Article Text

Abstract
Objectives There has been a large influx of central and east European (CEE) migrants to the UK following the expansion of the European Union. This paper examines factors associated with genitourinary medicine (GUM) clinic attendance and sexually transmitted infection (STI) diagnosis among CEE migrants in London.
Methods A survey of sexual behaviour was conducted among CEE migrants attending two central London GUM clinics (n=299) and community venues in London (n=2276). Routinely collected clinic data were also analysed.
Results CEE migrants made up 2.9% of male and 7.0% of female attendees at the clinics. Half the women attending sessions for female sex workers were from CEE countries, and paying for sex was widely reported by men. Women were more likely than men to have attended a GUM clinic in the UK (7.6% vs 4.5%, p=0.002). GUM survey respondents were more likely than community survey respondents to report one or more new sexual partners in the past year (women 67.9% vs 28.3%, p<0.001; men 75.6% vs 45.1%, p<0.001) and homosexual partnership(s) in the past 5 years (men 54.3% vs 1.8%, p<0.001), but were less likely to report assortative heterosexual mixing (women 25.9% vs 74.2%, p<0.001; men 56.5% vs 76.3%, p<0.001).
Conclusions CEE patients make up a notable minority of patients attending two central London GUM clinics. Higher numbers of sexual partners, homosexual partnerships and sexual mixing with people from outside the country of origin are associated with GUM clinic attendance. Heterosexual CEE men report behaviours associated with HIV/STI acquisition but appear to be underutilising GUM services.
- European migration
- GUM services
- health service research
- sexual behaviour
- sexual health
- STD
- UK
Statistics from Altmetric.com
On 1 May 2004, the Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Slovakia and Slovenia (Accession 8 or A8) joined the European Union (EU), followed by Romania and Bulgaria (A2) on 1 January 2007. The accession of these 10 central and east European (CEE) countries resulted in a large influx of predominantly young economic migrants to the UK. All nationals of these countries have entitlement to NHS services, and the UK has a responsibility to ensure that the health needs of these communities are met.
In a recent study of people who attended two central London genitourinary medicine (GUM) clinics, 2.2% of men and 6.6% of women were from an A8 country and the proportion of attendances by A8 men and women had increased significantly over 6 years.1 However, these data do not provide any information on sexual risk behaviour that would enhance our understanding of the sexual health service needs of people from CEE countries. While reporting GUM clinic attendance is associated with greater numbers of sexual partners, having same-sex partnerships, injecting drug use and paying for sex among those in the general British population,2 the factors lying behind GUM clinic attendance among the new CEE migrant population are unknown. Following the accession of the A2 countries, this paper examines sexual risk factors among men and women from both the A8 and A2 countries who attend sexual health services in London, as part of the Sexual Attitudes and Lifestyles of London's East Europeans (SALLEE) project.
Methods
SALLEE cross-sectional survey
A detailed description of the methodology has been published.3 A summary of the methods for the SALLEE cross-sectional survey is described below. In this paper we refer to two samples of men and women who took part in the survey—SALLEE GUM respondents and SALLEE community respondents.
Participants and procedure
Eligible respondents for both samples were literate men and women aged 18 years or over who self-identified as migrants from one of the 10 CEE countries. Eligible respondents were born or spent formative years in one of those countries. Given the fluid nature of migration, length of time in the UK was not a pre-condition for participation. The SALLEE GUM sample was recruited from the two central London GUM clinics over 9 months (1 July 2008 to 31 March 2009). Recruitment in the clinics was mainly undertaken by two members of the research team, one of whom was a native speaker of Polish and Lithuanian. The SALLEE community sample was recruited from a range of venues in London over the same period. The nine fieldworkers involved in community sample recruitment were native speakers of six of the languages of the CEE countries.
Sampling
For the SALLEE GUM sample, the days and times of recruitment in the clinics varied over the data collection period. During the times that recruitment took place, men and women who stated on their clinic registration form that they had been born in one of the 10 CEE countries were asked to participate in the study. For the SALLEE community sample, recruitment locations were selected following a detailed social mapping exercise and times of recruitment at venues were varied. Fieldworkers asked individuals where they were from before asking if they would be willing to take part in the study. The resulting community sample reflects a broad cross-section of CEE migrants in London.
Study instrument
The survey instrument was a self-completed questionnaire that was fielded using hand-held computers and included no information that would allow respondents to be identified. The questionnaire was available in 12 languages (the 10 CEE languages plus English and Russian). It was translated from English into the 11 languages and checked for accuracy by native speakers of these languages. Informed consent was sought using information sheets available in the 12 languages. A £5 high street voucher was offered as an incentive.
