67.6% vs 48.6%, p<0.001). Men who had been in the UK for over 2 years also reported a median of three new anal intercourse partners in the past year compared with a median of two among men who had been in the UK for less time (p=0.002).

{kind=link}
Change in assortative sexual mixing, use of recreational drugs and number of male partners over time in the UK.
Most of the other risk behaviours listed in table 2 were not associated with time in the UK: there were no significant associations between the length of time in the UK and being paid for sex, injecting drugs, anal intercourse in the past year, UAI with a casual partner, non-concordant UAI with a casual partner and non-concordant UAI with a main partner. However, the data suggested that ever being diagnosed with an STI increased the longer men had been in the UK, rising from 27.6% of men who had been in the UK for up to 1 year to 37.2% of men who had been in the UK for at least 5 years (p=0.035); and men who had been in the UK for longer were also somewhat more likely to report ever paying for sex (12.4–18.1%, p=0.026).
GP registration increased the longer men had been in the UK (44.3–87.9%, p<0.001). Men who had been in the UK for longer were also more likely to have attended a sexual health clinic in the UK (24.6–67.2%, p<0.001) and to report ever having had an HIV test (68.1–86.7%, p=0.001). Men were less likely to return to their home country two or more times during their first year in the UK compared with men who had been in the UK for a year or more (39.3% vs 63.1% made at least two trips home in the previous year, p<0.001).
STI and HIV diagnosis
Almost one third of men (30.7%) reported that they had ever been diagnosed with an STI. Gonorrhoea was most commonly reported (11.1% of all respondents), followed by chlamydia (10.5%) and syphilis (7.3%) (table 3). The majority of men reported that their STI had been diagnosed in the UK (77.8% of those reporting chlamydia, 68.0% of those reporting syphilis and 56.6% of those reporting gonorrhoea). Just under 5% of men reported being HIV positive (n=32) and London men were more likely to report that they were HIV positive (5.6% vs 3.1%, p<0.001). Most HIV-positive men reported being diagnosed in the UK (78.1%). Men were asked the year of their HIV diagnosis. The majority had been diagnosed since 2004 (80.6%) and 12.9% were diagnosed in 2009 (the year of the study).
STI reported by CEE MSM and diagnosis in the UK
Unprotected anal intercourse
UAI with a casual partner was reported by 28.3% of all men in the past year, 22.8% reported UAI with a casual partner of unknown or discordant HIV status and 17.1% reported UAI with a main partner of non-concordant HIV status (no significant differences by place of residence). UAI with a casual partner of discordant or unknown HIV status was more common in men known to be HIV positive (46.9%) than HIV-negative or untested men (18.8% or 27.7%, respectively, p<0.001). In a multivariate model (table 4), UAI with a casual partner was associated with being HIV positive (vs HIV negative: aOR 0.16, p<0.001; untested: aOR 0.23, p=0.001), taking recreational drugs in the past year (aOR 2.07, p<0.001) and being paid for sex in the UK (aOR 2.20, p=0.004).
Factors associated with UAI with a casual partner
Discussion
CEE MSM in the UK are at significant risk for the acquisition and transmission of STI and HIV through UAI with non-concordant casual partners, sexual mixing and commercial sex. They were more likely to report STI diagnoses when they had been in the UK for longer and a high proportion of STI and HIV were reported as diagnosed in the UK. These findings suggest that CEE MSM are at greater risk following migration to the UK.
The self-reported HIV prevalence among CEE MSM was relatively low, with under 6% of CEE London men reporting that they were HIV positive compared with 11% of men in a similarly recruited web sample of London gay men9 and 12% in a community survey of London gay men conducted at the same time (D. Mercey, personal communication, 2010). However, a substantially larger proportion of new HIV diagnoses among CEE men in the UK result from sex between men compared with diagnoses among men across the CEE region.3
We found that assortative sexual mixing decreased the longer men stayed in the UK and partner numbers increased after a period of 2 years in the UK. The low prevalence of new HIV diagnoses among CEE MSM in their countries of origin4 means that assortative sexual mixing between CEE MSM is likely to be protective against STI and HIV infections. Barriers to HIV testing in CEE countries10 11 may mean that HIV is more likely to remain undiagnosed among MSM in CEE countries compared with the UK, but the high prevalence of HIV among MSM in the UK is likely to increase exposure to infection when CEE men have partnerships with men who are not from their home country. By comparison, the majority of heterosexual CEE migrants report that their most recent partner was from their home country (F.M. Burns, manuscript in preparation). It is possible that CEE MSM seek out partners from other countries in response to the homophobia in their home countries. Whatever the mechanisms, sexual mixing requires continued monitoring to clarify its role in the acquisition and transmission of HIV and STI.
