Article Text

Abstract
Objectives The present study investigates the varied spatial distribution of syphilis cases in Shenzhen, China, and explores the individual-, neighbourhood- and district-level factors affecting the distribution.
Methods This study uses spatial analysis and multi-level generalised estimating equations to explore the spatial distribution of reported syphilis cases among individuals in Shenzhen, Guangdong Province, China. The spatial distribution of primary/secondary and latent cases was investigated using the Moran's I-statistic. Primary/secondary syphilis cases were compared with all syphilis cases using a three-level model with individual (n=6496), neighbourhood (n=55) and district (n=6) levels.
Results A total of 6496 syphilis cases were reported in 2009 with 35.8% primary and secondary syphilis cases. Both primary/secondary syphilis cases (Moran's I value=0.33, p<0.01) and latent syphilis cases (Moran's I value=0.19, p<0.01) showed significant spatial clustering at the neighbourhood level. Adjusting for the number of reporting hospitals, the best model found that the following characteristics were associated with primary/secondary syphilis infection: individuals who are younger in age (p=0.003), male (p<0.001), migrant labourers (p=0.047) and those who live in districts with a higher gross domestic product (p<0.001).
Conclusions There is substantial clustering of primary and secondary syphilis cases at the neighbourhood level in Shenzhen, suggesting the need for greater STD health service provision in these clustered neighbourhoods. Spatially targeted syphilis control measures may be useful to optimise testing, treatment and partner services.
- Syphilis
- China
- neighbourhood
- spatial
- HIV
- HPV
- sexual behaviour
- syphilis
- sexual health
- AIDS
- social/policy perspectives
- social
- sociology
- STD
Statistics from Altmetric.com
- Syphilis
- China
- neighbourhood
- spatial
- HIV
- HPV
- sexual behaviour
- syphilis
- sexual health
- AIDS
- social/policy perspectives
- social
- sociology
- STD
Introduction
Syphilis has made a major resurgence in China over the past 10 years1 ,2 and has surpassed tuberculosis as the most commonly reported communicable disease in many major metropolitan areas. In 2009, Guangdong Province reported 41 syphilis cases per 100 000 people compared with 14.7 cases per 100 000 people reported in the USA. The epicenter of Guangdong Province's syphilis epidemic is within the Pearl River Delta region that has nearly half of all syphilis cases in the region.3 Shenzhen, a special economic zone, located in the southeast of Guangdong and adjacent to Hong Kong, reported more than 30 000 cases of sexually transmitted infections (STIs) in 2008, with syphilis, gonorrhoea, chlamydial infection, genital herpes and genital warts accounting for 19.1%, 19.3%, 38.1%, 16.5% and 6.9%, separately.4 Syphilis is particularly important because it increases the risk of acquiring and transmitting HIV infection. The reported incidence of syphilis in Shenzhen was 48.9 cases per 100 000 people in 2008,5 which was 2.3 times higher than China (21.1 cases per 100 000 people) and among the highest of any city in Guangdong Province. The high syphilis incidence in Shenzhen provides a unique opportunity to explore spatial and structural factors associated with a higher burden of disease.
A growing sexual health literature from China suggests the importance of specific spatial and environmental attributes in promoting STI transmission.5 ,6 Rapidly expanding entertainment centres and related sex venues have created specific local environments that may increase the likelihood of unsafe commercial sex.7 ,8 A rich anthropological and sociological literature describes densely clustered sex venues that serve as a locus for purchasing and selling sex.9 Yet sex venues frequented by high-risk groups have also been the site of pilot syphilis testing and control strategies in many parts of China,10 including Shenzhen. Neighbourhood-related factors could be plausibly linked to increased or decreased sexual risk taking within the Chinese context. Exploring spatial characteristics of the leading edge of the syphilis epidemic would be useful for refining and expanding spatially targeted syphilis programs.
This study investigates primary/secondary syphilis cases in Shenzhen, China, using spatial methods and multi-level modelling. The purpose of this analysis is to identify spatial and socio-demographic subpopulations that have a higher burden of primary/secondary syphilis.