The questionnaire concentrated on sexual risk behaviour, including sexual practices, numbers of partnerships, use of condoms, paying for sex, sexually transmitted infection (STI) (including HIV) and the use of sexual health services. Respondents were also asked about recreational drug use. When possible, questions from previously validated questionnaires were used in order to maximise their reliability and validity. The questionnaire was piloted with nine CEE migrants to examine its feasibility and acceptability and to explore understanding of the question items and underlying constructs. The final questionnaire took approximately 10 min to complete.
Retrospective analysis of routinely collected GUM clinic data
Routinely collected data on all attendances of patients from CEE countries and elsewhere at the same two GUM clinics were analysed for the same period (1 July 2008 to 31 March 2009). We refer to these data as GUM clinic patients in order to distinguish them from the SALLEE GUM clinic respondents who participated in the cross-sectional survey. Data analysed here refer to new attendances; GUM clinic attendees who were known to be HIV positive before their visit were excluded, as were follow-up GUM clinic appointments unless they resulted in a new STI diagnosis.
Statistical analysis
Standard statistical tests such as χ2 and the Student t test were used to examine associations between factors. Logistic regression modelling was used to obtain OR and adjusted OR. Analysis was performed using SPSS version 12.0.
Results
Retrospective analysis of routinely collected GUM clinic data
This analysis of routinely collected GUM clinic data was conducted for the same period as data collection for the SALLEE project (1 July 2008 to 31 March 2009) and provides the context for our analysis of the SALLEE cross-sectional survey. A total of 29 770 GUM clinic patients attended the two clinics at least once during this time and half of them were men (48.7%). Country of origin was not recorded for 8.9% of GUM clinic patients. Of the 27 131 men and women with a known country of origin, 1373 (5.1%) were born in a CEE country: 2.9% of men and 7.0% of women.
One of the GUM clinics runs sessions specifically for female sex workers (FSW). Among the 295 patients attending these sessions, 50.2% (n=148) were from a CEE country, compared with 6.1% of female patients attending all other GUM clinic sessions. The majority of CEE women attending sessions for FSW were Romanian (44.6%), Lithuanian (25.7%) or Polish (10.8%). As the SALLEE cross-sectional survey was not administered to women attending sessions for FSW, these women are excluded from the remaining analysis of clinic data.
Overall, male GUM clinic patients were more likely than women to have one or more STI diagnoses (including HIV) during their visits (18.5% vs 13.3%, p<0.001). There was no significant difference between men from CEE countries and from the UK or elsewhere on the overall likelihood of an STI diagnosis (20.5% vs 18.5%, p=0.338). CEE women were slightly less likely to be diagnosed with an STI than women from the UK or elsewhere (11.0% vs 13.6%, p=0.032). A higher proportion of CEE men were recorded as homosexual or bisexual than men from other countries (42.8% vs 33.0%, p<0.001). Among CEE GUM clinic patients, STI diagnoses (excluding HIV) were more likely among men than women, those under 25 years old, from an A2 country and who were recorded as homosexual or bisexual (table 1). In multivariate analysis, gender and age remained statistically significant. Seven CEE GUM clinic patients (0.06% of all CEE GUM clinic patients) were diagnosed with HIV during the study period, five of whom were men recorded as homosexual or bisexual.
Factors associated with having a new STI diagnosis* among CEE patients attending two GUM clinics in London
SALLEE cross-sectional survey
A total of 299 men and women attending these clinics completed the SALLEE questionnaire. The SALLEE GUM clinic sample therefore represents 24.4% (299/1225) of all CEE GUM clinic patients who attended the clinics (excluding sessions for FSW) over the data collection period. Three hundred and twenty-five CEE GUM clinic patients were approached and 26 declined to take part, giving a response rate of 92%.
Two-thirds of SALLEE GUM clinic respondents were women (68.2%). The majority had been in the UK for more than 1 year (this was more likely among people from the A8 than from the A2; 94.5% vs 74.5%, p<0.001), and had returned home twice or more in the previous year (68.5%). SALLEE GUM clinic respondents were similar in age to the population of CEE GUM clinic patients who attended the clinics during the data collection period (27.0 vs 27.4 p=0.218; table 2), were as likely to be men (31.8% vs 31.1%, p=0.823) and the distribution of CEE nationalities was similar (p=0.167), with Poles making up approximately 40% of the total.
