Article Text

Abstract
Many innovative diagnostic technologies will become commercially available over the next 5–10 years. These tests can potentially transform the diagnosis of sexually transmitted infections but their introduction into control programmes can be hampered by health system constraints, and political, cultural, socioeconomic and behavioural factors. We used the introduction of syphilis rapid tests to illustrate the importance of programme science to address the gap between accruing evidence of acceptable test performance and the complexity of programme design, implementation and evaluation of test deployment to address public health needs and improve patient-important outcomes.
- Diagnosis
- Programme Science
- Sexual Health
Statistics from Altmetric.com
Introduction
The global burden of sexually transmitted infections (STIs) is highest in the developing world where access to laboratory services is limited.1 Highly sensitive and specific laboratory diagnostic tests using non-invasive specimens have enabled developed countries to screen for and diagnose curable STIs in a variety of settings, but control programmes in resource-limited settings without access to laboratory facilities have largely been dependent upon a syndromic approach for the management of symptomatic cases of STIs, while screening programmes for asymptomatic infections have been unaffordable.
Simple, rapid and affordable point of care tests (POCTs), which do not require electricity, a laboratory or highly trained staff, are now available for several STIs. POCTs offer an unprecedented opportunity to improve healthcare, especially for poor, rural and marginalised populations, and to reduce inequalities in health. However, scientific evidence of good performance and ease of use often fails to translate into impact due to the enormous gap between the demonstration of scientific effectiveness and the complexity of programme design, implementation and scale up, particularly in fragile or dysfunctional health systems.2 ,3 There is growing recognition of the importance of programme science to address this gap in different areas of global health. The application of programme science to the introduction of STI diagnostic technologies is particularly important for reasons listed in box 1.
Special considerations in introducing diagnostic technologies for sexually transmitted infections (STIs)
-
An STI diagnosis is frequently associated with stigma, shame and denial.
-
STI testing should be private and confidential.
-
Most individuals with STIs are asymptomatic most of the time.
-
False-positive and -negative results lead to harm for the patients with adverse psychosocial and societal consequences.
-
False-negative (lack of sensitivity) diagnosis leads to failure to treat and increases risk of long-term complications and onward transmission within the population.
-
False-positive (lack of specificity) diagnosis leads to erroneous diagnosis, overtreatment and potentially psychosocial harm.
-
-
Co-infections with two or more pathogens, such as HIV and genital herpes or syphilis, are common.
-
There is considerable heterogeneity in behaviours making it critical to understand risk perception, the social and sexual networks in which persons operate and their health seeking behaviour.
The pathway from diagnostics development to implementation
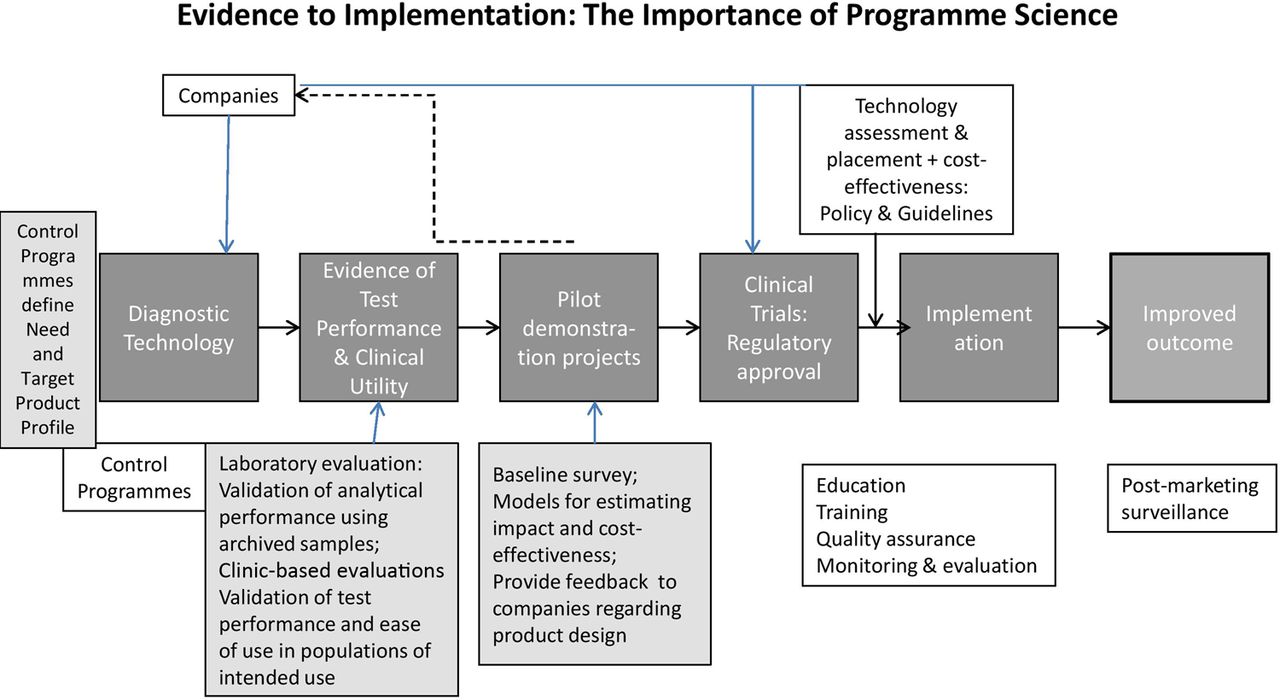
The conventional pathway from test development to the introduction of new diagnostic technologies is illustrated in figure 1. In response to needs defined by country policy and control programmes, companies develop tests and optimise their performance and ease of use with feedback from laboratory and clinic-based evaluations. Companies are required to conduct regulatory quality trials to determine product safety and effectiveness while control programmes need to assess new diagnostic technologies and, based on their operational characteristics and cost-effectiveness, place them into appropriate levels of the healthcare system. Once a diagnostic product is approved for sale in a country, policy and guidelines for its use need to be developed. At the same time, education of the public and healthcare providers on the new technology, including its limitations, should be undertaken by the companies and the public sector. The success of introduction and implementation depends critically on the extent to which the technical aspects of training, quality assurance (QA), supply chain management and linkage to treatment, care and surveillance are planned within the political, socioeconomic, cultural and behavioural context of the population and the health system where they are to be used.

