Article Text

Abstract
Objective To discuss the epidemiology of Trichomonas vaginalis (TV) and HIV co-infections, the role of TV in acquisition and transmission of HIV, special treatment considerations for TV among women with HIV and the prevention of TV among HIV-infected persons.
Design Systematic review.
Data source Review of literature of EMBASE and PubMed databases from January 1990 to February 2013. Search keywords included TV, HIV co-infections, HIV acquisition, HIV transmission, HIV shedding, TV treatment, HIV and couples studies.
Review method We included studies of any design that contained the selected search words and were published during the specified time frame. We then searched the reference lists of included papers for additional papers and included these when relevant.
Results There is strong evidence that TV increases both transmission and acquisition of HIV among women, and that successful treatment for TV can reduce HIV genital shedding. Single dose metronidazole (MTZ) should no longer be used for HIV+ women with TV given the high rates of asymptomatic bacterial vaginosis co-infections and other factors that may render MTZ less effective in HIV+ women. Prevention of TV among HIV+ persons is similar to among HIV, including promotion of condoms as well as regular screening and prompt treatment. There may be a role for expedited partner treatment for the prevention of repeat infections, but most repeat infections are clinical treatment failures. Diligence in screening and treating TV among both HIV- susceptible and HIV+ persons is an important public health strategy.
- TRICHOMONAS
- HIV
- TRANSMISSION DYNAMICS
- TREATMENT
- PUBLIC HEALTH
Statistics from Altmetric.com
Trichomonas vaginalis (TV) is the most common non-viral sexually transmitted infection (STI) worldwide1 and has been associated with pelvic inflammatory disease and adverse pregnancy outcomes.2 Once thought to be a minor STI, TV is now being given more attention because of its potential role in both the acquisition3–6 and transmission7–9 of HIV. In this paper, we discuss the epidemiology of HIV and TV co-infections, present evidence that TV plays a role in HIV acquisition and HIV transmission, describe the theories of how TV amplifies HIV transmission, discuss issues of TV treatment among HIV positive women, and present potential prevention measures of TV among HIV+ persons.
Methods
EMBASE and PubMed databases were searched with date ranges between January 1990 and February 2013. Search words included: TV and HIV acquisition, TV and HIV transmission, HIV shedding, epidemiology of HIV/TV co-infections, modelling and TV treatment and HIV, and TV and HIV and couples studies.
Selection of papers for review
The review of papers was completed by two reviewers (PK and AA). Titles and abstracts (where abstracts were available) were screened for relevance and duplicates removed. Relevant papers were reviewed for the association between TV and HIV acquisition, TV and HIV transmission (mostly via genital shedding), and HIV shedding and TV treatment. Reference lists of relevant papers were also searched and any additional relevant studies from these lists were included.
Results
Using all search terms in both databases, 1068 papers were identified. After eliminating duplicates 560 remained. The titles and abstracts of these papers were reviewed for relevance and 33 papers were reviewed in full. An additional three studies on TV and HIV modelling and two abstracts were found on the topic of TV treatment among HIV+ women, and 40 other papers were found on TV/HIV co-infections and other related topics.
Epidemiology of TV and HIV co-infections
While the global prevalence of TV is unknown, rates differ by population and by region. TV disproportionately affects women of African descent. In the USA, the highest prevalence of TV is seen among African Americans with rates ranging from 13% to 51%,10 a rate well above the US population-based prevalence of 3%.3 African Americans are also the demographic group which also has the highest rate of HIV in the USA.4 Worldwide, the majority of the 174 million new cases of TV each year are found in Sub-Saharan Africa, a place where the majority of HIV infections also occur.5 In Sub-Saharan Africa, the rate of TV ranges from 11%6 ,7 in population-based studies to 20.9% in pregnant women,8 but selected cohorts have demonstrated much higher rates.