Our findings suggest that CEE MSM report comparable levels of risk to those in the general MSM population in London and the UK. Nearly one third of CEE MSM in London reported UAI with a casual partner in the past year compared with one quarter of gay men in a community sample in London (D. Mercey, personal communication, 2010). CEE MSM throughout the UK reported similar amounts of UAI with a casual partner of unknown or discordant HIV status to non-concordant UAI reported in another UK sample of MSM (23% vs 26%).12
We found that the likelihood of practising non-concordant UAI with a casual partner did not change with time in the UK or place of residence. Limited data from CEE countries suggest that UAI is practised among a substantial proportion of MSM11 13 14 and condom use may not alter following migration to the UK. Data are needed to explore the extent to which individuals practice UAI before and after migration.
UAI with a casual partner was more likely among men who were HIV positive, had taken recreational drugs in the past year and had been paid for sex in the UK. Previous work shows that HIV-positive London men were more likely to report non-concordant UAI with casual partners than men who were of negative or unknown HIV status15; and recreational drug use is also associated with UAI.16 The association with sex work is of particular concern, given that 15% of CEE MSM in London reported that they had been paid for sex in the UK. It is possible that recruiting men through gay dating websites might have increased the number of sex workers in our sample. However, the proportion of East European men attending a clinic for male sex workers in London increased from less than 1% in the mid-1990s to 8% over the following 6–7 years,17 and numbers are likely to have increased further following EU accession. Further research is needed to understand when and how CEE MSM take up commercial sex work and the risks involved.
The primary limitation of the study is that it recruited MSM through gay websites and such samples are more likely to include men with higher levels of sexual risk behaviour than are found in the general population of MSM.18 This method of recruitment, however, has become increasingly common in behavioural surveillance among gay men, and data collected in this way therefore benefit from comparability. CEE migrants come from 10 different countries across an area of wide regional variation. The relatively small sample size of our study did not provide sufficient statistical power to analyse data at the country level. In addition, we cannot be sure that our sample represents the distribution of CEE nationalities among MSM in the UK. Not only are data on the nationality of CEE migrants to the UK incomplete, but they may not reflect the distribution of MSM from CEE countries. Finally, although a reassuringly high number of men reported that they had been tested for HIV, the study is limited by its reliance on self-report and the absence of biological samples. This should be considered in future studies.
Our findings indicate that CEE MSM are at significant risk for the acquisition and transmission of STI and HIV in the UK. This may have important implications for the cross-border transmission of infections, given the fluidity of movement among CEE MSM between their home countries and the UK. CEE MSM regularly returned to their home countries, which creates the opportunity for the transmission of infections between countries. Access to sexual health services in the UK is therefore an important factor in managing sexual health among CEE MSM both in the UK and their countries of origin. These findings are furthermore relevant to sexual health services throughout the UK, given that men living in London and elsewhere in the UK were as likely to practise UAI with a non-concordant casual partner. Interventions aimed at MSM should be accessible to CEE MSM, with information available in CEE languages if possible, and alternative strategies for health promotion and HIV/STI prevention may be important among new arrivals. In addition, culturally sensitive prevention programmes may benefit men who do not identify as gay or bisexual. The UK has a duty of care to ensure that MSM from CEE countries are aware of the sexual health services in the UK and are able to access them.
Key messages
HIV prevalence among MSM in CEE countries is much lower than among MSM in the UK.
Following migration to the UK, CEE MSM report more STI and HIV diagnosed in the UK than diagnosed elsewhere.
CEE MSM in the UK report high levels of risk behaviour including commercial sex and recreational drug use.
CEE MSM return regularly to their home countries and these findings have important implications for the cross-border transmission of infections.
Acknowledgments
The authors are grateful for the expert guidance provided by expert and community advisory boards. They would also like to thank GayRomeo and Gaydar for fielding the questionnaire and everyone who took part in the study. The views expressed are those of the authors and are not necessarily those of the MRC, NoCLoR or the health departments.
References
Footnotes
Funding This study was supported by the MRC Sexual Health and HIV Research Strategy Committee and the North Central London Research Consortium (NoCLoR) grant enhancement fund. The sponsors of the study had no role in the study design, collection, analysis or interpretation of the data, the writing of the report or the decision to submit the paper for publication.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Camden and Islington Community Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Behaviour
- Behaviour