Article Text

Abstract
Objectives Although not authorised in France, HIV self-tests are easily available online. The authors questioned French-speaking internet-using men who have sex with men (MSM) concerning their access to and use of such tests.
Methods Online questionnaire on sex websites and gay and HIV community websites. A multivariate logistic regression for rare events was used to identify factors associated with accessing self-tests.
Results 9169 MSM completed the questionnaire. 2748 (30%) were aware of online self-tests, but only 82 of those aware and not already HIV positive (3.5%) declared having accessed one and only 69 using it. In the multivariate model, living one's sex-life with men in absolute secrecy (odds ratio (OR)=3.90, 95% CI 1.73 to 8.76), knowing of the tests via a sex partner (OR=3.42, CI 1.39 to 8.41) or an internet search engine (OR=2.18, CI 1.26 to 3.74) but not through the general (OR=0.21, CI 0.11 to 0.42) or the gay press (OR=0.34, CI 0.16 to 0.73), having unprotected anal intercourse with a casual partner in the preceding year (OR=1.90, CI 1.17 to 3.06), using self-tests for other diseases (OR=2.66, CI 1.43 to 4.90), using poppers (OR=2.23, CI 1.35 to 3.67) and doping products (OR=3.53, CI 1.55 to 8) in the preceding year, having done a traditional HIV test but not in the preceding year (OR=1.93, CI 1.14 to 3.32), never having had suicidal thoughts (OR=0.54, CI 0.32 to 0.90) and living in the provinces (OR=1.80, CI 1.01 to 3.25) were all independently associated with accessing self-tests.
Conclusions Although readiness to admit use of unauthorised medical products may have influenced results, few MSM aware of the existence of self-tests actually declared having accessed one. Accessing the self-test was independently associated with both living one's sex-life with men in total secrecy and having had unprotected anal intercourse in the last 12 months, indicating that autonomous self-testing may reduce barriers to testing for this vulnerable population.
- Screening
- gay men
- HIV testing
- homosexuality
- men
- HIV
- prevention
- psychiatry
- counselling
- behavioural interventions
- sexual behaviour
- AIDS conference
- AIDS
- homosexual
Statistics from Altmetric.com
- Screening
- gay men
- HIV testing
- homosexuality
- men
- HIV
- prevention
- psychiatry
- counselling
- behavioural interventions
- sexual behaviour
- AIDS conference
- AIDS
- homosexual
Introduction
On an international level, rapidity and autonomy in accessing HIV test results are at the centre of current policy debate on screening, with certain experts now going so far as to recommend providing direct access to self-testing.1 In developed countries, an estimated 25% to 30% of HIV-positive people are unaware of their HIV status,2 ,3 and this is particularly true for certain high-risk populations such as men who have sex with men (MSM).4 ,5 Alternative HIV testing methods have proved their worth by addressing barriers to testing and bringing in individuals at risk for HIV but who are reticent to use standard procedures: in a retrospective study describing patterns of use of home sample collection (HSC) kits in the USA, 60% of all users and 49% of those who tested HIV positive had never been tested before; in one branch of the study, bisexual men accounted for 38% of positive results.6 HSC kits, where the user sends in a sample collected at home and the results are given over the telephone, are clearly a more acceptable option for persons such as these bisexual men who may be particularly concerned about confidentiality. Going for an HIV test for these men is even further compounded by the fact that the stigma around HIV/AIDS may well be largely due to it being associated with homosexuality.7 Nonetheless, studies with higher risk populations in countries, such as the USA where alternative tests are authorised, have shown varied but generally low levels of awareness and use of these tests.8
More recently, the arrival of reliable rapid tests is creating a veritable revolution in testing policy. A 2006 review of evidence on patient testing preferences concludes that, overwhelmingly, both patients and providers prefer rapid HIV tests to conventional tests.9 The rapid test is being progressively rolled out, both in low-income countries and in many Western countries, where it is generally being integrated into existing health service provision.