Women who have HIV have high rates of TV and women who have TV have excess rates of HIV. Prevalence of TV ranges from 6.1% to 52.5%8 ,9 ,11–16 among HIV-positive women compared with 3.2%–34% among HIV-negative women.5 ,17
TV and HIV acquisition
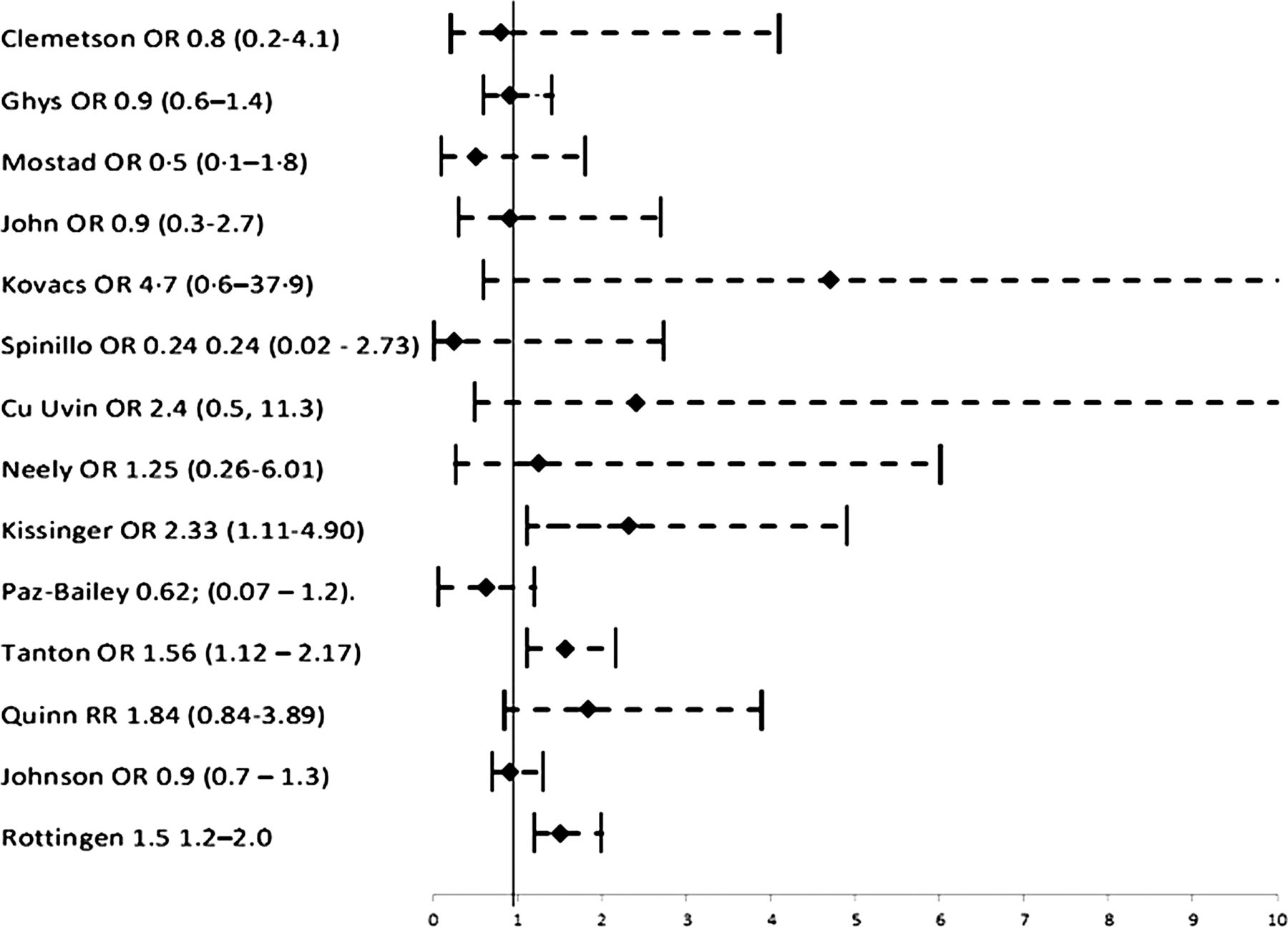
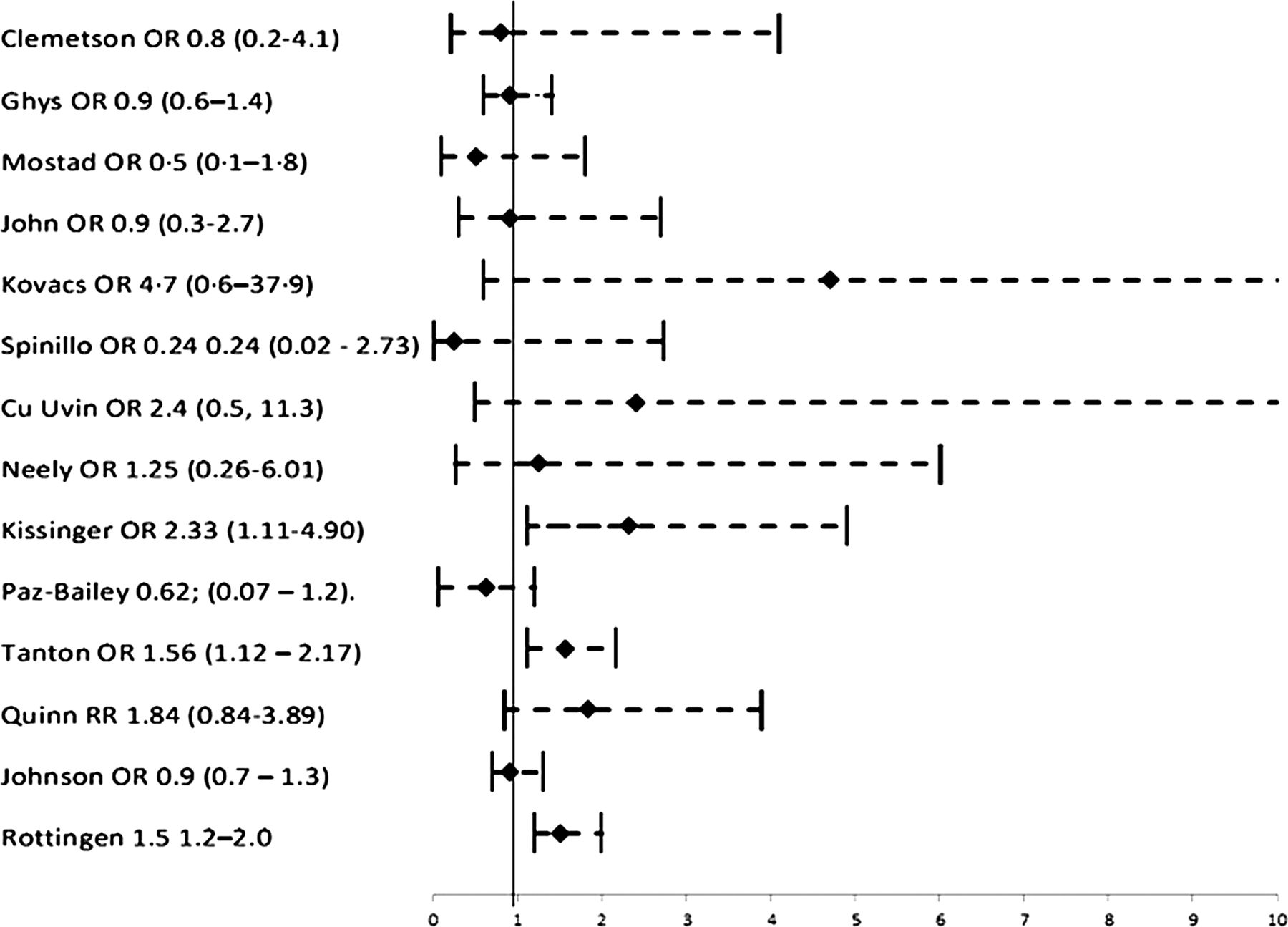
There were 14 studies that examined the association between TV infection and HIV acquisition and all of them found a positive association, 11 of which were statistically significant. Of these studies, nine were cohort, two were nested case-control and three were partner study designs (two cohort and one nested case-control designs). Most of these studies used either wet prep or culture as the diagnostic test for TV, which have lower sensitivity than amplification methods and would likely have under-represented asymptomatic women. All three of the studies that used nucleic acid amplification techniques found statistically significant elevated risk for TV infection and a subsequent HIV infection.
