Article Text

Abstract
Objectives To analyse the effect of educational level on the progression from HIV seroconversion to highly active antiretroviral therapy (HAART) requirement, HAART initiation, AIDS and death from any cause at different periods of the HIV epidemic in Spain.
Methods Open, prospective, multicentre cohort of HIV seroconverters set up in 1983. The risk of progression was calculated by the multiple decrements method. Effect of educational level was estimated by Fine and Gray model, adjusting for sex, HIV transmission category, age and method to estimate seroconversion. Calendar period was introduced as a variable that could change over time (<1997; 1997–2003; >2003).
Results Up to 2009, 989 HIV seroconverters with information on educational level were identified. Some 52% and 48% had a low and a high educational level respectively. Persons with higher education had 32% lower risk of death (HR: 0.68; 95% CI 0.45 to 1.03). Regarding progression to AIDS, educational level had no effect in the pre-HAART era (HR: 1.47; 95% CI 0.91 to 2.38), but did show an effect in the period 1997–2003 (HR: 0.58; 95% CI 0.34 to 0.99), which was accentuated after 2004 (HR: 0.26; 95% CI 0.10 to 0.68). No difference was found in time to HAART requirement or initiation.
Conclusions Results suggest that, despite similar access to HAART, persons with low educational level are at increased risk of HIV disease progression, highlighting the impact of social inequities on health. The availability of more effective treatments over time will strengthen the protective effect of higher education on the development of AIDS.
- HIV
- AIDS
- HIV seroconversion
- disease progression
- education
- socioeconomic factors
- anteretroviral therapy
- CD4
- cervicitis
- chlamydia infection
- diagnosis
- anogenital cancer
- commercial sex
- epidemiology (general)
- ethnicity
- gender
Statistics from Altmetric.com
- HIV
- AIDS
- HIV seroconversion
- disease progression
- education
- socioeconomic factors
- anteretroviral therapy
- CD4
- cervicitis
- chlamydia infection
- diagnosis
- anogenital cancer
- commercial sex
- epidemiology (general)
- ethnicity
- gender
Introduction
The HIV epidemic in developed countries is concentrated in vulnerable groups. Although historically HIV has primarily affected injecting drug users (IDUs) and men who have sex with men (MSM), heterosexual transmission is currently the most frequent route of infection. Some of the factors that increase vulnerability are migrant status and ethnicity and low socioeconomic level.1–3 These factors cross all transmission routes and may confound or modify their effect on HIV. Highly active antiretroviral therapy (HAART) has led to a radical change in HIV prognosis,4 but there is a risk that the most vulnerable populations may be the least likely to benefit from available resources, contributing doubly to increased health inequalities.
Different variables have been used to measure social class. Educational level is one of the most widely used because it is easy to define and obtain. Despite its limitations,5 6 it has been shown to be a good approximation, especially with regard to psychosocial and behavioural factors associated with social class.7 8 It also has the advantage of being relatively stable, whereas others, such as employment status, are more likely to change over time. Low educational level has consistently been associated with higher mortality, both overall and cause-specific.9–12
Few studies have examined the effect of educational level on HIV progression; all were conducted before 1999 and on seroprevalent subjects. Studies of seroconverters are the best way to investigate the natural history of HIV,13 but no studies have been conducted to specifically estimate the effect of education on HIV progression or on HAART prescription.
Our hypothesis is that low educational level accelerates HIV progression to AIDS and death and delays HAART prescription. As the effect of education may vary at different times and places, our objective was to estimate the effect of educational level on these events at different periods of the HIV epidemic between 1983 and 2009 in a cohort of seroconverters in Spain.
Methods
We analysed data from the Spanish Multicenter Study Group of Seroconverters (Spanish acronym, GEMES), an open, prospective, multicentre cohort of HIV positive subjects with a known date of seroconversion, made up of six cohorts recruited in outpatient clinics located in Madrid, Valencia, Barcelona, Badalona and Navarre. This study received ethical approval from the Carlos III Health Institute ethical committee. A seroconverter was defined as a patient with a documented negative HIV test in the 3 years before the first confirmed HIV diagnosis. Date of seroconversion was estimated as the mean point between the two tests. Persons in whom seroconversion could be confirmed by laboratory criteria were also included. Patients were followed up according to clinical practice with a collection of clinical, laboratory and treatment variables, as well as epidemiological and sociodemographic characteristics.