{kind=link}
Translation of evidence of acceptable diagnostic performance to policy and implementation: importance of programme science.
The importance of programme science
Programme science is the systematic application of theoretical and empirical scientific knowledge to improve the design, implementation and evaluation of public health programmes; its end point is a reduction in the incidence of disease at the population level. To illustrate its importance, we used the example of the introduction of rapid syphilis tests to prevent congenital disease in high burden countries.
Syphilis in pregnancy causes close to one million stillbirths or neonatal deaths each year. These adverse outcomes could be prevented by screening all pregnant women for syphilis and treating those who are found to be infected with a single dose of penicillin before the third trimester.4–6 Prenatal screening for syphilis is the recommended policy in almost every country. According to the latest Unicef statistics, 75–85% of women attend an antenatal clinic (ANC) at least once during pregnancy.7
In the 1990s, several papers were published describing the success of decentralising prenatal screening for syphilis in sub-Saharan Africa using the Rapid Plasma Reagin (RPR) assay, which only takes 8 min and costs $0.2 per test.8–10 Yet, two decades later, syphilis remains a major cause of stillbirth and neonatal mortality in much of the developing world.11 There are a number of reasons why country programmes have difficulty implementing the RPR test as a POCT in many healthcare settings even though it is rapid and affordable. The test card is designed for 10 reactions per card, so tests must be performed in batches, requiring patients to return for a follow-up visit to obtain their test results. The test can only be used with serum, and requires electricity to operate a centrifuge, a shaker and a refrigerator for reagent storage. Health workers who are not laboratory trained often find the test results difficult to interpret.12 ,13
New POCTs for syphilis are now available which do not require electricity and are easy to perform. Several of those on the market meet the ASSURED criteria, being Affordable, Sensitive, Specific, User-friendly, Rapid and robust, Equipment-free and Deliverable to those who need them.2 ,14–16 It is now possible to advocate for a Same day Testing and Treatment (STAT) strategy to overcome the barriers to testing. However, if we examine the reasons why syphilis has remained a major cause of stillbirth and neonatal mortality, the barriers we face in implementing POCTs are no longer technological, but they are the constraints inherent in the healthcare system, and the lack of political will and knowledge of the adverse outcomes of pregnancy associated with syphilis (table 1). To address the gap, it is important for policy makers and programme managers to consider the following:
Factors affecting the effectiveness of prenatal screening programmes for syphilis
Policy and stakeholder consultations
Although prenatal screening for syphilis is the recommended policy in almost every country, the implementation of policy has not been effective because programme managers do not have the appropriate tools. Public health needs and country policies can drive technology development, as is the case with the development of several nucleic acid amplification tests for the screening for genital chlamydial infections. However, there is often a mismatch between public health needs and the available diagnostic tools because countries lack the capacity to accurately define target product profiles that test developers need as a starting point for technology development (figure 1). Such knowledge synthesis requires a sound grasp of disease epidemiology, health infrastructure, health-seeking behaviours and human and financial resources in a country. It is critical that programme science, as applied to screening or diagnosis of STIs, incorporates early interactions between test developers and policy makers at national and global levels on appropriate diagnostic tools that are needed to change the status quo. For the design of POCTs, there may be trade-offs between test performance and ease of use or rapidity of test results, which can be guided by policy consultations.