It is possible that TV may just be a marker of some other factor that causes HIV infection. However, all three of the serodiscordant partner studies, the strongest of the study designs for examining this issue, demonstrated positive associations. Two did not achieve statistical significance likely because they were underpowered (n=415 and n=90). Table 1 presents details of the studies and figure 1 presents the effect measures and their 95% CI.

Trichomonas and HIV acquisition.
Trichomonas and HIV acquisition
Using some of these studies as inputs, epidemiological modelling has demonstrated the potential role of TV on HIV transmission using data from the USA. Using population attributable risk curves, Sorvillo et al demonstrated that if TV amplifies HIV transmission twofold, as has been shown in some studies,25 ,27 and the prevalence of TV in a community is 25%, a rate commonly found among African American women studied, a fifth (20%) of HIV transmission in that population would be attributable to TV.31 This finding suggests that TV control may have an impact on the HIV-related disparities among African Americans in the USA. Quinlivan et al found similar findings. They estimated that 23% of the HIV transmission events from HIV-infected women may be attributable to TV infection when 22% of women are co-infected with TV, suggesting the importance of TV control among HIV+ women. 32 Chesson et al estimated that, in the USA, 747 new HIV cases a year in women are a result of the facilitative effects of TV on the transmission of HIV,33 proposing that TV control may be a cost savings initiative.
TV and HIV shedding
HIV shedding in the genital tract can theoretically increase the chance of HIV transmission; however, the amount of HIV needed for transmission to occur is unknown. Unlike TV and HIV acquisition, the association of TV on HIV genital shedding is less clear. There were 14 original studies (including one discordant partner study), one meta-analysis and one review paper that examined TV and HIV genital shedding. Of the 14 studies, over half (n=8) found an increased risk. The meta-analysis/review papers were also mixed. Many of these studies had small sample sizes and did not control for several key confounding variables, which could account for the variability in findings. Genital shedding of HIV, particularly among women, can be influenced by several factors. Among these factors are: plasma viral load, antiretroviral therapy (ART) status, other STIs, vaginal douching and unprotected sex with an HIV+ person. Therefore, studies of genital shedding must be adequately powered and well designed to reduce this potential confounding.
Other cofactors may increase TV-associated genital shedding. In a cohort of HIV+ women in New Orleans, USA, bacterial vaginosis (BV) seemed to act synergistically with TV to increase genial shedding. In this study, the odds of shedding HIV vaginally in the presence of TV alone, BV alone and TV/BV co-occurrence were 4.07 (95% CI 1.78 to 9.37), 5.65 (95% CI 2.64 to 12.01) and 18.63 (95% CI 6.71 to 51.72) respectively when compared with women with no diagnosis of TV or BV and adjusted for age, ART status and plasma viral load.34 The vaginal ecology may play an important role in sexual acquisition and transmission of HIV.
And while there is mounting evidence that ART status may be one of the most important preventive measures to reduce HIV genital shedding and consequently HIV transmission, there is evidence that even if plasma HIV is well controlled, HIV may still be expressed in genital fluids.35 Thus, measures to further reduce transmission beyond ART provision are needed. Table 2 presents details of the studies and figure 2 presents the effect measures and their 95% CI.
{kind=link}
{kind=link}
Trichomonas and HIV genital shedding. *The findings of Hobbs39 and Price42 are not shown in the figure because they did not present effect measures.
Trichomonas and HIV genital shedding
While the association of TV infection on HIV genital shedding among HIV+ person has not been consistent, there is good evidence that TV treatment reduces HIV genital shedding. Five studies were reported in the literature and, of these, four found a decrease in HIV genital shedding after TV treatment. The one study that did not find an association had a sample size of 31. Two prospective studies in Africa 50 51 where women were not receiving ART, and one study in the USA where about half of the women were receiving ART45 found that HIV genital shedding decreased after TV treatment, suggesting a role for TV treatment in HIV prevention beyond ART provision. These findings may not be generalized to men since there are far fewer studies of both acquisition and transmission among men (see table 3).
