Article Text

Abstract
Objectives To compare different ways of measuring partner notification (PN) outcomes with published audit standards, examine variability between clinics and examine factors contributing to variation in PN outcomes in genitourinary medicine (GUM) clinics in the UK.
Methods Reanalysis of the 2007 BASHH national chlamydia audit. The primary outcome was the number of partners per index case tested for chlamydia, as verified by a healthcare worker or, if missing, reported by the patient. Control charts were used to examine variation between clinics considering missing values as zero or excluding missing values. Hierarchical logistic regression was used to investigate factors contributing to variation in outcomes.
Results Data from 4616 individuals in 169 genitourinary medicine clinics were analysed. There was no information about the primary outcome in 41% of records. The mean number of partners tested for chlamydia ranged from 0 to 1.5 per index case per clinic. The median across all clinics was 0.47 when missing values were assumed to be zero and 0.92 per index case when missing values were excluded. Men who have sex with men were less likely than heterosexual men and patients with symptoms (4-week look-back period) were less likely than asymptomatic patients (6-month look-back) to report having one or more partners tested for chlamydia. There was no association between the primary outcome and the type of the health professional giving the PN advice.
Conclusions The completeness of PN outcomes recorded in clinical notes needs to improve. Further research is needed to identify auditable measures that are associated with successful PN that prevents repeated chlamydia in index cases.
- Chlamydia infections
- contact tracing
- quality of healthcare
- clinical audit
- outcome assessment (healthcare)
- audit
- Chlamydia trachomatis
- contact tracing
- health advice
- health services research
Statistics from Altmetric.com
- Chlamydia infections
- contact tracing
- quality of healthcare
- clinical audit
- outcome assessment (healthcare)
- audit
- Chlamydia trachomatis
- contact tracing
- health advice
- health services research
Introduction
Partner notification (PN) is an essential component of comprehensive case management for sexually transmitted infections (STIs).1 PN involves, where possible, providing the sexual partner(s) of people with diagnosed STI with information about the risk of possible exposure to infection; offering investigation, treatment and advice about avoiding future infection and completing documentation of this process.2 Fear of stigmatisation or judgemental attitudes are barriers to communication1 that contribute to difficulties in undertaking PN for both healthcare practitioners and patients. It is often not possible to reach all sex partners of a person with an STI, but it is important to attempt this to maximise the benefits of infection control for individuals, for partnerships (by preventing reinfection from untreated partners) and for the population (by breaking chains of transmission).
In 2007, the British Association for Sexual Health and HIV (BASHH) carried out a national audit of case note documentation of chlamydial infection management, including PN outcomes.3–5 The audit showed that the average number of contacts screened per index case was 0.3 for clinics in the London regions (North and South Thames) and 0.5 for clinics outside these areas. These levels were lower than the standards set for genitourinary medicine (GUM) clinics in 20046 and included in the most recent BASHH National Guideline,7 which were derived from a review of published and unpublished audit reports from 1995 to 2002. An observed geographical difference in outcomes resulted in different standards for clinics in London (0.4 contacts per index case screened for chlamydia) and outside London (0.6 contacts per index case). A limitation of the original review was that outcomes were not consistently defined or analysed.6 The 2007 BASHH audit requested information from all GUM clinics in a uniform format and also collected clinic-level information about policies that might affect PN.3–5 These data therefore allow sources of variation in PN outcomes across and between UK GUM clinics to be examined. The objectives of this study were to compare different ways of measuring outcomes for PN with the published standards, to examine variability between clinics and to examine factors at the individual and clinic level that contribute to variation in PN outcomes.
