Article Text

Abstract
Objectives Infection with Trichomonas vaginalis has declined dramatically in urban Australia but remains endemic in some predominantly indigenous rural regions. The objective was to determine T vaginalis positivity rates in clinical specimens by PCR detection, from a large community-based private pathology laboratory servicing rural and urban Australian populations.
Methods Retrospective analysis of data from 44 464 specimens referred for T vaginalis PCR testing over 8 years from 2004 to 2011.
Results 44 464 consecutive specimens (37 137 female, 7242 male, 85 sex-unspecified) were analysed: T vaginalis was detected in 633 specimens. The overall community T vaginalis positivity rate was 1.4% (95% CI 1.3% to 1.5%). Overall rates were 2.1-fold higher in women than in men (1.5% vs 0.7%). Positivity rates were highest in the 10–14 year age group (p<0.0001). Referrals from urban areas of South-East Queensland accounted for 52% of specimens (23 121): the T vaginalis positivity rate in this urban cohort was 0.7% (95% CI 0.6% to 0.8%). Referrals identified to be from indigenous patients accounted for 48% of positive cases (304/633), and came from predominantly rural and regional areas of northern Queensland. Where follow-up testing was available 21% of patients (14/66) remained T vaginalis PCR positive when tested again within 3 months and 25% (26/101) within 6 months of the initial diagnosis.
Conclusions This study confirms that T vaginalis is rare in the urban non-indigenous Australian setting. Guidelines need to be developed to allow targeted testing. Follow-up testing 3 months after treatment should be considered.
- Trichomonas
- PCR
- Epidemiology (Molecular)
Statistics from Altmetric.com
Introduction
Trichomonas vaginalis (TV) is the most common, curable, sexually transmitted infection (STI) worldwide according to WHO estimates,1 however its prevalence is highly variable. In resource-limited countries the prevalence among women is usually high, ranging from 5–35%.2 Reported prevalence rates in the USA are 3.1% with much higher rates of 13.3% among non-Hispanic black women.3
In Australia rates have dramatically declined over the past 25 years with infection being virtually eliminated from urban areas. Reported prevalence of T vaginalis in women in a STI clinic setting in Australia peaked at 20–30% in the 1960s, declined to 5–10% in the 1970s, then fell to below 1% in the 1990s.4 Reasons attributed to the decline include improved access to healthcare, the introduction of metronidazole in 1961 and increasing surveillance through Papanicolaou (Pap) smears which were introduced in 1965.
The prevalence in remote, predominantly indigenous Australian populations remains similar to that found in resource-limited countries. A study by Bowden et al5 in 1999 of 1090 indigenous women in the urban, rural and remote areas of the ‘Top End’ of the Northern Territory (NT) of Australia attending for ‘well-women's checks’ showed an overall prevalence of T vaginalis of 25% using PCR detection in self-inserted tampons.
The NT is the only region in Australia where T vaginalis is a laboratory notifiable condition. Data from 2011 indicate that T vaginalis for the first time replaced Chlamydia trachomatis as the most frequently notified disease with a notification rate of 1264/100 000 population.6 An extremely high proportion (96.5%) of T vaginalis notifications was recorded in indigenous patients.
In contrast, prevalence of T vaginalis infection in women attending an urban Sydney sexual health clinic was found to be 0.4%, with 123 cases diagnosed over a 15 year period from 1992 to 2006.7 The true prevalence may likely be underestimated since the diagnosis was made by wet mount microscopy, which is less sensitive than other methods such as culture or PCR. Two other Sydney sexual health clinics, using PCR for T vaginalis detection in cervical specimens, reported a T vaginalis prevalence of 4.8%, with 17 cases diagnosed over 3 years from 2006 to 2008.8
Current US guidelines9 suggest that testing for T vaginalis be performed in women with symptomatic vaginal discharge and in asymptomatic women considered at high risk for infection (ie, women who have new or multiple partners, have a history of STIs, exchange sex for payment and use injection drugs). Rescreening for T vaginalis at 3 months following treatment can be considered due to the high rate of reinfection among patients in whom T vaginalis is diagnosed, with 16.5% culture positive within 3 months and 18.5% within 6 months in one study.10 The Australian National Management Guidelines for STIs suggest testing for T vaginalis in symptomatic females and in asymptomatic females if T vaginalis is ‘clinically suspected’.11 No recommendations are made for screening in males or for follow-up testing. NT guidelines12 suggest testing for T vaginalis in symptomatic and asymptomatic patients of both sexes.