Technology assessment and appropriate placement
When a new technology becomes available, its performance and operational characteristics should be assessed in laboratory and clinic-based studies. If the technology shows acceptable performance and addresses a public health need, then it is important to consult policy makers and stakeholders in deciding where the new test could be deployed within the healthcare system for maximum health impact. The appropriate placement or deployment of the technology should be informed by need, technical capacity and cost-effectiveness. Consultations with personnel from all levels of the healthcare systems and with civil society should be part of the assessment.
If more than one POCT with acceptable performance is available, the diagnostic technology assessment panel should consider developing criteria for test selection that include:
-
Test performance
-
Ease of use
-
Conditions of use
-
Conditions and duration of storage
-
Requirement for other supplies
-
Price
The criteria can be weighted depending on the availability of resources, prevalence of infection, programme capacity and existence of comorbidities. For example, although price is often the most important consideration, POCTs that have the longest stability without the need for refrigeration are preferred by countries in which customs clearance and distribution of commodities to target populations may take a long time.
Test evaluation
A preliminary estimate of test performance can be determined using well-characterised archived specimens. If results are promising, field trials can be conducted to determine test performance in which testing is performed by healthcare workers (HCWs) in settings of intended use17 (figure 1).
Cost-effectiveness
The cost per person screened and treated depends largely on the cost of the test and the prevalence of the STI. The cost of rapid syphilis testing in sub-Saharan Africa amounts to approximately US$2 per woman screened.18 The cost per person treated becomes higher as the prevalence drops. In models developed based on costs in Tanzania and Haiti, approximately 50% of the cost of the rapid test programme is the cost of the tests, with personnel and supplies accounting for less than 15% of the remaining costs.18–20
POCTs are slightly more expensive than RPR (approximately US$0.5, compared with $0.2 for RPR). Nevertheless, even when the costs of training, supervision and QA are included, the cost per ANC attender tested is generally less than US$3.
Integrating syphilis screening into Prevention of Mother to Child Transmission programmes for HIV screening, is particularly cost-effective as personnel time and building space can be considered shared costs, especially in countries that have made a strong commitment for the joint elimination of Mother to Child Transmission of HIV and syphilis.
Pilot studies
Consultations with the ministry of health and other stakeholders on the design and location of pilot projects for test introduction are important. Pilot studies to introduce POC STI testing should be conducted in a variety of settings and populations so that results can be generalised to as many countries as possible. Models that are available online can be used to estimate the potential impact of a STI diagnostic test and its cost-effectiveness.21
Baseline survey to determine health systems failures
Before making plans for implementation, a baseline survey is critical as policy makers are sometimes not aware of the low implementation rates or the barriers faced by health facilities around the country. This is especially true when a surveillance system for maternal syphilis screening does not exist or does not function well. Information on current practice for syphilis screening and barriers to achieving full coverage, recent records on the number and proportion of women screened and treated for syphilis can be obtained through interviews with healthcare providers and their supervisors.