TV treatment and HIV shedding
Potential mechanisms whereby HIV amplifies HIV transmission
There are several possible mechanisms by which TV can increase susceptibly to HIV-1 including the aberrations caused by the inflammatory process, disruption of the mechanical barrier and impaired immune response.53 TV infection typically elicits an aggressive local cellular immune response with inflammation of the vaginal epithelium and exocervix in women and the urethra of men.10 The normal flora and pH are altered, producing a conducive environment for HIV-1 to pass through the cervicovaginal epithelium and mucosa infecting the host immune system.
TV may also increase the risk of HIV-1 acquisition by increasing susceptibility to BV or persistence of abnormal vaginal flora. When the normal flora of the vagina is disturbed there is a decrease in the proportion of H2O2 producing lactobacillus, which function to maintain a low vaginal pH.54 Without H2O2 producing lactobacillus the pH of the vaginal mucosa rises and pathogens that could not otherwise survive can now flourish. Decreased proportions of H2O2 producing lactobacillus and increased proportion of anaerobes have been associated in women infected with TV.55 56 In in vitro studies, lactic acid from all species of lactobacilli and H2O2 producing species have shown virucidal properties.57
An intact vaginal multilayered squamous epithelium provides a natural barrier to infection, as it does not appear to be susceptible to endocytosis and transcytosis of the HIV-1 virons. HIV-1 has been shown to pass though the thin gaps between squamous epithelial cells which could bring the virus into contact with CD4 T lymphocytes and Langerhans cells.58 Microabrasions caused during sexual intercourse removes the surface of the epithelium exposing the basal and stroma layers, weakening the barrier protection. TV frequently causes punctuate mucosal haemorrhages, which potentially compromises the mechanical barrier to infection. The epithelium of the cervicovaginal tissue is also disrupted by TV leading to the characteristic colpitis macularis, ‘strawberry cervix’ appearance and friability.59 These breaks in the surface epithelium facilitate the entry of HIV-1.
Vaginal innate mucosal immunity can become suppressed in the presence of TV. The main effector molecules of the innate mucosal immunity are cationic antimicrobial polypeptides, including secretory leukoprotease inhibitor (SLPI) and human B defensins, which work by downregulating inflammatory responses of macrophages and monocytes.60 It has been reported that SLPI has virucidal properties against HIV-1 in vitro.60 TV has been shown to decrease SLPI and other innate immune factors.61 The suppressed innate immunity can also allow other pathogens to flourish. There is some evidence that there may be some non-infectious causes of inflammation that increase cervicovaginal HIV-1 shedding.
TV induces a clinical or subclinical pro-inflammation of the cervix and vaginal tissues. Inflammation is a protective reaction in response to infections from vaginal pathogens.62 Women who are infected with TV show increased levels of neutrophils, interleukin 1B (IL-1B), IL-8 and macrophage inflammatory protein three α (MIP-3α), which are markers of a pro-inflammatory response.62 63 Langerhans-like CD34 progenitor dendritic cells are effective antigen presenting cells that are recruited to the vaginal mucosal surface by the chemokine MIP-3α.63 Macrophages, dendritic cells, and CXC4 and CCR5 expressing T lymphocytes are densely located in the subepithelia stromal tissues in the vagina. HIV most likely uses CD4/CCR5 intraepithelia cells, such as lymphocytes and Langerhans, to cross the mucosal surface and infect CD4 T lymphocytes.64 The inflammatory response induces the recruitment of leukocytes including HIV target cells such as CD4 bearing lymphocytes and macrophages to which HIV can bind and gain access. By activating the inflammation pathways and mediators, HIV target cells are localised to the site of inflammation. This facilitates the uptake of the viral particles and subsequent infection.
TV treatment issues among HIV positive women
Treatment of TV with single dose metronidazole (MTZ) is imperfect. High repeat infection rates (8%–20%65–70) among women receiving 2 g dose of MTZ for the treatment of TV have brought into question the effectiveness of single dose treatment.
In a study of HIV-/TV+ women who were given directly observed single dose MTZ and provided with medication to deliver to their sex partner(s), repeat infections rates were high (8%) and nearly all (92%) were attributed to clinical treatment failure,11 suggesting that clinical failure is the reason for lack of efficacy of single dose MTZ.