Methods
Shenzhen is a municipality of more than 10 million residents.11 The municipality was further divided into six districts which were then divided into 55 neighbourhoods in 2009. These neighbourhoods are the smallest operational administrative division within China. Substantial variation in neighbourhood social factors such as economic development and percentage of the population who are migrants creates an opportunity to investigate relationships between social factors and syphilis rates through spatial analysis at multiple levels.11
The main outcomes examined were confirmed primary/secondary syphilis cases and latent syphilis cases per 100 000 persons in 2009. All syphilis data were for Shenzhen residents, including both permanent and temporary residents, regardless of where the syphilis diagnosis was made. Syphilis data came from the China Information System for Disease Control and Prevention, managed by the China Center for Disease Control and Prevention (China CDC). Primary and secondary syphilis cases were defined according to standard Chinese definitions that require positive treponemal and non-treponemal tests in addition to consistent clinical findings.12 Latent syphilis cases were defined according to the same standards that stipulate positive treponemal and non-treponemal tests without symptoms. Spatial clustering of syphilis cases at the neighbourhood level was assessed using the Moran's I-statistic and Local Indicators of Spatial Association (LISA), both standard spatial tools for evaluating clustering.13 LISA indicates the presence or absence of significant spatial clusters or outliers for each neighbourhood. A positive SD denotes spatial clustering of similar values, while a negative value denotes dissimilar values. The Moran's I statistic of p<0.05 is consistent with a spatial distribution of high values and/or low values in the data set more spatially clustered than would be expected if underlying spatial processes were random.
All independent variables at the individual, neighbourhood and district levels are shown in table 1. At the individual level, the sex, age and occupation of individuals with syphilis came from the reporting system that has been described elsewhere.3 At the neighbourhood level, socioeconomic variables (percentage migrants, age distributions, population, hospitals per 10 000) were from the Shenzhen Statistics Bureau.11 The total population includes both registered and unregistered populations in each neighbourhood. Total entertainment venues in each district were based on calculations from the Shenzhen Health Inspection Bureau, responsible for monitoring and registering all entertainment venues. These entertainment venues were then a priori separated into low risk or high risk based on anthropological data about the commercial sex industry8 ,14; local public health staff identified the number of high-risk sex entertainment venues in each neighbourhood in late 2010. Men who have sex with men (MSM) venues were defined by previous spatial mapping exercises conducted by the Shenzhen CDC in collaboration with a network of MSM volunteers.15 Also at the district level, data regarding gross domestic product (GDP) per capita (in RMB per year) were obtained from the Shenzhen Statistics Bureau. Variables were transformed to fit a normal distribution when appropriate.
The mean or frequencies of multilevel independent variables
All variables at the neighbourhood and district levels were tested for correlation and multicollinearity in a preliminary Ordinary Least Squares regression analysis. If there was collinearity (the value of variance inflation factor was >5) and/or variables were highly correlated, one of the variables was included. A generalised estimating equations (GEE) model was used to identify correlates of primary/secondary syphilis compared with other syphilis cases, including data from the individual, neighbourhood and district levels. GEE is a commonly used type of semiparametric regression that can account for clustering of observations. A single fixed term was used to account for variability in the number of clinics or hospitals reporting syphilis at the neighbourhood level.
Primary/secondary syphilis cases were the focus of this analysis because they are early syphilis cases that more likely reflect recent syphilis transmission. Latent syphilis cases were also analysed since latent syphilis cases reflect the extent of routine syphilis screening in the area. The model goodness of fit was assessed by measuring the Akaike information criteria (AIC). We used SAS V.9.2 for the regression analyses and GeoDa V.0.9.8.14 (Geoda Center for Geospatial Analysis and Computation) for spatial analyses. This research protocol was exempted by the Shenzhen Center for Chronic Disease Control and Prevention IRB.