Background characteristics of SALLEE GUM clinic respondents compared with all CEE GUM clinic patients attending between 1 June 2008 and 31 March 2009
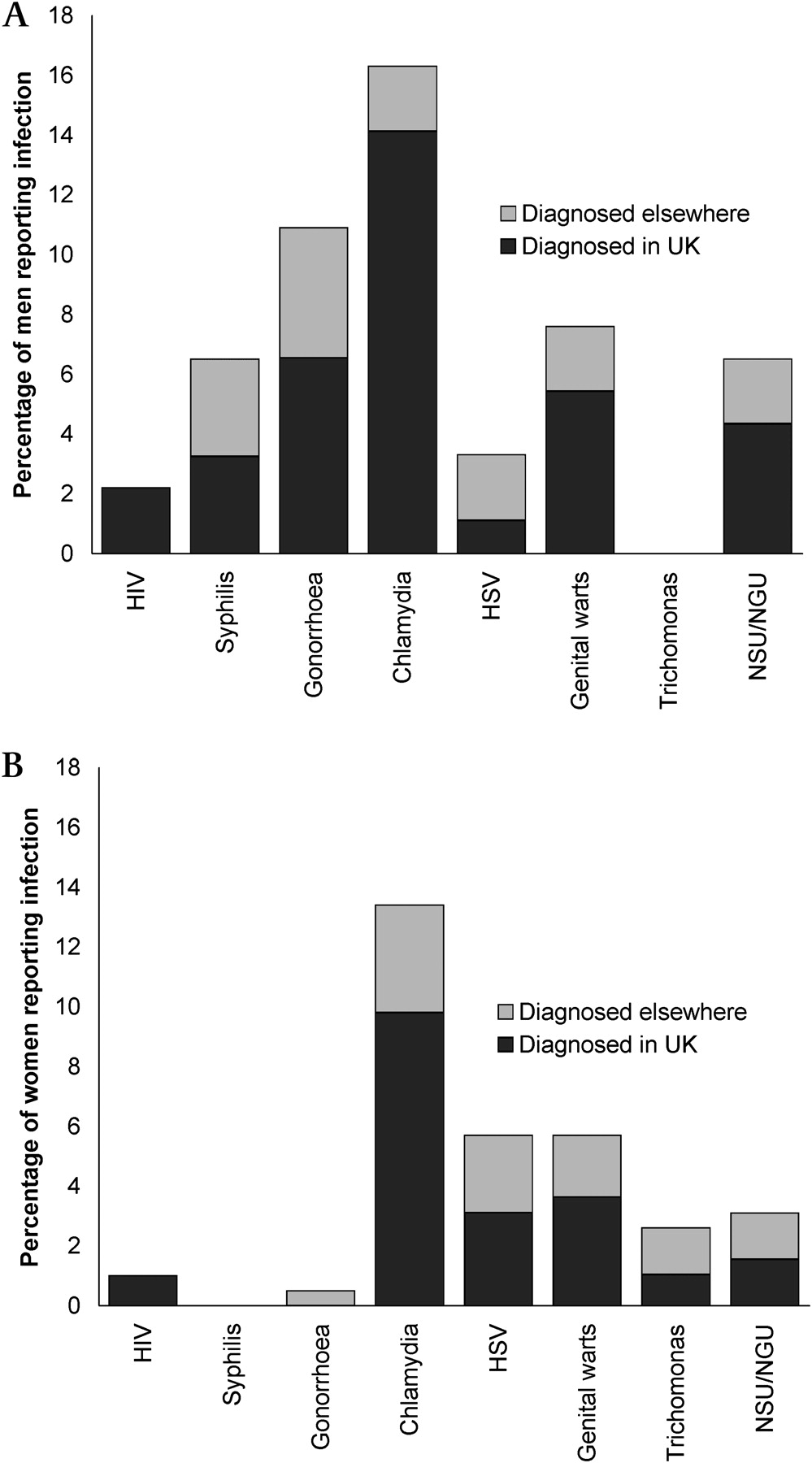
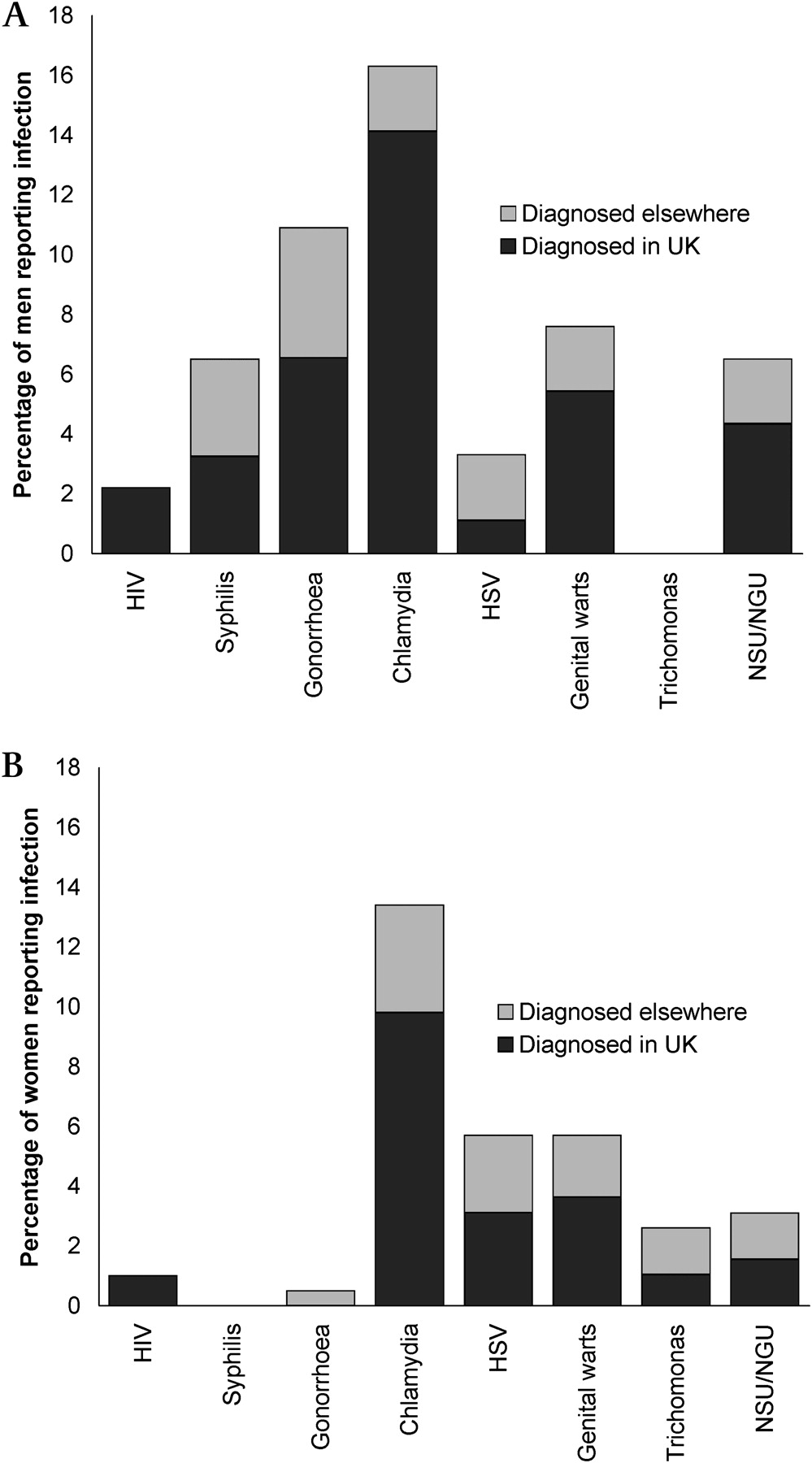
A previous STI diagnosis was reported by 38.0% of male SALLEE GUM clinic respondents and 41.2% of women (p=0.607). HIV-positive status was reported by 2.2% of men (2/93) and 1.0% of women (2/195). All HIV-positive respondents had been diagnosed in the UK, and the majority of previous STI diagnoses had been made in the UK (figure 1A and 1B).
{kind=link}
(A) Previous sexually transmitted infection (STI) diagnoses reported by the male Sexual Attitudes and Lifestyles of London's East Europeans (SALLEE) genitourinary medicine (GUM) clinic respondents, by country of diagnosis. (B) Previous STI diagnoses reported by female SALLEE GUM clinic respondents, by country of diagnosis. HSV, herpes simplex virus; NGU, non-gonococcal urethritis; NSU, non-specific urethritis.
Comparing SALLEE GUM clinic and SALLEE community samples
In order to explore the factors that may lie behind attendance at the GUM clinic, we examined differences between the SALLEE GUM clinic and the SALLEE community samples (table 3). Women in the SALLEE community sample were more likely than men to have attended a GUM clinic in the UK (7.6% vs 4.5%, p=0.002). In comparison with community respondents, male and female GUM clinic respondents were younger, more educated and had been in the UK for longer. They were less likely to be married or cohabiting. Female GUM clinic respondents were more likely to be working than their community counterparts.