The characteristics of the sample were described and non-parametric tests were applied to evaluate clinical and sociodemographic differences by educational level. Educational level was measured at cohort entry in four categories and was grouped into two levels for this analysis: persons with a low educational level (no education or only primary education completed) and persons with a high educational level (secondary or university studies completed). Due to the low number of subjects with heterosexual transmission, the transmission category was grouped into two mutually exclusive categories: IDU and sexual (including heterosexual, MSM and unknown route). Data on CD4 levels and viral load at diagnosis, sex and age at time of seroconversion, patient's region of origin, and the method used to estimate the date of seroconversion were collected. Region of origin could not be introduced in the analysis as there were too few subjects to create meaningful groups that could adequately account for the heterogeneity of the migrant population in Spain. No adjustment was made for CD4 and viral load to avoid overadjustment.
Follow-up was divided into three periods that reflected the different availability and changes in HAART recommendations (up to 1996; from 1997 to 2003; from 2004 onwards) and was introduced as a time-dependent covariable. Accordingly, each patient contributed to the analyses with as many registers as periods at risk he/she contributed to the study, and patients with an equal duration of infection were compared for each period.14
Survival analysis was conducted taking the time of seroconversion as the risk origin, but with delayed entry to the time of the first positive diagnosis in the recruitment centre to eliminate possible survival bias, which would underestimate the incidence rate by eliminating rapid progressors.15 We analysed the risk of progression to AIDS, death and HAART initiation and HAART requirement, defined as the time until a patient reached a CD4 count under 350 or developed an AIDS defining condition.
Patients were cross-matched with the National Registry of AIDS cases in the year 2004. Patients not appearing in the registry were considered AIDS-free as of 31 December 2002, leaving two washout years to correct for reporting delays.15 For dates after the cross-match, only AIDS events occurring during clinical follow-up were registered, and those lost to follow-up were censored and considered AIDS-free on the last date they had been seen. To evaluate the risk of progression to AIDS, death was considered as a competing event; therefore, the cumulative incidence function was estimated by the multiple decrements method,16 an extension of the Kaplan–Meier method. To evaluate the effect of educational level on the risk of AIDS we used the Fine and Gray method,17 an extension of the Cox proportional hazards model, which models the subdistribution of the risk of competing events and estimates the so-called sub-HR.18
Three of the six cohorts that constitute GEMES were cross-matched with the mortality register of the National Statistics Institute: two by 2006 and one by 2008. Subjects not recorded as deceased in the registers were considered alive until 2 years before the date of the cross-match. After the cross-match, and for cohorts not cross-matched, losses to follow-up were censored and considered alive on the date of their last visit. The cumulative incidence function was calculated using the Kaplan–Meier method. To evaluate the effect of educational level on the risk of death, we used Cox's proportional hazards model to estimate the HRs.
For the analysis of time to requirement of HAART and time to HAART initiation, we restricted to persons seroconverting after 1996, time at which HAART became universally available in Spain, and each individual was censored on the date of the last visit. Death was considered as a competing event, and the multiple decrements method and the Fine and Gray model were used.
The association between the exposure of interest, ‘educational level’ and the various outcomes was examined in crude analyses and step-forward modelling was carried out to evaluate confounding; we retained variables that changed at least 10% the value of the HR as of interest. Robust methods were used for SE estimation, and statistical significance was evaluated using the Wald test. All the analyses were conducted using Stata software (V.11.1, Stata Corporation, College Station, Texas, USA).
Results
For the period between 29 April 1983 and 26 February 2009, 1772 patients were included in the cohort, with a median seroconversion date of 25 December 1994 (IQR): 21 July 1991—4 December 1999. The median seroconversion window (time between the last negative and first positive tests) was 1.0 years (IQR: 0.6–1.7). A total of 783 (44.2%) patients did not have information on educational level and were excluded and 67.4% of them corresponded to IDUs from a prison cohort and a detoxification unit. Compared with those with available information, they were younger, there was a higher proportion of IDUs, women and people with missing region of origin, had been recruited in early calendar periods, had been imprisoned in their life-time and had lower CD4 counts at entry. The sample for the final analysis consisted of 989 persons.