There is a paucity of data with respect to the prevalence of T vaginalis in the Australian population, particularly in males, and there are no guidelines as to whether T vaginalis detection should become part of routine STI testing (except in the NT). This study provides an analysis of the T vaginalis positivity rate in specimens, from females and males, using PCR, from a large community-based Australian private pathology laboratory that services rural and urban Australian populations.
Methods
Setting and study period
Results of T vaginalis PCR testing on consecutive specimens referred to Sullivan Nicolaides Pathology (SNP) for T vaginalis testing over a period of 8 years from January 2004 to December 2011 were analysed retrospectively. SNP provides diagnostic services predominantly to community-based medical practices and private hospitals throughout Queensland and northern New South Wales.
Specimen sources
Specimens were tested where T vaginalis PCR was requested by the clinician. Dry swabs or those in chlamydial transport medium were accepted, in addition to ThinPrep fluids and tampons. Recommended urine samples were first stream samples where the patient had not urinated for 1–2 h prior to collection. Specimens were transported to the laboratory under ambient conditions then stored at 4°C. Testing was performed daily. There were no exclusions for delays in specimen processing although more than 85% were processed within 24 h of collection.
Laboratory methods
Specimens were tested for the presence of T vaginalis by real-time TaqMan PCR using primer and probe sequences with accession number L23861 targeting the T vaginalis-specific 2-kb repeated sequence and based on a method described by Schirm et al.13 To identify false negative reactions and extraction failures, Lactobacillus fermentum was used as an internal control. Until August 2009 conventional PCR targeting the β-tubulin genes of T vaginalis (bTUB2 and bTUB9) was used, in conjunction with 16S rDNA PCR inhibition controls, based on a method by Madico et al.14 Positive samples generated a 127bp PCR product detected on agarose gel electrophoresis. For both methods DNA extraction was performed using the MagNA Pure LC instrument and DNA isolation kit.
Data source and analysis
Data was extracted from the SNP laboratory information system using Crystal Reports. Specimen types were evaluated. T vaginalis positivity rates were stratified by age group and sex. Positivity rates were analysed for patients overall, in addition to those from designated postcodes in urban South-East Queensland. Overall positivity rates were determined for both laboratory methods, due to the change in PCR method during the study. Positivity rates were assessed following removal of duplicate results on patients with multiple specimens submitted during the 8-year study period.
Request forms from patients with positive results were scrutinised for information regarding clinical symptoms of vaginitis and the demographic source of the referral. Patients were identified to be of indigenous origin if they were resident in a known indigenous community or if they were referred by a doctor working in an indigenous health clinic. Details of ethnicity were sometimes available from clinical notes made by a pathologist when a positive result was telephoned to the requesting doctor.
Data regarding concomitant T vaginalis diagnosis by microscopy or Pap smear and concurrent C trachomatis and Neisseria gonorrhoeae detection were evaluated from patients with positive T vaginalis results where available.
Repeat testing of positive patients within 3 months and 6 months of the initial diagnosis was analysed.
χ2 calculations and 95% CIs were calculated using OpenEpi software V.2.3.1. Ethical approval was given at an institutional level in accordance with the National Health and Medical Research Council guidelines for low risk human research.
Results
Specimens
Forty-four thousand four hundred and sixty-four consecutive specimens (37 137 female, 7242 male, 85 sex unspecified) were referred for T vaginalis PCR testing during the study period. Testing was commenced in 2004, with a significant rise in the volume of testing in each successive year from 690 specimens tested in 2004 to 16 931 specimens in 2011. In August 2010 diagnosis by wet mount microscopy was ceased. Since this time requests for T vaginalis PCR escalated more than threefold, from around 500 per month to over 1500 per month.
The predominant specimen types in 2011 were urine (51%) and vaginal swabs (43%). In 2004 vaginal swabs were the most common specimen type (80%) compared with urine (20%). A variety of other specimen types were submitted during the study period, although numbers were low. These included ThinPrep fluids (301), urethral swabs (284), throat swabs (83), anal swabs (27), tampons (6), peritoneal fluid (1), eye swabs (2) and nasal swab (1). Of these additional sites T vaginalis was only detected in two ThinPrep fluids and the nasal swab from an infant with neonatal trichomoniasis.