However, this is not the case for the self-test. Although increasingly recommended as a serious option for facilitating access to HIV testing,10 it encounters strong opposition from health professionals who, aside from problems related to the currently higher risk of inaccurate results11 or user errors,12 consider that the face-to-face testing process, whether the results are positive or negative, provides a key time to start people thinking about risk reduction or accessing care.13 Professionals are also worried that discovering positive test results alone at home may increase suicide risk, an argument already encountered prior to the introduction of HSC kits in the 1990s, with opponents underlining the risks involved with people receiving results by telephone.14
Nonetheless, studies increasingly reveal that the general population are open to or would prefer self-testing: more than one-third (37%) of Californians would be willing to use an instant home HIV test if a reliable one were available.15 Individuals in high-risk groups who have never tested before are significantly more likely to prefer home self-testing, finding it to be more private, convenient and faster.16 Furthermore, internet marketing strategies for self-tests exploit the fact that internet is also increasingly used for sexual encounters, thus transforming the HIV risk environment,17 with the populations most at risk investing it in a major way.18 This is particularly true for MSM. Already in 2003, in a survey of gay men in the UK, two-thirds of men declared using the internet for sexual purposes in the previous month and more than half of Londoners in the last 48 h.19 The situation in France is similar.20 ,21
The need for new testing strategies that take into account the evolving social networking media for MSM is increasingly evident. This need is even more critical in that, in a general population context of decreasing incidence of HIV, there has been no corresponding decrease among MSM.22 ,23 Furthermore, MSM who find partners on the internet are more likely to have more sexual partners and more unprotected anal intercourse (UAI) than those who use other methods for meeting partners.24 ,25
In France, the distribution and sale of HIV self-tests is not authorised. However, self-tests being easily accessible via internet, there is a real possibility that the general public, and especially those who use the internet, are already accessing such tests or at least considering accessing them. In addition, confidentiality, rapidity in accessing test results and less invasive testing methods are advantages that internet advertisements promoting self-tests do not hesitate to underline.
The purpose of the present study was to determine awareness of, access to and use of unauthorised online HIV self-tests in a population of French-speaking MSM who use dating or sex websites or gay or HIV community websites.
Methods
Study design
The survey was conducted online for 12 weeks from 3 February to 29 April 2009, promoted via banners with links and/or emails sent to subscribers of 11 MSM sex, dating and chat sites, five gay community websites and the two principal French HIV/AIDS community information websites. Respondents were men aged 18 years or more who were users of the websites in question and who chose to answer the proposed online questionnaire. No remuneration was offered for survey completion.
No personal identification information was collected. The questionnaire information page described the nature of the survey and informed respondents that the software managing the survey guaranteed their anonymity and that all information recorded was completely anonymous. Respondents wishing to participate then had to click on a specific link to access the first question. Approval for the study protocol was obtained from the Commission Nationale d'Informatique et des Libertés.
Questionnaires
The survey included 93 questions regarding knowledge of, attitudes to and use of self-tests, internet use, demographic characteristics and sexual attitudes and behaviours. Using algorithms with skip and branch patterns, participants were presented with different sequences of questions depending on their individual responses. The questionnaire was piloted off-line and online with 30 MSM during the formative phase of the study and modified based on responses.
Statistical analyses
Due to the low number of participants (3.5%) declaring having accessed self-tests, the characteristics of this subgroup were analysed using logistic regression for rare events.26 Model building was in two steps: first, a list of potential explanatory variables was defined and a univariate analysis was conducted on these; variables with a p value inferior to a predefined threshold (0.20) were then included in a multivariate analysis and a backward selection method based on the log-likelihood ratio test was used to select significant variables in the multivariate model (significance level α=0.05). Data management was performed using SPSS (SPSS Inc.), with STATA being employed for statistical analyses (StataCorp LP).