Background characteristics and sexual risk behaviour among SALLEE respondents, by gender and sample
Overall, SALLEE GUM clinic respondents were substantially more likely than community respondents to report at least one new sexual partner in the past year (women 67.9% vs 28.3%, p<0.001; men 75.6% vs 45.1%, p<0.001). Although male community respondents were more likely to report one or more new heterosexual partners than their GUM clinic counterparts (44.4% vs 31.5%, p=0.017), SALLEE GUM clinic respondents were more likely than community respondents to report one or more homosexual partners in the past 5 years and the difference was particularly marked among men (54.3% vs 1.8%, p<0.001).
Community men were more likely to report consistent heterosexual condom use than GUM clinic men (38.7% vs 13.5%, p=0.002) but there was no difference in the consistency of condom use between women in the two samples (28.4% vs 29.9%, p=0.716). Community men were also more likely to have paid for sex with a woman (35.2% vs 24.3%, p=0.063). Among men reporting male sexual partners, however, there was no difference between the samples on ever paying for sex with a man (13.5% vs 12.0%, p=0.858). Three-quarters of female and male community respondents reported assortative heterosexual sexual mixing (whereby their most recent partner was from their home country), compared with 25.9% of female GUM clinic respondents and 56.5% of male GUM clinic respondents (p<0.001 for female and male comparisons). GUM clinic men were much less likely than community men to report a most recent male partner from their home country (9.6% vs 58.3%, p<0.001).
Male and female SALLEE GUM clinic respondents were more likely than community respondents to report a previous STI diagnosis, being paid for sex in the UK and recreational drug use (all p<0.01). There were no differences between the samples on injecting drug use.
In logistic regression analysis adjusting for background characteristics (age, work status, education, relationship status, time in the UK, country of birth), all significant associations between the sample and the sexual risk behaviours listed in table 3 remained significant (at p<0.001 among women and p<0.01 among men). The only exception was recreational drug use among men, with an adjusted OR of 1.55 (p=0.063).
Discussion
CEE patients make up a notable minority of patients in two central London GUM clinics. Previous patient data from these GUM clinics (May 2006–April 2007) showed that 2.2% of men and 6.6% of women were from an A8 country.1 In this paper, we included men and women from the two CEE countries that joined the EU in January 2007, giving them entitlement to NHS services, and found that CEE men now make up 2.9% and CEE women make up 7.0% of patients.
The key factors associated with having a new STI diagnosis among CEE patients were gender and age. Surveillance data from the UK as a whole also show that people under 25 years of age are disproportionately affected by STI.4 A previous STI was reported by 40% of SALLEE GUM clinic respondents, which is consistent with data from the broader population of people attending GUM clinics in Britain. One third of men and 40% of women who had attended a GUM clinic in Britain reported a previous STI diagnosis,2 as did 41% of those attending one of the GUM clinics included in the present study.5
Half of the women attending GUM clinic sessions for FSW were from CEE countries and almost half of these were Romanian. While sessions specifically for sex workers were excluded from our analysis, sex workers attending general GUM clinics may have contributed towards increased new STI diagnoses among people from A2 countries. As a newer migrant population, people from A2 countries may be more likely to use GUM services only if they have a suspected STI, whereas A8 patients might be more likely to come for a sexual health check. We are unable to test these hypotheses as data on sex work and time in the UK are not routinely collected.
CEE men who have sex with men (MSM) appear to be more likely to access GUM services than their heterosexual counterparts. Male CEE patients were more likely to be recorded as homosexual or bisexual than men from other countries. Homosexuality is no longer a criminal offence in CEE countries, but stigmatisation and discrimination are widely reported in the region,6 7 which may encourage higher levels of migration among CEE MSM compared to the CEE population as a whole.
Data collected from SALLEE respondents suggest that GUM clinic patients have an increased risk due to a higher turnover of sexual partners, more homosexual partnerships among men and commercial sex. This is consistent with data showing that increased partner numbers and same-sex partnerships are more commonly reported among people who have attended GUM clinics across Britain.2 Levels of consistent condom use were similar for women across both samples, but the higher turnover of sexual partners among GUM clinic respondents is likely to put them at greater risk for the acquisition and transmission of STI. Recreational drug use, which was highest among male GUM clinic respondents, was found to be substantially higher among MSM compared with heterosexual men and women at a London HIV testing clinic.8 Interestingly, male SALLEE GUM clinic respondents were less likely to have paid for sex with a woman than men in the community, whereas paying for sex is associated with GUM clinic attendance in Britain.2 GUM services may not be reaching all CEE men who are at risk for STI.