Of these, 9.7% had not completed primary education, 42.4% had competed primary education, 28.8% had completed secondary education and 19.1% had completed higher than secondary education. In all, 515 subjects (52.1%) were included in the category of low education and 474 (47.9%) in the category of high education. Some 52.4% were IDUs, and the rest of the sample was composed of MSM (85.1%) and heterosexuals (11.7%), with a small proportion (3.2%) of unknowns. Table 1 shows a description of these groups by educational level and calendar period. The low education group was composed mostly of IDUs, had more women and young people and fewer foreigners than the high education group. In more recent calendar periods, patients had higher education, were older, more likely to be foreigners and acquired the infection by sexual transmission. No differences were detected with regard to CD4 or viral load at the time of diagnosis by educational level, except in the first study period.
Sociodemographic and clinical characteristics by educational level
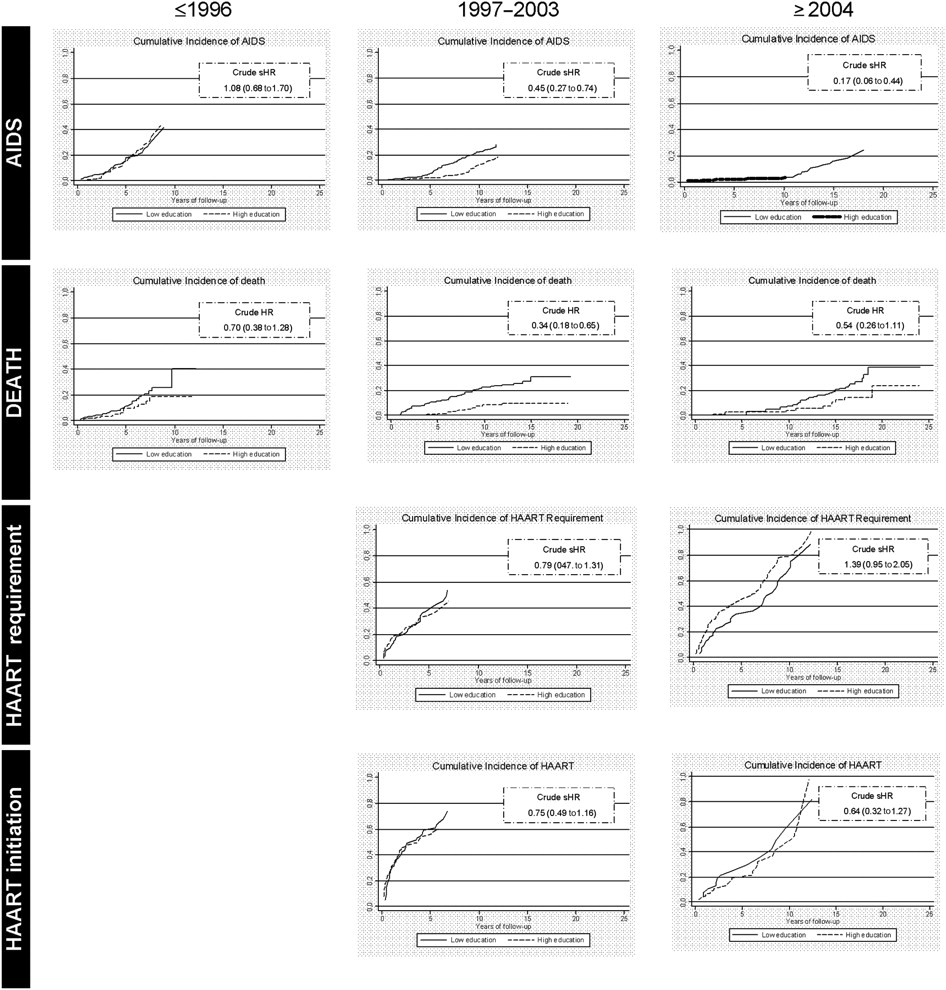
In the analysis of time to AIDS, 203 events were produced over 6783.1 person-years. The incidence rate was 37.7 per 1000 (95% CI 32.1 to 44.2) in persons with low education versus 18.9 per 1000 (95% CI 14.4 to 24.7) in those with high education. Figure 1 shows the cumulative incidence function by educational level for each period. The risk of AIDS decreases in each period and the protective effect of educational level increases. In adjusted analysis, transmission route and calendar period were confounding variables, with a notable change in the crude HR observed after adjusting for these variables. A significant interaction was detected between educational level and period, so that no effect was observed before 1996, but between 1997 and 2003, persons with high education had a 42% lower risk of AIDS (95% CI 1% to 46%); this effect was larger for the period beginning in 2004 (74% lower, 95% CI 32 to 90%; table 2). No significant interaction was found with transmission category.