Re-infection from an untreated partner is another potential source of repeat infections. Patient-delivered partner treatment (PDPT), or the provision of antibiotics to infected index persons to deliver to their sex partners, is a possible alternative to the standard of partner referral or telling the index woman to refer her partner for care. While PDPT has been found to be superior to standard partner referral methods for reducing repeat Chlamydia trachomatis and Neisseria gonorrhoeae infections,24 the efficacy of PDPT for TV is less clear. Two published randomised controlled trials (RCTs) of PDPT for TV given to index women to deliver to their male sex partners found conflicting results.13 ,25 However, these studies were single centred and likely underpowered, and thus larger multi-centred trials are needed. One study of HIV+/TV+ women demonstrated high adherence to PDPT71 suggesting that, while Centers for Disease Control and Prevention have not yet recommended PDPT for HIV+ women, it may be a feasible option.
Repeat infection rates appear to be particularly high among HIV+ women ranging from 18.3% to 36.9%,13 66 72 suggesting that some factors specific to HIV+ women may be interfering with single dose MTZ therapy. A recently completed RCT among HIV-infected women with TV found multi-dose MTZ to be superior to single dose treatment.22 This RCT also found that the presence of BV was likely a major factor in the early failure of the single dose treatment.73 Another study corroborated these findings and found that women who were receiving nevirapine-containing ART had higher rates of treatment failure74 Subsequent analysis of the US-based study also found that ART interfered with MTZ treatment of TV.75 These studies suggest that ART may reduce the efficacy of MTZ. There are also data indicating that BV may play a factor in MTZ treatment failure.73
The Centers for Disease Control and Prevention guidelines for treatment of TV include: MTZ or tinidazole 2 g single dose as the recommended regimens, and MTZ 500 mg twice daily 7 day dose as the alternative treatment regimen, but suggest that for HIV+ women the multi-dose therapy can be considered.21
Prevention of TV
Prevention of TV for HIV+ persons is similar to those for HIV- persons. Primary prevention includes promotion of condoms and other safer sex activities to reduce the chance of exposure. There is some evidence that nonoxynol-9 can be used as an antitrichomonal agent;76 thus, condoms that contain nonoxynol-9 may also serve to prevent trichomonal infections. Secondary prevention includes screening and prompt treatment. Periodic presumptive treatment among female sex workers in Papua New Guinea demonstrated a twofold decrease in TV.77 Increased use of improved diagnostics in women is needed.
Since TV testing for men is difficult and the majority of TV-infected men are asymptomatic,78 partner treatment is paramount to reducing early repeat infections in women. Clinicians should consider diagnosis and treatment of TV in men. The influence of male circumcision on incident TV has demonstrated both protective effects among men and women79 and no effect among men.80
Conclusions
The evidence is clear that TV is associated with HIV acquisition among women. And while less clear that it is associated with increased genital shedding of HIV among HIV+ persons, it is clear that TV treatment reduces vaginal shedding. While it is unknown how much genital HIV is needed to transmit HIV, we do know that it is a necessary, but not sufficient, factor and evidence is mounting that while ART can significantly reduce plasma viral loads, there may be reservoirs of genital HIV and this could increase transmission.
Given the high rates of TV in populations in HIV vulnerable populations and among HIV+ persons, TV should be given higher priority for STD control programmes. At a minimum, HIV susceptible women in areas with high rates of HIV should be screened for TV. In addition, HIV+ women should be consistently screened and treated with multi-dose MTZ to prevent the possibility of perinatal and sexual HIV transmission.
Key messages
-
There is strong evidence that Trichomonas vaginalis (TV) increases both transmission and acquisition of HIV among women, and thus diligence in screening and treating TV among HIV susceptible and HIV+ women is an important public health strategy.
-
Treatment of TV among HIV+ women may require multi-dose of metronidazole given the high rates of asymptomatic bacterial vaginosis co-infections, changes in vaginal ecology and impaired immunity of HIV+ women that may interfere with single dose treatment.
-
Prevention of TV among HIV+ women is similar to HIV- persons, but special attention should be paid to prevent recurrent infections which are highly prevalent among HIV+ women.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online references
Footnotes
-
Contributors PK and AA designed the study, conducted the literature search and evaluated the papers.
-
Funding Funding for this review paper was from NIAID 1R01AI097080-01A1.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.