Methods
We analysed data extracted from case notes of patients seen between 2 January and 31 March 2007 and responses about clinic-level policies relating to PN. Detailed descriptions of the audit methods and responses to each questionnaire item have been published.3–5
Individual-level characteristics
We considered four characteristics: sex/sexual orientation of the index case (‘male heterosexuals’, ‘men who have sex with men’ (MSM) and ‘females’, which included all women irrespective of sexual orientation), age group (18 or less, 19–24, 25–34 or 35+ years), ethnic group (‘White’, ‘Black African’, ‘Black Caribbean/Black other’, ‘other’ and ‘not documented’) and documentation of index case symptoms at baseline, which included urethral discharge, dysuria, post-coital or intermenstrual bleeding, lower abdominal pain, vaginal discharge, rectal symptoms, pharyngeal symptoms or chlamydial conjunctivitis.
We did not calculate the total number of partners reported by index cases because different look-back periods (in accordance with guidance from the Society of Sexual Health Advisers2) were used in the audit questionnaire for patients who were symptomatic (number of partners in the past 4 weeks) or asymptomatic (past 6 months) at presentation.
Clinic-level characteristics
We used data about the number of chlamydia episodes reported by each clinic during the 3-month data collection period as an approximation of workload and the type of health professional providing PN advice (‘health adviser only’; ‘health adviser, doctor or nurse’ or ‘any health professional’). Information about the main method of PN used by each clinic, such as patient or provider referral, was not collected.
Outcome variables
There were three possible measures of PN outcome for each clinic: the number of partners per index case who were tested for chlamydia (abbreviated as ‘tested’), the number of partners per index case with a positive chlamydia test (‘tested positive’) and the number of partners per index case treated (‘treated’). The possible responses were 0, 1, 2, 3, 4, 5–10, >10 partners or missing (not known, not documented or not applicable). We assigned all values in the category ‘5–10’ as 5 partners and ‘>10’ as 10 partners. Whereas the BASHH audit collected and reported outcomes based on the numbers of these contacts ‘reported by index patient’ and ‘verified by a healthcare worker’,4 the primary outcome for this study was the number of partners per index case tested for chlamydia, as verified by a healthcare worker or, if information about verification was missing, as reported by the patient.
Statistical analysis
We merged datasets from the patient and clinic-level databases, using the name of the clinic. All analyses were performed using Stata 10.1.8 We first examined the measure of agreement between numbers of partners per index case with each outcome as verified by a healthcare worker and as reported by the index patient. We used the κ statistic9 to calculate the level of agreement between healthcare worker-verified and patient-reported outcomes. κ Values from 0.61 to 0.80 are regarded as ‘substantial’ agreement and values from 0.81 to 1.00 as ‘almost perfect’.9 Because of the substantial agreement between the two measures used in the BASHH audit (patient-reported and healthcare worker-verified), and to maximise the numbers of observations, we calculated an outcome that used the value recorded ‘as verified by a healthcare worker’ where available and replaced missing values with the response ‘reported by patient’.
To describe the variability in PN outcomes between clinics, we used a method similar to that previously described to construct Shewhart's control charts.6 10 First, for all index cases in each clinic, we calculated the mean number of partners tested per index case. We used the ‘median absolute deviation’ (MAD) method11 to calculate the median across all clinics and the control limits. The control limits are approximately the 99% confidence intervals (CIs). The MAD is defined as the median of the absolute deviations. The SD is calculated as 1.48×MAD and control limits are MAD±(3×SD). Differences in outcomes between centres that fall within the control limits are said to result from common causes that might be expected to occur within the healthcare system. Data points lying outside the control limits are said to result from special causes and such unintended variation, which is not due to random variation and is not predictable, should be investigated and controlled.10
We then examined the influence of missing contact numbers on PN outcomes. We plotted the proportion of all cases in each clinic for which there were no PN outcome data. We estimated the median and control limits for the number of partners tested per index case by assuming that if the data were missing then the number of partners tested was zero and excluding all index cases with missing data. For these analyses, we examined clinics in the Greater London area (28 clinics) and all other clinics separately. We repeated this for the outcomes ‘tested positive’ and ‘treated’.
We used a hierarchical logistic regression model12 to examine factors associated with PN outcomes at the individual and clinic level. We recoded the outcome as either zero or one or more partners tested per index case and estimated the odd ratio (OR, with 95% CIs), which takes into account the variation in outcomes between clinics. We then included all variables in a multivariable model to control for confounding. Data from patients with missing outcome data had to be excluded.