{kind=link}
Cumulative incidence functions for AIDS, death and HAART, by educational level and period. HAART, highly active antiretroviral therapy.
Adjusted effect of high educational level on each of the events
There were 164 deaths over 8432.8 person-years. The incidence rate was 25.0 per 1000 (95% CI 21.0 to 30.0) in persons with low education and 10.9 per 1000 (95% CI 7.9 to 15.1) in those with high education. Figure 1 shows that the cumulative incidence of death in each period tends to be lower for persons with high education in all periods. After adjusting for confounding variables—transmission rate and age at seroconversion—persons with high education had a 32% lower risk of death (95% CI 55% lower to 3% higher), a result of borderline statistical significance (table 2).
Analysis of time to HAART was restricted to those persons seroconverting after 1996, a total of 435. There were 186 patients who fulfilled criteria of HAART requirement and 122 initiated HAART during 1149.8 and 914.8 person-years of follow-up, respectively. Figure 1 shows no crude effect in HAART requirement or initiation by period and educational level. After adjusting for transmission route and calendar period, no effect of educational level was seen in any of the two HAART outcomes and no interaction was found (table 2).
Other censoring strategies and alternative ways of handling competing deaths, or censoring at the end of the calendar period in which death took place, did not substantially change the results (data not shown).
Discussion
Educational level is a determinant of progression to AIDS and death, but not to HAART requirement or initiation. In the early stages of the epidemic no differences by educational level are seen in progression to AIDS but after 1996, the time when HAART appeared, higher educational level becomes a protective factor, an effect that is accentuated after 2004. In the case of progression to death, higher educational level also tends to be a protective factor, reducing the risk by 32%.
The different effect of educational level on progression to AIDS in the various calendar periods shows that, in the absence of effective therapeutic resources, education does not determine prognosis in HIV-infected persons, but as effective treatments become available, those with lower education benefit to a smaller extent. These results corroborate what has been previously found in Spain,19 but differ from what has been reported in other countries, although no study has used data after 1999 and none was performed in seroconverters: the ideal group to study natural history. Schechter et al20 observed different progression to AIDS by socioeconomic level before HAART times, whereas Junghans et al21 did not find these differences in the years after HAART. The effect of educational level may vary from one country to another.
Our study, as other publications, supports the hypothesis that persons with lower education have a higher risk of death. Several studies in Spain have shown a greater risk of death in the general population associated with a low educational level, and have attributed the differences in the younger groups to infectious diseases and, specifically, HIV/AIDS.12 22 Jarrín et al23 found a protective effect of educational level on mortality from all causes in IDUs after HAART availability, and a study in British Columbia (Canada),24 where access to HAART is free and universal, found that persons with a lower socioeconomic level had a higher mortality from HIV, a finding that has also been observed in other studies in Spain.25 26
The effect of educational level on mortality was the same in all three calendar periods in our study, independent of the availability of HAART, which suggests the existence of other determinants of inequality besides HIV infection. Many causes of death, like overdose or external causes, are not affected by HAART; in fact, 23% of the deaths in our study were due to these causes. Attributing a death to HIV is complex, and a high degree of misclassification must be assumed, especially with regard to causes categorised as infectious diseases or tumours. Partly because of this limitation, and partly due to the small sample size, we did not specifically analyse the risk of death attributable to HIV.
Time to HAART initiation showed no difference by educational level, as no difference was found in time to HAART requirement, suggesting there is equal access to treatment. This is to be expected in a health system with free, universal coverage, as is the case in Spain. Other studies however, some of them in similar contexts, have found differences in access according to socioeconomic level.12 21 It is possible that in our cohort we did not capture the most marginalised persons who may not have had access to the health system. Thus, the lack of differences in our study population does not rule out the possibility that such differences may exist in population subgroups that were not represented in our seroconverter sample.