Males comprised just 7% (49) of requests in 2004. The proportion of males tested increased during the study period to 15% (2604) of specimens in 2011. The mean age of women with T vaginalis was 29 years (range: 5 weeks–71 years), which was not significantly different from that of women without T vaginalis. The mean age of males with T vaginalis was 34 years (range: 15–71 years), which also was not significantly different from those without infection. T vaginalis was detected in a nasal swab of a 5 week old female infant with a nasal discharge and dry cough born to an indigenous mother with proven T vaginalis vaginitis.
Positivity rates
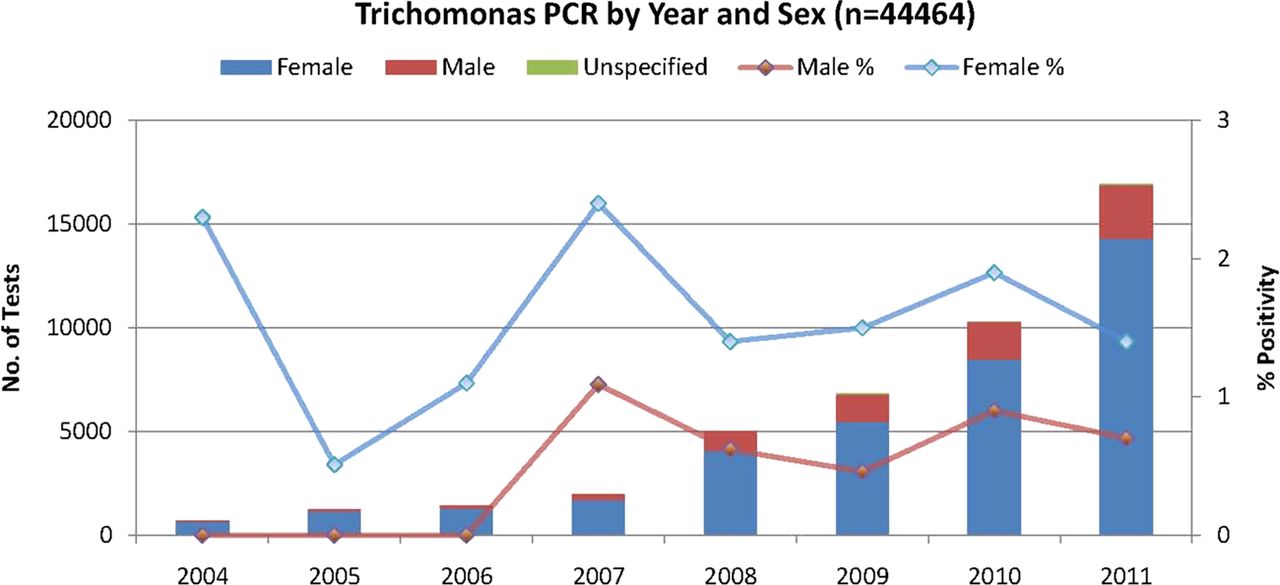
During the study period the overall positivity rate for T vaginalis was 1.4% (95% CI 1.3% to 1.5%), with T vaginalis detected in 633 of 44 464 specimens. The positivity rate was 2.1-fold higher among females than males at 1.5% and 0.7% respectively. Urban areas of South-East Queensland were identified by postcode and accounted for 52% (23 423) of the total number of specimens. In this urban population the positivity rate was 0.7% (95% CI 0.6% to 0.8%), with 165 specimens testing positive. PCR testing was unsuccessful due to the presence of inhibitors in 0.25% (113) of the total number of specimens. Figure 1 demonstrates T vaginalis PCR requests and positivity rates by year and sex throughout the study period.

Trichomonas PCR by year and sex.
T vaginalis positivity rates were higher (p<0.0001) in the 10–14-year-old and 15–19-year-old age groups (positivity rates of 4.4% (16/367) and 2.1% (153/7124), respectively) than in older age groups. Patients with T vaginalis detected in the 10–14 year age group were all ≥13 years and all of indigenous origin. The positivity rate was 1.1% in 20–29-year olds and 1.4% and 1.6% in 30–39-year olds and 40–49-year olds, respectively. A significant rise in positivity rate with age beyond 30 years was noted (p<0.001), compared with the 20–29-year age group. Age-specific positivity data is shown in figure 2.

{kind=link}
{kind=link}
Trichomonas positivity rates by age group.