Results
We merged the data on 5032 individuals with chlamydia in 193 clinics with the clinic-level data reported by 177 GUM clinics. The merged dataset consisted of 4616 individuals in 169 GUM clinics; this excluded 23 clinics with 415 index cases for which there was no information about clinical policies and one clinic with only one index case for whom there were no data for any outcome of interest. The demographic characteristics of excluded index cases were comparable with those of included patients (results not shown). Excluded clinics were distributed across the country and were more likely to have audited <30 case records than included clinics. The percentages of patients for whom there was no information about the outcome of PN were partners tested for chlamydia, 41%; partners with a positive test for chlamydia, 43%; partners treated for chlamydia, 32% (table 1). The number treated exceeds the number tested because some patients will be treated ‘epidemiologically’, that is, treated because they have been in contact with chlamydia.
Numbers of patients and agreement between healthcare worker-verified and patient-reported outcomes
Comparing healthcare worker-verified and patient-reported outcomes
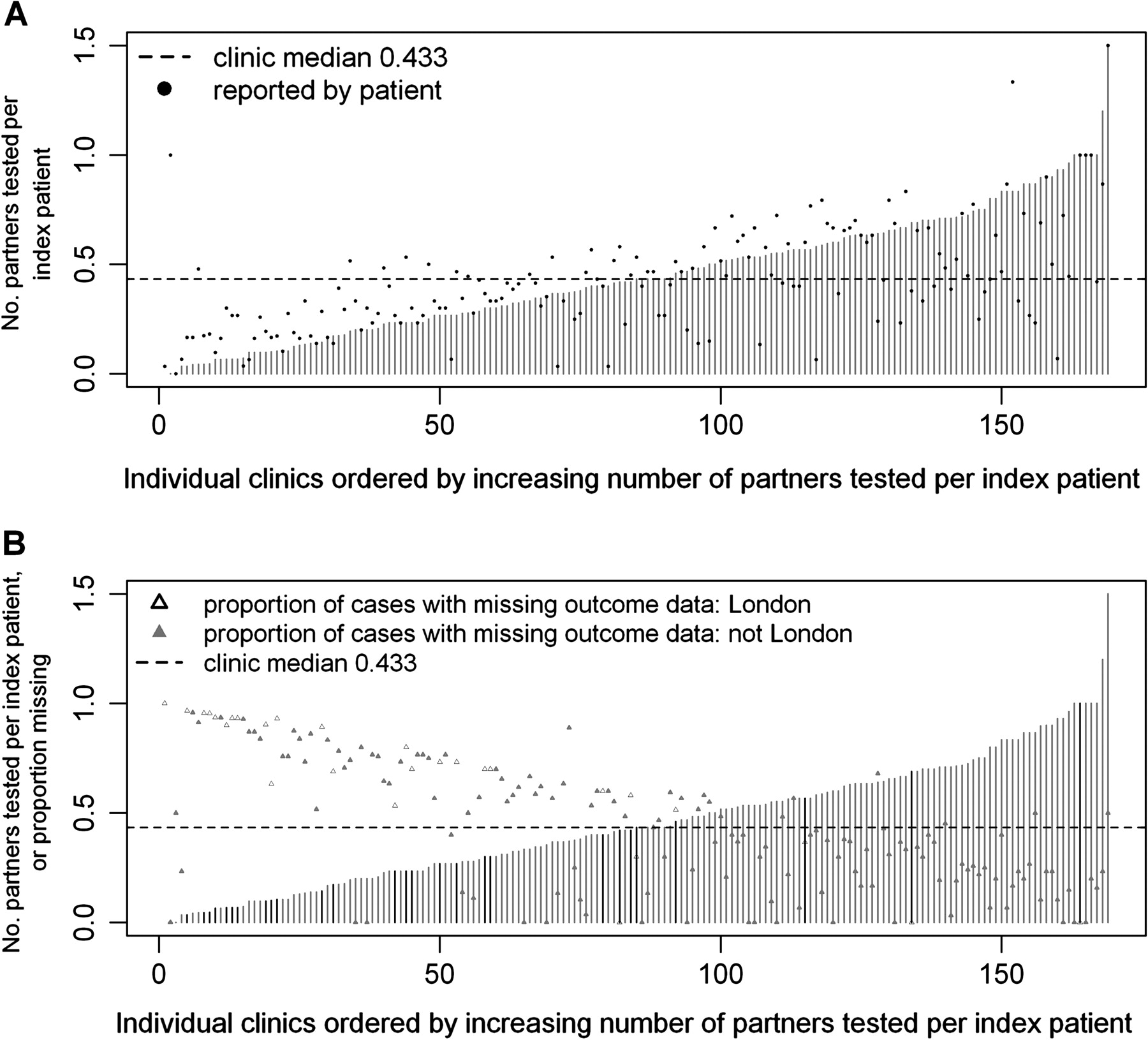
The observed κ values indicate substantial agreement between healthcare worker-verified and patient-reported outcomes given that there were seven categories for the numbers of partners (table 1). Figure 1A shows that the mean number of partners tested for chlamydia in each clinic, as verified by a healthcare worker, ranged from 0 per index case (based on 1 patient) to 1.5 (based on 60 patients). The mean values, as reported by the index case, had the same range and showed a generally good level of agreement, but the ordering of the clinics would be different if the patient-reported values were taken as the primary outcome. The median number of partners tested per index case over all clinical mean values was 0.43 when all index cases were included in the denominator for the calculation of the mean, and the number of tested partners was assumed to be zero if outcome data, as verified by a healthcare worker, were missing. Figure 1B shows the proportion of index cases in each clinic with missing data. There was a strong inverse relationship between the recorded outcome and the proportion of patients with missing data. The 28 GUM clinics in London had high proportions of records with missing outcome data. For the other reported outcomes, we observed a median over all clinical mean values of 0.33 partners per index case who tested positive for chlamydia and 0.53 partners per index case treated for chlamydia (online supplementary figures 1 and 3).
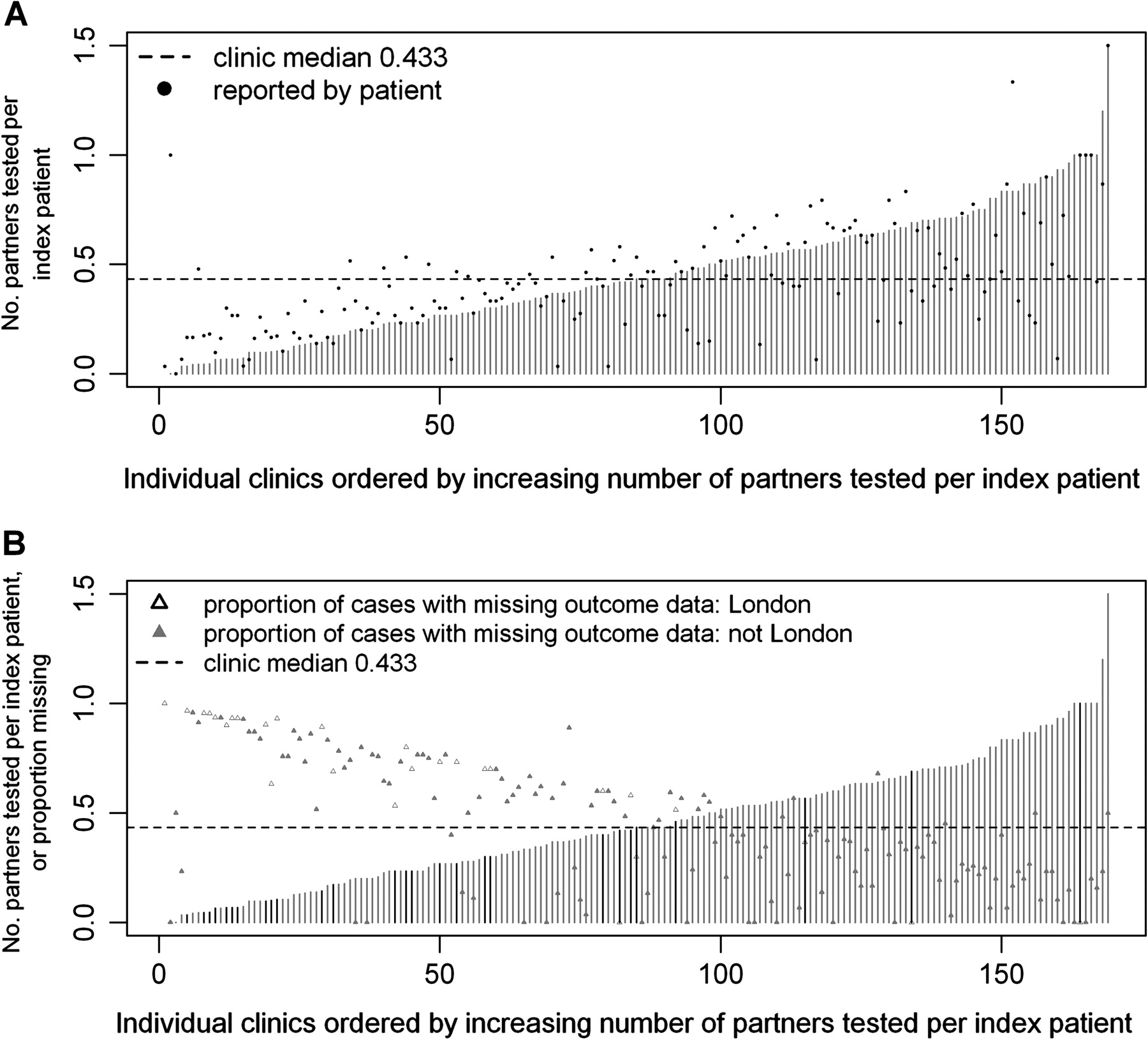
Partners tested per index case as verified by a healthcare worker; all cases included. (A) Vertical lines represent mean for each clinic for outcome as verified by a healthcare worker; filled circles represent mean for outcome for the corresponding clinic as reported by patient. Observations with missing data for outcome are coded as zero. (B) Vertical lines represent mean for each clinic for outcome as verified by a healthcare worker; triangles represent proportion of observations in each corresponding clinic with missing data about partner notification outcome.
Variability between clinics in PN outcomes
Figure 2A shows the mean number of partners tested for chlamydia per index case for each clinic, when healthcare worker-verified data were supplemented with patient-reported values. The median across all clinics was 0.47 when missing values (both healthcare worker and patient) were assumed to be zero (0.30 for Greater London GUM clinics and 0.52 for all other clinics). No GUM clinics were below the lower control limit, but most Greater London clinics were below the median. Only one clinic was above the upper control limit, suggesting that most variation resulted from common causes. When index cases with missing data were excluded from analysis (figure 2B), the median number of patients tested for chlamydia increased to 0.92 per index case (1.00 for Greater London and 0.89 for all other clinics). Using this method, there were several clinics both below and above the control limits.

{kind=link}
{kind=link}
Control chart for partners tested per index case, as verified by a healthcare worker or, if data were missing, outcome as reported by patient (combined outcome). (A) All cases included and those with missing data coded as having zero partners tested. (B) Cases with missing data excluded.
The other measures of PN outcome were the number of partners per clinic with a positive chlamydia test (median 0.37 assuming missing values as zero partners and 0.75 excluding missing values) and the number of partners per index case treated for chlamydia (median 0.60 and 0.95) (online supplementary figures 2 and 4).