Results
Study population
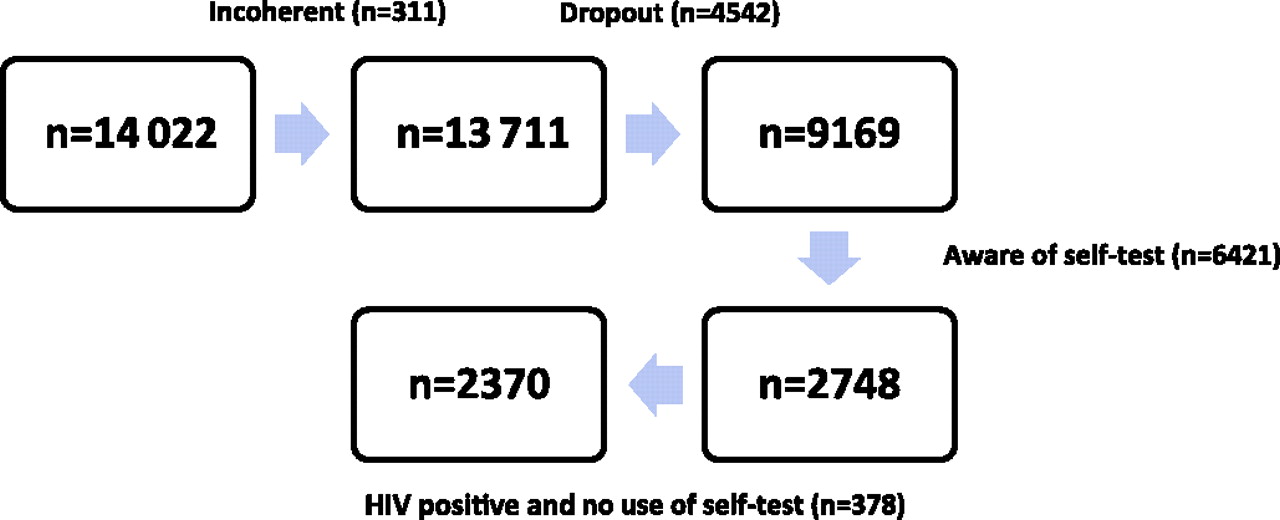
The survey presentation page was displayed 119 326 times during the study period, by visitors either clicking on the banner on one of the 18 sites participating in the study (43 257, 36.3%) or by accessing the research site directly (76 069, 63.7%). On only 14 022 occasions (11.8%) did visitors actually click on the link at the bottom of the presentation page, thus opening the second screen of the questionnaire and accessing the first question. Due to the privacy protection system used to prevent access to participants' identities, no information was available concerning the number of different PIN addresses used to access the questionnaire nor how many different people accessed the questionnaire. The same person could have displayed the questionnaire more than once. Questionnaires (n=311) from respondents whose answers were incoherent, who explicitly stated they were not MSM or who completed the questionnaire but failed to respond to more than 15 questions were excluded. Of the remaining 13 711 men, 4542 (33.1%) dropped out before reaching the final question. The final 9169 MSM who completed the survey did so in an average of 23.2 min.
Comparisons using the χ2 test between those who completed the survey and those who did not revealed that completers were more likely to have university-level education (58.7% compared with 54.7% of those who dropped out, p=0.001), a job (77.8% vs 75.3%, p=0.017), a higher revenue (51.0% vs 47.2%, p=0.002) and to be already aware of the existence of the self-test (30.0% vs 24.0%, p<10−3). However, completers were not significantly more interested in accessing the self-test (83.0% vs 83.6%, p=0.483) nor were they more likely to live in a city of more than 100 000 inhabitants (49.9% vs 48.5%, p=0.199). A Mann–Whitney test for age revealed that they were also older (median age 35.8 vs 33.8, p<10−3) (figure 1).

{kind=link}
Study population: men who have sex with men (MSM) aware of existence of online self-test, including HIV-positive men who declare having used the self-test but excluding other HIV-positive MSM.
In answer to the first question concerning respondents' awareness of the existence of self-tests available online, three in 10 respondents (2748/9169=30.0%) responded positively. Of these men, 378 declared being already HIV positive and never having accessed the self-test. This paper examines the points of view of the 2370 remaining participants concerning their access to and use of the online self-test.