A major point of concern is that all self-reported HIV and the majority of previous STI among SALLEE respondents had been diagnosed in the UK. We cannot rule out the possibility that infections went undiagnosed in their countries of origin or the impact of an age effect unrelated to migration on sexual risk behaviours among this group of young migrants. However, other factors are likely to have played a part. First, migration has been identified as an independent risk factor for HIV.9 These CEE migrants have taken a risk in coming to the UK and it is thought that such risk-taking may filter through to other areas of their lives.10 Second, the sexual norms in the UK may be less limiting than in their countries of origin. Third, data suggest that the incidence of STI may be higher in the UK than in CEE countries: notification rates of gonorrhoea and chlamydia are higher in the UK than in CEE countries, and the UK is only exceeded in new HIV diagnoses by Estonia and Latvia.11 It also has the highest rate of newly diagnosed cases of HIV infection among MSM in Europe.12 SALLEE GUM clinic respondents were much less likely to report assortative sexual mixing than men and women in the community and this may have increased their risk for the acquisition of STI.
A key limitation of our study is that we did not link data from the cross-sectional survey to clinic records, which means that we are unable to look at the association between reported sexual behaviour and a new STI diagnosis. We wanted to assure respondents of anonymity and our high response rate suggests that we were successful in this respect, although other studies have found that respondents are willing to consent to linking questionnaire data to their clinic records.13 Some data were missing on nationality, although this did not vary according to whether patients were or were not diagnosed with a new STI. CEE migrants come from 10 different countries across an area of wide regional variation, but the small size of our study sample did not provide sufficient statistical power to analyse behavioural data at the country level. The limitations of convenience samples have been published,3 but it is reassuring that our SALLEE GUM clinic sample did not differ from the CEE GUM clinic population in age, gender or nationality. Whereas HIV-positive patients were excluded from our analysis of GUM clinic patient data, seven SALLEE GUM clinic respondents reported that they were HIV positive. However, the inclusion of HIV-positive SALLEE GUM clinic respondents provides a more complete picture of CEE migrants accessing GUM services.
These findings have important implications for the cross-border transmission of infections. Our data show that sexual mixing with people from the UK and other countries is one of the factors associated with GUM clinic attendance, a risk indicator for STI. In addition to frequent trips home, CEE migrants often stay in the UK for short but recurring periods,14 creating an opportunity for the transmission of infections between countries. Language barriers, confusion over entitlement and lack of knowledge about the services provided by GUM clinics may mean that migrants do not fully benefit from public health programmes or services. Bulgarians and Romanians may also benefit from specific targeting, given the increased likelihood of STI diagnosis among A2 GUM clinic patients and the high proportion of Romanian women at GUM clinic sessions for sex workers. CEE migrants are entitled to NHS services and the UK needs to ensure they are aware of sexual health services in the UK and are able to access them.
Key messages
The accession of 10 CEE countries has resulted in a large influx of predominantly young economic migrants to the UK.
Attendances at central London GUM services by migrants from eight of these accession countries have increased steadily over a number of years.
CEE GUM clinic attendance is associated with reporting new sexual partners, homosexual partnerships and heterosexual mixing with people from outside the home country.
CEE migrants make up a notable minority of patients at central London GUM services, but these services may be underutilised by heterosexual CEE men.
Acknowledgments
The authors are grateful for the guidance provided by the expert and community advisory boards, and for the hard work and commitment of the fieldworkers who collected the data. They would also like to thank the staff and management at the Mortimer Market Centre and the Archway Sexual Health Clinic; the many commercial, social and educational premises that facilitated recruitment for the fieldworkers; and everyone who took part in the study.
Footnotes
Funding This study was supported by the MRC Sexual Health and HIV Research Strategy Committee and the North Central London Research Consortium (NoCLoR) Grant Enhancement Fund. The sponsor of the study played no role in the study design, collection, analysis or interpretation of the data, the writing of the report or the decision to submit the paper for publication. The views expressed are those of the authors and not necessarily those of the MRC, NoCLoR or the health departments.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Camden and Islington Community Research Ethics Committee (07/H0722/110).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Behaviour
- Behaviour