Duplicate patients accounted for 4332 specimens (9.7%) over the course of the study period. When duplicates were removed from the data analysis the overall positivity rate was not significantly different at 1.3% (527/40 133). The overall positivity rate for specimens tested until July 2009 using the conventional PCR method was 1.3% (N=14 741); twice as many specimens were tested from August 2010 using real-time PCR with a positivity rate of 1.5% (N=29 723).
Clinical history and demographics
Vaginitis was indicated in clinical notes in 17% (96/572) of all T vaginalis-positive female patients. Female non-indigenous patients were more likely to have symptoms of vaginitis indicated on the request form (29%) than female indigenous patients (6.8%). Referrals identified to be from indigenous patients accounted for 48% (304) of the positive cases predominantly from rural and regional areas of northern Queensland.
Data on concomitant microscopy, Pap smears and STIs
T vaginalis microscopy was performed in 21% (136/633) of patients in whom T vaginalis was detected by PCR. The sensitivity of T vaginalis diagnosis using wet mount microscopy compared with PCR was 23% (95% CI 16% to 30%), with 31/136 samples positive. A Pap smear was performed concomitantly in 131 of the 633 T vaginalis PCR-positive patients. The sensitivity of Pap smears compared with PCR was 44% (95% CI 35% to 52%), with 57 samples noting the presence of T vaginalis.
Concomitant PCR diagnosis of C trachomatis was made in 67 patients and that of N gonorrhoeae in 12 patients with T vaginalis. Infection with all three pathogens was made in another 24 patients (of which 23 were indigenous). The overall rate of concurrent C trachomatis positivity was 15.6% and that of N gonorrhoeae 6.2% in patients with confirmed T vaginalis, which compares with a background community rate of C trachomatis and N gonorrhoeae positivity of 6.8% and 0.8%, respectively (SNP 2011, unpublished data).
Follow-up data
Follow-up within 6 months of the initial diagnosis was available on 106 patients who had initial positive T vaginalis PCR results. Five patients who were tested again and remained positive within 5–7 days of the initial test were excluded (since a positive result is not unexpected in this timeframe due to non-initiation of treatment or persisting T vaginalis DNA). T vaginalis infections were detected in 21% (14/66) tested again within 3 months of the initial diagnosis and in 25% (26/101) tested again within 6 months. One patient had T vaginalis detected 14 days after the primary test, however in all other cases T vaginalis was detected more than 30 days after the initial test. Negative follow-up test results were seen as early as 10 days following the primary positive test, with 14 patients having a subsequent negative result within 1 month. No specific characteristics were identified within the patients repeatedly testing positive.
Discussion
Evaluation of T vaginalis PCR data from testing of 44 464 specimens at SNP from 2004 to 2011 confirms that T vaginalis is rare in the urban Australian setting, with a total of 633 positive specimens and an overall positivity rate of 1.4% in the referred population. Urban referrals from South-East Queensland accounted for 52% of total specimens. Of these, 165 were positive, giving an urban positivity rate of 0.7%.
T vaginalis PCR is predominantly requested in females, with males comprising just 15% of requests in 2011. Overall 2.1-fold higher T vaginalis positivity rates were found in women (1.5%) compared with men (0.7%). Few studies have documented T vaginalis prevalence in males. However, a fivefold higher T vaginalis prevalence among women than men was noted in one US study.15 Given that most infections in males are asymptomatic accurate diagnosis was particularly limited prior to the introduction of nucleic acid amplification tests (NAAT). Lack of manifest symptoms in men may lead to reduced case finding. In addition, males are more likely to have transient or self-limited infection.16
Indigenous referrals, predominantly from rural and regional areas of northern Queensland, accounted for at least 48% of positive cases. In the 2011 census 3.6% of the Queensland population identified as being indigenous (Aboriginal and/or Torres Strait Islander).17 It is possible that more cases had an indigenous background, particularly since 35% of the indigenous population of Queensland live in the Brisbane region,17 however information on indigenous status was not uniformly available. SNP provides pathology services to the general community, excepting public hospital inpatients and emergency departments. Disadvantaged indigenous populations are less likely to access private pathology and thus may be under-represented. It is therefore likely that indigenous status is a risk factor for T vaginalis infection as has been shown in the NT.6
In most studies the prevalence of T vaginalis is seen to increase with age,3 ,5 ,18 in contrast with N gonorrhoeae and C trachomatis where infections are concentrated in women under 25 years of age.19 ,20 This is thought to be attributable to a long duration of infection combined with a low level of testing. In our study a significant rise in positivity rate with age beyond 30 years was noted, consistent with other studies, compared with the 20–29 year age group. However, T vaginalis positivity rates at 4.4% were highest in the 10–14 year age group than all other age groups. It was notable that all positive patients in this age group were of indigenous origin.