Factors associated with PN outcomes
Table 2 shows associations between individual- and clinic-level characteristics and the number of partners tested for chlamydia per index case, taking into account the variability between clinics. There was no information for the clinic-level variables for 16 clinics (163 index patients); results for individual-level variables in the remaining clinics were the same as those obtained from the full merged dataset. Compared with heterosexual men, MSM were less likely to have at least one partner tested in both univariable and multivariable analyses. There was no difference in the numbers of partners tested between women and heterosexual men. There was no strong evidence of associations between the numbers of partners tested and the age or ethnic group of index cases. Index patients with symptoms at presentation were less likely to report having one or more partners tested for chlamydia than asymptomatic cases in both univariable and multivariable analyses. There was no statistical evidence of an association between the number of partners tested for chlamydia and the health professional giving the PN advice. As the number of chlamydia cases diagnosed by clinics increased, the odds of at least one partner being tested per index case increased (p value for trend 0.031); the model excludes all cases with missing data at either patient or clinic level.
Factors associated with the number of partners tested for chlamydia per index case (N=2532 cases from 153 clinics, 2084 cases with missing outcome data)
The patterns of associations for the other PN outcomes were similar to that observed for the number of partners tested for chlamydia, but there was no association with numbers of chlamydia cases diagnosed. In addition, women were less likely than heterosexual men to have a partner with a positive chlamydia test (adjusted OR 0.77, 95% CI 0.63 to 0.94).
Discussion
This study showed marked variation between GUM clinics in outcomes of PN for chlamydia, most resulting from common causes. For the primary outcome, the number of partners tested for chlamydia per index case, there were no data entered in 41% of records. There was a twofold difference in the median across all clinics in this study, depending on how missing data were dealt with. MSM were less likely than heterosexual men and patients with symptoms less likely than asymptomatic patients to have had at least one partner tested for chlamydia. In clinics diagnosing greater numbers of chlamydia cases, the odds of recording at least one partner tested for chlamydia were higher than in clinics with fewer diagnosed chlamydia cases. Findings were similar with outcomes of the number of partners with a positive chlamydia test and the number of partners treated for chlamydia.
The main strength of this study was that it included information from about 5000 patients with chlamydia in GUM clinics across the UK, although clinics auditing fewer cases were more likely to be excluded. We used a range of methods to examine different sorts of variation in PN outcomes for chlamydia at both individual and clinic levels, including the definition of the outcome (verified by a healthcare worker or reported by the index patient) and different outcomes (partners tested, partners with a positive test and partners treated). The MAD method used to examine variation between clinics is a more robust measure of statistical dispersion than the SD used in the previous analysis,6 because it does not assume that the outcome is normally distributed.11 The main limitation of the study was related to the high level of missing values for the partner outcomes. The inclusion or exclusion of these individuals from the denominator resulted in a twofold difference in calculated values for the overall median; 0.47 partners tested for chlamydia per index case when those with missing data were coded as having no partners tested and 0.92 when missing values were excluded. Differences between index cases with and without information about the outcomes of PN mean that the observed outcomes are likely to be biased, but without additional information, it is not possible to say whether these are under-reported or over-reported. A further limitation was that we were not able to make use of all of the items in the audit questionnaire because of the way in which the questions were asked.