Results
This analysis identified a total of 6496 syphilis cases among Shenzhen residents with 1096 (16.9%) primary cases, 1227 (18.9%) secondary cases, 22 (0.3%) tertiary cases, 4137 (63.7%) latent cases and 14 (0.5%) congenital cases. Missing data accounted for <5% of each variable. Among all syphilis cases, 3168 (48.8%) were men and 3328 (51.2%) were women. The mean age of syphilis cases was 34.3 years with a SD of 12.3 years. The most common occupations associated with syphilis cases were worker (1846, 28.4%), unemployed or housewife (1475, 22.7%) and business service (1120, 17.2%). More complete descriptions of occupations were included as supplementary data (supplementary table 1).
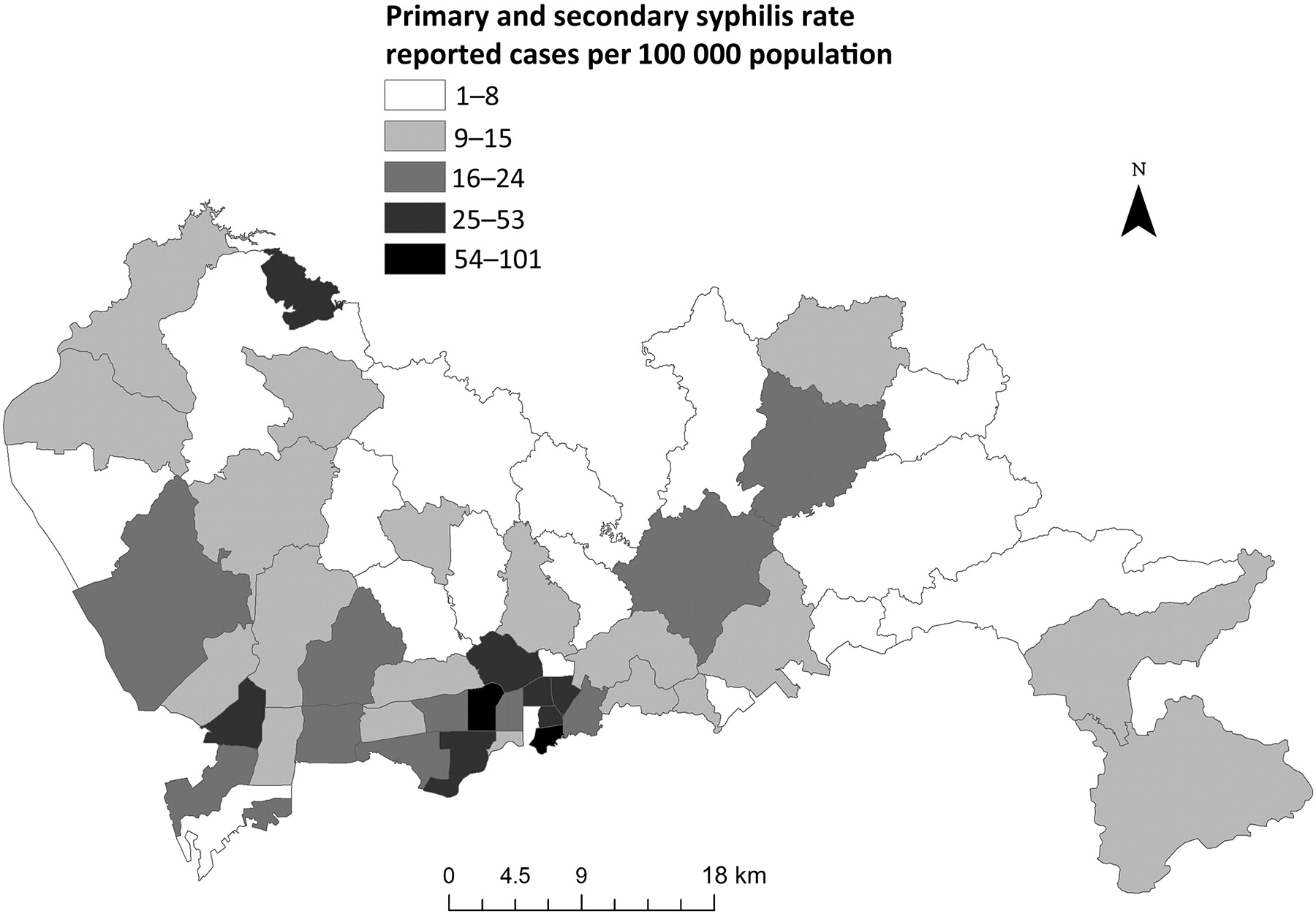
The spatial distribution of primary/secondary syphilis cases and latent cases per 100 000 by neighbourhood (n=55) were shown in figures 1 and 2. The Moran's I value for primary/secondary syphilis was 0.33 with a p value <0.01 and the value for latent syphilis was 0.19 with p value <0.05, suggesting significant spatial clustering. Clusters of primary/secondary syphilis cases were disproportionately found in southern neighbourhoods that border Hong Kong (figure 1). Latent syphilis cases at the neighbourhood level were concentrated along the southern edge of the city (figure 2). LISA maps also showed clustering of primary/secondary syphilis cases (supplementary figure 1) and clustering of latent syphilis cases (supplementary figure 2).

Primary/secondary syphilis cases by neighbourhood reported in Shenzhen, Guangdong Province, China, in 2009.

{kind=link}
{kind=link}
Latent syphilis cases by neighbourhood reported in Shenzhen, Guangdong Province, China, in 2009.
The mean or frequencies of independent variables were shown in table 1. The mean value for primary/secondary syphilis was 34.7 cases per 100 people with syphilis; the mean value for latent syphilis cases was 62.7 cases per 100 people with syphilis. A GEE model was constructed with three levels: individual, neighbourhood and district (table 2). At the individual level, men were more likely than women to have primary/secondary syphilis infection (χ2=171.2, p<0.001). Younger people (χ2=9.1, p=0.0025) and migrant labourers (χ2=3.9, p=0.047) were also more likely to have primary/secondary syphilis infection. Adjusting for the number of hospitals in each neighbourhood reporting syphilis, there was no relationship between the proportion of migrants in the neighbourhood and primary/secondary syphilis infection. At the district level, higher per capita