The self-reported characteristics of these 2370 men are described in table 1. The median age was 35 (Interquartile ratio (IQR):(28–43)). More than one in three (34.3%) were living in the greater Paris area (Ile-de-France) and 62% in the provinces or overseas departments and territories; only 3.3% lived in foreign countries. Two respondents in three (67%) had a university degree or equivalent and more than half (54%) earned €1600 per month or more. Over four respondents in five (85%) defined themselves as being homosexual or gay; 12% declared living in a traditional family either with their parents or with a female partner and/or children; 11% lived their MSM life hidden or in total secrecy. More than eight of 10 respondents (84%) had had more than one casual sex partner in the preceding year and 34% had had UAI with at least one of these casual partners. Half of the study participants (49%) had had suicidal thoughts. With regard to HIV testing, 59% had done at least one traditional test in the last 12 months, 31% prior to that and 10% never. One in two (48%) had heard of the self-test via the general public press.
Self-reported characteristics of participants aware of the existence of the HIV self-test (n=2370) and who have accessed it (n=82) or not
Only 82 respondents (3.5%) declared having already accessed the self-test: 63 had accessed it for themselves, two for another person and 17 reported someone else accessing it for them.
Accessing the self-test
In the multivariate logistic regression for rare events, the following factors were identified as independent correlates of having accessed the self-test: living one's sex-life with men in absolute secrecy, having heard of the self-test via a sex partner or an internet search engine but not through the general or the gay press, having had UAI with a casual partner in the preceding year, having used self-tests for other diseases, having used poppers and doping products in the preceding year, having done a traditional HIV test but not in the preceding year, never having had suicidal thoughts and living in the provinces (table 2).
Univariate and multivariate logistic modelling of factors associated with accessing the self-test (n=2370)
Using the self-test
Among the 82 respondents who had had access to the self-test, 69 had used it on themselves. Of the latter, 42 (61%) reported using it once and 27 (39%) several times. Thirteen had accessed it but not used it. First use was recent for most users, with 48/69 (70%) using it for the first time since January of the year preceding the study (2008).
Of the 63 men who bought the self-test themselves, eight (13%) had not used it, 31 (49%) had used it once and 24 (38%) several times. Of the 17 men who reported someone else accessing the self-test for them, five had not used it. Only two men reported buying the self-test for someone else—and they had done this several times. In both cases, it was not for someone with whom they were planning to have a sexual relationship. Both reported also having used it on themselves several times.
For the 69 men who reported having used the self-test, concerning their most recent use, the result was negative in 62 cases and positive in three. The other four users were uncertain of their results: three had not understood how to read the results and one felt he had not used the test correctly. Almost one in two (29/62=47%) of those who tested negative had since sought confirmation of this result. Of those who had sought confirmation, 24 went to a private clinic or an HIV testing centre and five did a second self-test. The initial negative test result was confirmed for all 29.
All three men who tested positive were alone when they discovered the result. None had gone to see a doctor to talk about this positive result. Two did not talk to anyone about the result. The first noted that he was not particularly surprised and had been expecting this result. He did a second self-test and the result was positive again. The second man did a traditional test in a testing screening centre and this time the result was negative. The third man indicated that he was surprised and shocked to discover a positive result; he called a hotline but had not yet gone for confirmation.
Finally, out of the four people whose test result was uncertain, two went to a testing centre for confirmation, one of whom tested negative and the other did not go back to get his results. The two others had not sought confirmation of their test results at the time of the study.
Discussion
This study is the first to investigate access to unauthorised online HIV self-tests by MSM in a French-speaking context. Although a large number of men responded to the online questionnaire, only 30% declared being aware of the existence of the online self-test, and only 3% (n=82) of those aware declared having accessed one. Of the latter, 84% (n=69) declared having used it. Use of self-tests does not exclude use of traditional HIV clinical tests: in the present study, almost one user in two had since validated self-test results at a private clinic or an HIV testing centre; furthermore, contrary to the findings reported above concerning HSC kits,6 where people who had used these kits were more likely to have never done the traditional HIV test, this was not the case in the current study with online self-tests: indeed, accessing the self-test was associated with having already done a traditional HIV test but just not in the preceding year.