It is possible that non-sexual transmission of T vaginalis could contribute to the burden of T vaginalis in the younger age groups. T vaginalis has been shown to survive outside the human body in a wet environment for up to 3 h.21 ,22 The study by Crucitti et al23 demonstrated an overall prevalence of T vaginalis in 13–16-year olds in Ndola in Zambia of 27.1%, with a rate of 24.7% in virgins. They postulated that the high prevalence was due to non-sexual transmission of T vaginalis via shared bath water and inconsistent use of soap.
The presence of concomitant STIs in this age group suggests, however, that sexual transmission is most likely. The SNP 2011 positivity rates for N gonorrhoeae and C trachomatis in the 10–14-year age group were 1.3% (5/371) and 6.5% (35/534), respectively, compared with all age-group rates of 0.8% and 6.8% (N=58 919 for N gonorrhoeae and 88 166 for C trachomatis) (SNP unpublished data, 2011).
The sensitivity of wet mount microscopy for diagnosis of T vaginalis compared with PCR was 23% (31/136). This emphasises the importance of using NAAT, such as PCR, for adequate diagnostic sensitivity and supports the decision to move from microscopy in our laboratory. The sensitivity of T vaginalis detection in concomitant Pap smears was 44% (57/131), in keeping with rates found elsewhere.24 Detection through Pap smears may continue to be important in low-risk patients in whom T vaginalis screening is not indicated, however due to the low sensitivity should not be relied upon for diagnosis.
Patients with T vaginalis were more likely to have concomitant C trachomatis and N gonorrhoeae infection, with positivity rates of 15.6% and 6.2% respectively, compared with SNP background community rates of 6.8% and 0.8%. This supports the recommendation to screen for T vaginalis in patients presenting with other STIs.
Twenty-one per cent of patients were T vaginalis-positive up to 3 months and 25% patients up to 6 months after the initial diagnosis. This may represent lack of treatment, treatment failure or reinfection. These results confirm the importance of follow-up testing to document the efficacy of treatment and to detect episodes of reinfection. Theoretically it may be possible to detect residual T vaginalis DNA for some time following effective treatment. The study by Schirm et al13 suggested that T vaginalis DNA disappears within 2 weeks of treatment. In keeping with this, 14/15 patients in this study had a negative follow-up test from 7–30 days following initial diagnosis and presumed treatment. Resistance to nitroimidazoles, as an explanation for the high rate of recurrent T vaginalis detection, is thought to be low although this data comes from US studies rather than Australian studies.25
Limitations of the study include the change in PCR methodology in the course of the study period which may have impacted on results. Other limitations include the inability to stratify all patients by indigenous status and region. Logistic regression modelling to assess associated risk factors would have been beneficial. However, due to technical limitations of the database size and extraction capabilities it was not possible to assess for co-infection, Pap smear results, referral types and presence of symptoms in T vaginalis-negative patients.
In summary, a risk evaluation should be done prior to requesting T vaginalis NAAT in asymptomatic patients given the low prevalence in an urban setting. In such a setting the positive predictive value of the test is diminished. Adolescents at risk, especially young indigenous patients, should be particularly targeted for testing. Males should also be considered for testing. Follow-up screening 3 months after treatment is recommended.
Key messages
-
Trichomonas vaginalis is rare in urban Australia: overall positivity rates are 1.5% in females and 0.7% in males.
-
Testing for T vaginalis using nucleic acid amplification tests should be performed in symptomatic patients and screening requested in asymptomatic patients where risk factors exist.
-
Risk factors include detection of other sexually transmitted infections and indigenous status.
-
Screening 3 months after treatment should be considered to exclude reinfection or treatment failure given the high rate of T vaginalis detected in follow-up specimens.
References
Footnotes
-
Contributors JMB and JMR: designed the study, analysed and interpreted data. JMB: wrote the manuscript. JMR: contributed to and revised the manuscript and approved the final published version.
-
Competing interests None.
-
Ethics approval This study was conducted in accordance with the NHMRC National Statement on Ethical Conduct in Human Research, deemed to be ‘low risk’ research and approved by the SNP institutional Ethics Review Body.
-
Provenance and peer review Commissioned; externally peer reviewed.