GDP was a strong predictor of primary/secondary syphilis (χ2=46.8, p<0.001). The following variables were not significant in the best model: occupation as retired or entertainment (individual level), number of high-risk sex venues (district level) and number of MSM venues (district level). The AIC associated with the best model was 7690 as compared with an AIC of 7712 for the initial model. The addition of GDP at the district level improved the model substantially, decreasing the AIC from 7709 to 7690.
Optimal generalised estimating equations model of primary/secondary syphilis cases among Shenzhen resident in 2009 (N=2323)
In addition to the syphilis cases among Shenzhen residents reported by hospitals in Shenzhen, 2.2% (146) of the total syphilis cases were reported by hospitals outside of Shenzhen. These hospitals represented provinces beyond Guangdong as well as cities within Guangdong Province. A total of 11 other provinces diagnosed syphilis infection in Shenzhen residents, representing 19 cases. A total of 14 other Guangdong cities reported syphilis infections from Shenzhen residents, representing 127 cases.
Conclusions
This study demonstrates considerable neighbourhood heterogeneity in primary/secondary syphilis cases within Shenzhen, China, consistent with other spatial analyses of syphilis.16 ,17 Within China, clustering of syphilis cases has been reported at the city3 and district5 levels, but to our knowledge, this is the first spatial analysis of syphilis at the neighbourhood level. A neighbourhood approach has great policy relevance since reproductive health services, health outreach campaigns and a number of other local responses can be implemented through local neighbourhood committees.18 The incorporation of reporting infrastructures into our model and the use of hierarchical modelling represent improvements over prior spatial models of syphilis in China.4–6
Our finding that young male migrants were more likely to have primary/secondary syphilis runs counter to a population-based study of chlamydia in China suggesting that married, older non-migrant men were a more critical population in STI transmission.19 At the same time, a subset of young male migrants who cannot find brides has been called ‘surplus men’ and may have increased sexual risk.20–22 Several empirical studies from China have shown that subsets of rural-to-urban migrants have increased sexual risk.23 ,24 Our model did not find that there was a separate neighbourhood-level effect associated with having a greater percentage of migrants.