Acceptability of rapid syphilis tests among healthcare workers and communities
Although POCTs have been well accepted by HCWs and ANC attenders in many studies, laboratory staff is sometimes opposed to the idea of training non-laboratory personnel such as nurses and midwives to do a task that had traditionally been done by trained laboratory technicians, especially in countries with excellent laboratory services. Laboratory staff needs to be involved in the training and supervision of HCWs doing the tests, and in setting up a QA programme to monitor the proficiency of HCWs in performing the test. Giving certificates of competence motivates the HCWs.
Implementation
Cultural contexts
In central Haiti, many babies are either stillborn or die in the first year of life. A myth has developed in the communities that a werewolf, the Loup Garou, preys on pregnant women as they sleep, sucking the blood out of the babies in the mother's womb.22 In introducing syphilis rapid tests, Groupe Haitien d'Etude du Sarcome de Kaposi et des Infections Opportunistes and the Ministry of Health worked with HCWs, traditional healers and voodoo priests to overcome these traditional beliefs. Knowledge of syphilis has empowered pregnant women to understand the importance of syphilis screening and treatment to keep their babies healthy.
In working with marginalised populations, understanding their perception of risk, what motivates them to have better healthcare seeking behaviours, and how to gain their trust and make services culturally sensitive and user-friendly are important considerations in planning the introduction of new diagnostic technologies. Cultural issues are also encountered in the treatment of STIs. There are cultures in which patients prefer injections to oral therapies. In some countries, health providers are reluctant to give penicillin to syphilis patients because of their fear of allergic reactions.
Training and site preparations
There is a serious shortage of trained staff in the health sector in many countries. Integrated screening for syphilis and HIV in ANCs can reduce the demands on HCWs, but problems remain even in clinics that have a high turnover of staff. Trained HCWs are often transferred to new facilities and do not always train the HCW remaining on site, leaving the facility unable to provide testing. Training in the use of POCTs needs to be rolled out at the national level, and included in the curriculum at schools of nursing and midwifery.
HCWs need to be trained in the use of POCTs, using training materials translated into the local language and adapted according to local needs. Courses for trainers and supervisors should be organised, including practical training on how to perform the tests and interpret the results, and how to train HCWs and assess their competence, with additional training in stock management, record keeping and quality control.
Standard operating procedures can be developed for performing a finger-prick, performing a POCT, preparing proficiency panels for QA, performing quality control testing and managing an out of specification result, ordering supplies and collecting samples for confirmatory retesting. Algorithms should be developed to guide treatment and other patient management decisions based on the test result. All individuals who test positive should be treated with appropriate drug regimens as recommended in the national guidelines on the same day and requested to refer sexual partners for testing and treatment.
Supply chain management
In many countries, supply chain failure is one of the most common reasons for not testing. Healthcare workers and their supervisors should receive training in stock management, but problems may remain at national, regional or district levels, especially when manufacturers are unable to keep up with the demand or there are long delays in clearance through customs. In recent years, simple optical readers or scanners for POCTs have made it possible to transmit test results to a central database. It is anticipated that supply chain problems may be alleviated if test results can be linked to supply chain software, allowing more accurate forecasts based on real time data on consumption of POCTs.
Quality assurance
For accurate results, it is important to ensure the quality of the tests as well as the testing. A quality management system should be developed that includes the development and distribution of standard operating procedures, training of HCWs and laboratory staff to ensure the quality of the tests and that testing is performed correctly.
A simple, low cost method for proficiency testing has been developed by the US Centres for Disease Control and Prevention to assess the ability of a healthcare worker to correctly perform rapid HIV testing and interpret the results.23 Dry tube specimen panels are prepared by allowing aliquots of sera with high titre antibodies, and negative control sera, to evaporate. These dry tubes can then be stored and transported at ambient temperature, and reconstituted with buffered saline on arrival at the site of HIV testing. This approach can be adapted for use to ensure accurate POC testing for syphilis.