In this study, we were able to investigate individual- and clinic-level factors influencing common causes10 of the variation in PN outcomes. MSM with chlamydia had poorer PN outcomes than heterosexual men. In The Netherlands, MSM with either gonorrhoea or chlamydia were found to have fewer partners attending a GUM clinic (0.22 per index case) than heterosexual men (0.49, p=0.056).13 MSM with gonorrhoea have previously been observed to have fewer partners tested or treated, despite reporting higher numbers of partners than heterosexual men.14 However, in a study in the USA, outcomes of PN for syphilis were similar for MSM and heterosexual men.15 Patients with symptoms also had poorer PN outcomes than asymptomatic patients. This might be related to the differing ‘look-back’ periods of 1 month for patients with symptoms and 6 months for asymptomatic patients (as recommended by the Society of Sexual Health Advisers).2 Additionally, patients with symptoms and asymptomatic patients may differ in their relationship to, and ability to contact, sexual partners, although data were not collected about these factors. Cases and clinics with missing data could not be included in the regression model so the observed association between the numbers of chlamydia cases diagnosed and PN outcomes was difficult to interpret. This finding might reflect biases for which we could not control in the analysis, if patients in larger clinics reported more partners or as a result of missing data. The pooled mean from the previous meta-analysis—0.61 (95% CI 0.55 to 0.66)6—was not stratified according to how missing values were dealt with and lies between the extremes reported in this study. The National Audit Group similarly coded missing values as zero, while counting index cases in the denominators, which led to the conclusion that the outcomes of PN for chlamydia were below the audit standard.4
It is difficult to define appropriate standards and outcomes for PN. The BASHH audit standard was based on the number of partners per index case tested for chlamydia because this was the most commonly reported outcome in UK audit studies.6 This is not a commonly reported outcome in other countries. In observational studies, the numbers of partners treated per index case or proportion of index cases with at least one partner treated are reported more often.16 None of these outcomes, however, provides information that PN has successfully treated chlamydial infection in a sex partner. The high rates of repeated chlamydial infection observed in people soon after treatment17 suggest that partners are often not contacted, not treated adequately, or information about avoiding subsequent infection has not been given or not adhered to. Further research is needed to determine the indicators of successful PN in individual case management and those that are associated with infection control at the population level. Tracing contacts back for longer than 6 months can yield a high proportion of infected contacts,18 which is efficient for case detection and management, but might not have a substantial impact on reducing chlamydia transmission in the population at large (Althaus CA, et al unpublished data 2011).
The extent to which unintended variation in clinical outcomes can and should be eliminated has been debated.10 19 20 There was a wide range in UK GUM clinics, from zero to 1.5 partners per index case tested for chlamydia. If clinics took further measures to improve their performance, this would improve both the consistency and the quality of clinical care. The findings from this audit were fed back to GUM clinics, and those falling below the control limits for the number of partners tested per index case when missing values were excluded were informed. In practice, the completeness of recording needs to improve so that levels of PN outcomes can be measured more accurately. Further research is needed to identify auditable measures that are associated with successful PN that prevents repeated chlamydial infection in index cases.
Key messages
The rate of partner notification for chlamydia in UK genitourinary medicine clinics was estimated to be about 0.5 partners tested per index case.
This has not changed appreciably since a previous analysis based on pooled data published in 2004.
Men who have sex with men were less likely than heterosexual men, and patients with symptoms were less likely than asymptomatic patients, to have one or more partners tested for chlamydia (look-back periods of 4 weeks for patients with symptoms and 6 months for asymptomatic patients).
Completeness of recording of partner notification outcomes needs to improve.
Research is needed to identify auditable measures that are associated with successful partner notification that prevents repeated chlamydial infection in index cases.
Acknowledgments
The work done by the following in supporting the BASHH 2007 Chlamydia Audit is gratefully acknowledged: all NHS staff who submitted data, NHS managers who supported the Audit, the BASHH National Audit Group Regional Chairs and officers who managed regional participation, and Hilary Curtis who produced the original national data aggregate. We thank Janneke Heijne and Christian Althaus for helpful comments on the manuscript.
References
Supplementary materials
Web Only Data sti.2011.049320
Files in this Data Supplement:
Footnotes
Funding SAH is funded by a Swiss National Science Foundation ProDoc award (PDFMP3_124952), Swiss National Science Foundation, Switzerland. This work was supported by the NIHR Health Technology Assessment programme [project number 07/42/02]. Part of this study will be published in the Health Technology Assessment journal series. Visit the HTA programme website for more details (www.hta.ac.uk/1722). The views and opinions in this article are those of the authors and do not necessarily reflect those of the Department of Health.
Correction notice This article has been corrected since it was published Online First. The final sentence of the abstract has been amended to read: Further research is needed to identify auditable measures that are associated with successful PN that prevents repeated chlamydia in index cases.
Competing interests HM and CAC are members of the National Audit Group.
Provenance and peer review Not commissioned; externally peer reviewed.