Despite the large spatial heterogeneity in primary/secondary syphilis cases among neighbourhoods, there was no relationship between number of identifiable high-risk heterosexual or MSM sex venues and primary/secondary syphilis cases. Given the expanding literature that links sex venues and sexual risk in China,7 ,25 this observation is unexpected. We would offer three potential explanations for this lack of an association. First, anti-prostitution campaigns in Shenzhen26 may have driven many sex workers underground into venues that are less easily identifiable. Second, the same sites that can be identified through public health authorities are also the ones most likely to be targeted for condom promotion, health outreach and related sexual health programs. Finally, the generalised syphilis epidemic may have already spread to ‘low-risk’ groups to such an extent that specific commercial sex venues are less critical in disease transmission. Further research is warranted to understand correlates of the local risk environment and what spatial attributes are associated with incident syphilis infection.
The finding that districts with higher per capita GDP are strongly associated with primary/secondary syphilis confirms findings from municipal and provincial analyses.3 ,27 This trend is also supported by the clustering of high-burden regions in the southern part of Shenzhen that borders Hong Kong. There are several potential mechanisms that could link higher GDP districts to greater primary/secondary syphilis burden. The composition of higher GDP districts having greater numbers of young male migrant labourers may help explain this relationship. Locations with higher GDP also tend to have more opportunities for commercial sex and extramarital sex. Although our data only showed a non-significant trend towards business-employed individuals having an increased risk of primary/secondary syphilis, this could also help to explain the relationship between economic development and syphilis spread. The close linkages between economic development and syphilis underscore the need for health-business collaboratives and novel models for promoting sexual health.
This spatial and multi-level analysis of syphilis infection has several limitations. First, these data are from Shenzhen residents and so comparison to other regions and cities should be made with caution. Second, these data focused on comparing primary/secondary syphilis cases to all syphilis cases but did not collect data about individuals without syphilis infection. At the same time, investigating correlates of primary/secondary syphilis infection are most critical because these represent early syphilis infections with higher transmission probabilities. Third, discrimination against STIs patients is common in China, leading to non-disclosure of real name or residence address when visiting clinics. Comparing to other Chinese cities, Shenzhen likely has better clinical services and would have a greater likelihood of obtaining more accurate spatial data. In addition, since 2005, STIs patients only disclose the neighbourhood they live in, not their exact home address, increasing the likelihood of obtaining accurate data. Fourth, our data do not include further information about high-risk sexual behaviours such as anal sex.
China's National Syphilis Control Plan28 has established clear benchmarks for controlling syphilis, with different goals set for rural and urban areas. The neighbourhood-level data here show large heterogeneity in syphilis burden within a single urban area, suggesting the need for more finely calibrated local syphilis control responses. Targeting partner notification or syphilis testing within neighbourhoods that have a greater burden of primary/secondary syphilis may be a useful syphilis control strategy.
Key messages
Primary/secondary syphilis cases showed significant spatial clustering at the neighbourhood level in Shenzhen, China.
Individuals who are younger, male, migrant labourers and those who live in districts with a higher gross domestic product had a higher risk of primary/secondary syphilis.
Spatially targeted syphilis screening initiatives in more economically developed districts may be especially useful for syphilis control.
Acknowledgments
Special thanks to the Shenzhen Center for Chronic Disease Control and Prevention for administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Funding This work was supported by grants from the Shenzhen Municipal Health Bureau for STI Prevention and Control Program, the Mega Project of China National Science Research for the 11th 5-year Plan (2008ZX10001-005) and an NIH Fogarty Career Development Award (US NIH 1K01TW008200-01A1).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.