The different progression to AIDS and death in our study could not, in principle, be attributed to marked differences in access to HAART. But it may be that the effectiveness of HAART depends on educational level, because of either poor adherence or worse response to treatment. A recent systematic review found that less than one-third of studies had shown a statistically significant association between educational level and adherence.27 On the other hand, some studies that have directly evaluated the virological, clinical and immunological responses to HAART have found lower effectiveness in persons with less education,28 even after adjusting for adherence to treatment;29 therefore, other factors may be implicated.
Some hypotheses of why educational level could affect risk of AIDS and death without affecting HAART access could be different life conditions and health behaviours, nutritional factors,20 the ability to understand and accept the disease, different attitudes towards prophylaxis or other social and psychological resources that make it possible to confront stressful life situations with success.12 A higher comorbidity in the low education group could also play a role, although adjusting for hepatitis C virus and hepatitis B virus co-infection in the subset of patients with this information did not modify the results.
The results of our study should be interpreted in light of its limitations. Educational level was recorded at the time of recruitment, which could lead to classification bias, since some subjects may have completed higher-level studies during follow-up. However, the change in category would occur in subjects who completed secondary education after recruitment, which is uncommon in an adult cohort. Moreover, this bias would work in favour of the null hypothesis; therefore, it is unlikely to explain our results. Selection bias could have been introduced by the exclusion of those with no information on educational level. Most were young patients infected in the early epidemic through IDUs, probably of Spanish origin, who had been imprisoned in their life-time and had lower CD4 count at diagnosis; a high proportion of them probably correspond to people with a low educational level. Because of the poorer prognostic factors, we can assume the direction of this selection bias, if existing, would also be towards the null. However, no differences were found in time to AIDS or death between people with or without information on educational level.
Another limitation stems from having combined MSM and cases of heterosexual transmission into a single category as they have different demographic and socioeconomic characteristics. In Spain, some of the heterosexual cases are partners of IDUs, with whom they share other determinants, among them, a lower educational level than MSM. The heterosexual group is difficult to capture among the seroconverters, since they have a lower perceived risk of infection and do not undergo repeated HIV tests. In addition, the sociodemographic profile of HIV patients has changed throughout the calendar periods, so we cannot rule out the possibility that changes in non-measured variables could partially explain our results.
Finally, the assumption that mortality and AIDS registers are complete and that persons who do not appear in them are event-free may lead to an underestimation of the incidence rate, but there is no reason to think this would differ by educational level. However, censoring those lost to follow-up on the date they were last seen can be problematic, since people with a slower disease progression tend to miss follow-up visits while those with a faster disease progression and who experience the event would be over-represented.15
Our study provides important evidence on the role of educational level on the progression of HIV infection and shows the need to take this factor into account, at the clinical care stage and from the perspective of health programmes and policies.
Key messages
Although highly active antiretroviral therapy (HAART) has reduced the risk of AIDS and death at a population level, this study shows that socioeconomic variables entail differences in effectiveness.
People with a low educational level had a higher risk of death, and in the HAART era, especially post-2004, a higher risk of developing AIDS.
This effect does not seem to be mediated by a differential access to antiretroviral therapy in the context of a health system with universal coverage.
These results show the impact of social inequalities on health and are important with regard to clinical recommendations and to health programmes and policies.
References
Footnotes
↵* The following are members of the Spanish Multicenter Study Group of Seroconverters: Santiago Pérez-Hoyos, Inmaculada Ferreros, Julia del Amo, Cristina González, Ana María Caro, Inmaculada Jarrín, Isabel Hurtado, Josefina Belda, Elisa Fernández, Isabel Gómez, Ignacio Alastrue, Concha Santos, Teresa Tasa Zapater, Amparo Juan, Jose Trullen, Robert Muga, Arantza Sanvisens, Jorge del Romero, Paloma Raposo, Carmen Rodríguez, Soledad García, Patricia García de Olalla, Joan Cayla, Eva Masdeu, Rafael Guerrero, Manolo Quintana, Isabel Ruiz, Ramiro Nuñez, Jesús Castilla, Marcela Guevara, Carmen de Mendoza and Natalia Zahonero.
Funding This work was supported by FIPSE (Fundación para la investigación y la prevención del SIDA en España, integrated by the Spanish Ministry of Health, Abbott Laboratories, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Merck Sharp and Dohme and Roche). This work is also supported by RIS (Red de Investigación de SIDA) RD06/006.
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by Instituto de Salud Carlos III.
Provenance and peer review Not commissioned; externally peer reviewed.