The proficiency panel allows supervisors to identify HCWs in need of refresher training, motivates HCWs, and reinforces good practice. The continuing use of proficiency panels to monitor the quality of testing is particularly important where there is a rapid turnover of staff, but the importance of QA programmes in settings outside of the laboratory is not widely recognised.
Monitoring and evaluation
Programmes should develop a checklist for monitoring visits and train proficient staff members to conduct monitoring visits. After the POC testing programme has been introduced, an internal monitor should be appointed to collect data on the number and proportion of people screened, the proportion that tested positive for syphilis, and the proportion of those testing positive who were treated, and to monitor problems in a timely manner. Problems should be immediately brought to the attention of the programme manager, and solutions tried until a sustainable one is found. External monitors should also visit the sites and provide suggestions for improvement. The opinions of HCWs on the simplicity and acceptability of the POCTs can be sought through interviews and focus group discussions.
Impact on other services
Integrating HIV and syphilis screening in prevention of mother to child transmission programmes avoids the tragedy of preventing babies from HIV infection only to have them die from syphilis, and is cost-effective.24 Vertical disease control programmes and silo healthcare infrastructures often do not result in cost-effective programmes and patient- important outcomes. An essential diagnostic package for prenatal care which can include diagnostics for infectious diseases and conditions such as anaemia and pre-eclampsia, should be considered, based on disease prevalence and epidemiological context, to improve the quality of prenatal care in all settings.
Impact of POCT introduction on health systems
In addition to improving pregnancy outcomes by ensuring higher coverage and earlier treatment of syphilis in pregnancy, the STAT strategy using POCTs can strengthen health systems by motivating HCWs and increasing capacity and efficiency as it reduces the number of return visits required.25
We have conducted a multi-country project to determine feasibility and cost-effectiveness of introducing rapid syphilis screening in prenatal and high-risk populations.25 Using the STAT strategy, we developed a generic protocol with standardised outcome measures. We encouraged all country teams to develop country-specific protocols within the health system infrastructure and the political, cultural and socioeconomic context of their setting. In all countries, policy has changed as a result of this demonstration project. POC testing, using the new rapid syphilis tests to provide a STAT service is now recommended policy in all countries in which the study was conducted, and national guidelines have been amended accordingly. What lessons can be learnt from this? Clearly, it is important to involve policy makers from the outset of a demonstration project such as this, and to keep them informed at all stages. In all six countries, regular meetings were held between project staff and Ministry of Health officials at national, regional and district levels, focussing on those responsible for maternal and child health and HIV/AIDS programmes. Through this project, we learnt that, unlike the situation for the adoption of new drugs and vaccines, leadership and infrastructure for critical decision making on the adoption of new diagnostic technologies is fragmented or absent in many countries in the developing world. The following are critical to the success of test introduction:
-
Engagement of policy makers and stakeholders as peers, throughout the entire study period
-
Sharing and communication of results
-
Using clear compelling messages
-
Identifying champions to promote syphilis screening
-
Training and technical assistance
-
Positive feedback to HCWs
-
Involving other partners
-
Making cost-effectiveness analysis user friendly
-
Keeping motivation high
Conclusion
High quality diagnostic tools play a critical role in improving global health. The development and increased use of high quality POCTs could have a major impact in reducing inequalities in healthcare. We have used the example of simple, inexpensive POCTs which can be used to diagnose maternal syphilis and prevent congenital infection to illustrate the importance of programme science in successful programme introduction and management. In the next few years, many novel diagnostic technologies will become commercially available. National disease control programmes need to consider programme science and set up an informed and well-structured diagnostic technology assessment and placement programme to inform policy decisions and design implementation and evaluation plans that address public health needs and take into account patient-important outcomes.
Acknowledgments
The authors thank the principal investigators of the syphilis POCT introduction study for valuable contributions towards the validation of programme science principles.
References
Footnotes
-
Contributors The corresponding author developed the concept for the paper and prepared the first draft. All authors contributed to the writing of the paper.
-
Funding Funding for the multi-country syphilis implementation project came from the Bill & Melinda Gates Foundation, grant #47697.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.