These results cannot be presented without taking into consideration the fact that the self-test is not authorised for sale in France: it is possible that certain users might have chosen not to respond to the questionnaire or, if they had, not to admit to having purchased or used the test in question. Furthermore, although the response rate (11.8%) is favourably comparable to other internet studies using banners,18 banner recruitment inevitably creates sample bias, in the present case no doubt over-representing the points of view of men interested in HIV self-tests. Similarly, although almost identical to that of other major internet surveys with similar population groups,27 ,28 the implications of a completion rate of only 67% cannot be ignored: questionnaire completers were older, had higher educational, income and employment levels and lived in larger towns or cities compared with those who dropped out. In addition, recruiting online via French-speaking MSM sex, dating and chat sites and gay and HIV/AIDS community websites excludes MSM who do not frequent such sites, even though they may be regular users of the internet. Generalising from this sample to younger MSM, to all internet-using MSM, to MSM speaking other languages or to other internet-using populations is therefore hazardous.
Multivariate logistic regression reveals a model for MSM who access the self-test which underlines the importance of privacy and autonomy for men whose MSM sex-life is lived in total secrecy and who take sexual risks. Although self-defined sexual identity was a highly significant factor in univariate analysis, with respondents who defined themselves as homosexual or gay being significantly less likely to have accessed the self-test, this factor no longer remained in the multivariate model. Self-defined sexual identity seems to be less important than the question of how openly men live their gay or MSM sex-lives, underlining the fact that individuals can define themselves as gay or homosexual but still live their sex-lives with men in total secrecy. Clearly, every attempt should be made to take into account such particularities and adapt testing options to the specific needs of each population, particularly for those at higher risk. Although opponents to self-testing may argue that this might simply result in displacing the barrier from testing to treatment for this highly sensitive population (and indeed, although all three men who had self-tested positive in the current study had subsequently taken further steps with regard to their personal health status, none had, at the time of the survey, talked to a doctor about their positive self-test result), knowing they are HIV positive should encourage many to take steps to protect their partners.29 The question of individual autonomy with regard to screening is further underlined by the fact that, in the present study, having already used self-tests for other diseases was also an independent predictor of accessing the HIV self-test. A remarkable aspect of this model is that, with the exception of living in the French provinces outside of the Greater Paris Area, no demographic variable, including age, income, education or employment status, remained in the model as an independent factor in multivariate analysis. Living in the provinces clearly adds barriers to screening for MSM, whether it be in terms of greater distances to access screening centres or greater stigma attached to HIV or to homosexuality. Finally, the fact that men who had experienced suicidal ideation were less likely to have accessed the self-test casts new light on the traditional argument of a heightened risk of suicide associated with self-testing. Although the current study does not allow us to conclude that self-test users suicide less—indeed, men who might have committed suicide after doing the self-test could scarcely participate in the survey—the possibility that MSM at risk of suicide are less likely to seek to play an autonomous role in health screening cannot be excluded.
The question of authorising anonymous online self-tests is clearly posed. At a time when citizens are encouraged to take responsibility for their own health, and with the ever-increasing acceptance of self-testing for other health conditions, as well as greater public awareness about HIV prevention and treatment, restricting HIV testing to clinical contexts directly contradicts the principles of empowerment and autonomy. This is all the more crucial for individuals for whom loss of anonymity might have grave consequences for their lives and for the lives of people around them. Resistance from health professionals to self-testing can no longer be the decisive argument. Above all, this entire debate is being undermined by internet marketing strategies for sexually transmitted infections, including HIV, promising rapid self-test results completely independently from clinical settings in the conventional health system. If, in this context, online purchase of the test is to become an acceptable and viable solution for individuals for whom anonymity is a determining issue, this will necessarily also involve educating people about the use of HIV self-tests and building educational strategies addressing the specific problems faced by subgroups such as men who live their MSM lives in absolute secrecy, particularly with regard to support in accessing care should the test result be positive.
Key messages
Few MSM declared accessing unauthorised online HIV self-tests.
Men who had accessed the self-test were more likely to live their sex-lives with men in absolute secrecy.
Men who had had suicidal thoughts were less likely to have accessed the self-test.
Anonymous online access to the HIV self-test may be a viable solution for high-risk men who live their sex-lives with men in total secrecy.
References
Footnotes
Funding This work was supported by the French National Agency for Research on AIDS and Viral Hepatitis grant number ANRS 08078/09099/09520.
Competing interests None.
Ethics approval Ethical approval was provided by Commission Nationale d'Informatique et des Libertés.
Provenance and peer review Not commissioned; externally peer reviewed.