Article Text

Abstract
Objectives The current study was conducted to synthesise evaluations of couple-based HIV prevention interventions, assess the efficacy of these interventions in reducing sexual risk, and identify moderators of intervention efficacy.
Methods A comprehensive literature search identified 29 interventions (22 reports; N=5168 couples) that met the inclusion criteria, including enrolment of both members of a heterosexual couple, measurement of condom use at baseline and follow-up, and sufficient statistical information to calculate effect sizes. Effect sizes were analysed using fixed-effects and random-effects assumptions; factors related to intervention efficacy were identified using metaregression.
Results Overall, there were significant increases in condom use from baseline to follow-up (d+=0.78, 95% CI 0.48 to 1.09) and significant decreases in partner concurrency (d+=0.37, 95% CI 0.13 to 0.60). Condom use increased to a greater extent when studies were conducted toward the beginning of the epidemic, were located in countries scoring lower on the Human Development Index, enrolled serodiscordant couples, and delivered intervention content in multiple contexts. Couples who had been together longer, reported higher incidence of sexually transmitted infection, were provided voluntary counselling and testing, and provided outcome measures during face-to-face interviews also reported larger increases in condom use.
Conclusions Couple-based interventions are efficacious in reducing unprotected sex within the context of romantic relationships. Future research should continue to improve risk reduction for couples.
- Prevention
- HIV
- Meta-Analysis
- Sexual Health
Statistics from Altmetric.com
According to WHO,1 there are 34 million people living with HIV (PLWH), nearly 70% living in sub-Saharan Africa. Within the USA, there are 1.2 million PLWH, with an estimated 48 100 new infections in 2009.2 Heterosexual transmission is rising, and women are roughly three times more likely to acquire HIV from a male partner than a man is from a female partner.3 Women now account for 52% of all HIV infections worldwide.1 In the USA, two-thirds of new heterosexually transmitted infections were contracted by women.2 Heterosexual relationships are often characterised by a sexual division of power,4 shared resources5 and shared sexual networks,6 which can lead to increased heterosexual transmission of HIV.7
For many couples, unprotected sex can be interpreted as intimacy and trust,8 acting as a barrier not only to condom use, but to communication about safer sex in general.9 Even within HIV-serodiscordant couples, condom use is inconsistent despite the immediate threat of transmission.10–12 Individuals within relationships may perceive themselves to be less at risk for HIV and other sexually transmitted infections (STI) due to their couple status, but may also underestimate their partner's risk.13–15
Partner concurrency can also place individuals in relationships at an increased risk for HIV. Estimates of partner concurrency vary widely (from 4% to 76%16–18). Partner concurrency is related to increased unprotected sex in some populations; Conley and colleagues found that ‘cheaters’ were less likely to use condoms with their main or outside partners, get regular STI tests, and disclose outside partners to their main partner compared with individuals in consensually non-monogamous relationships.19 Nineteen percent of participants in a couple-focused HIV-prevention intervention reported concurrent partners at baseline, and while condom use with main partners increased over the course of the intervention, there was no change in partner concurrency or STI incidence indicating that participants had unprotected sex with concurrent partnersw5 Studies examining HIV transmission within serodiscordant couples found that between 18% and 29% of new HIV infections originated from external partners.20–22
Despite early calls for couple-focused reproductive health interventions23 and recently published strategies1 and guidelines24 for the use of voluntary counselling and testing (VCT) and antiretroviral therapy to prevent transmission within serodiscordant couples, couple-based interventions are scarce. Previous meta-analytic work on VCT and interventions targeting condom use included only a handful of interventions targeting couples.25 ,26 A more recent meta-analysis of HIV prevention interventions for PLWH in developing countries included separate analyses for four studies comparing couple-based HIV counselling to individual-based counselling, but found no difference in risk reduction between the two formats.27 The only systematic review conducted to date that explicitly examined the efficacy of couple-based HIV prevention interventions included six interventions, and while the authors reported generally positive behavioural and condom use outcomes, they did not conduct a meta-analysis due to heterogeneity among studies.28
The goal of the present meta-analysis was to extend previous reviews by including more recent literature, determining the efficacy of couple-based HIV interventions in increasing condom use with both main and concurrent partners, and identifying moderators of intervention efficacy. We hypothesised that couple-based HIV interventions would significantly increase condom use with study partners, and would increase condom use with concurrent partners to the extent that interventions addressed concurrent partnerships. We also explored commonly identified predictors of behaviour change as identified by past reviews (eg, provision of behavioural skills training26) and included couple-specific moderators (eg, serodiscordancy25).
Methods
Literature search
The current meta-analysis adhered to PRISMA guidelines.29 Relevant studies were located using several search strategies. First, we searched electronic databases (PubMed, PsycINFO, CINAHL, Eric, Psychology and Behavioural Sciences, and ProQuest Dissertations and Theses) using Boolean operators: (couple* OR partner*) AND (HIV OR “human immunodeficiency virus” OR AIDS OR “acquired immune deficiency syndrome” OR STD OR “sexually transmitted” OR STI). Next, all available issues of several relevant journals (eg, AIDS & Behavior, JAIDS) and conference abstracts for the 2012 International AIDS Conference were searched online. Finally, reference lists of prior meta-analyses, reviews and included reports were searched to identify additional reports. Reports available by 1 January 2013 were included in the present meta-analysis; details of the full search strategy are provided in appendix A, supplementary web content.
Inclusion criteria
Studies were included if they (1) examined the efficacy of a couples-based HIV/AIDS-related behavioural intervention, (2) recruited and enrolled both members of a self-identified couple, (3) delivered some/all intervention content to both members of a couple either concurrently, separately, or in a group setting, and (4) reported condom use outcomes at baseline and follow-up (see figure S1, supplementary web content). Studies were excluded if they (1) did not evaluate an HIV/AIDS-related behavioural intervention, (2) were conducted primarily to test medication adherence or efficacy, (3) did not provide sufficient statistics to calculate effect sizes (ES) for outcomes of interest, (4) enrolled only one member of a couple and (5) did not target heterosexual couples (originally, there were no restrictions based on couple sexual orientation, but only one report was identified targeting same-sex couples30). One additional report31 was excluded due to extreme over-reporting of condom use as determined by the authors of the study after comparing self-reports to biological markers. Studies did not have to incorporate a control group. Authors were contacted when additional information was needed to calculate ES (four of seven authors provided the necessary information; one author also provided an additional in-press study, which was included.w12 When studies reported evaluations of an experimental couples-based intervention and a comparison intervention that was HIV/AIDS-related and delivered to both members of a couple, the comparison was included as an additional couples-based intervention.
Coding and reliability
Two trained raters independently coded report information (eg, location), characteristics of interventions (eg, number of intervention sessions), and sample demographics (eg, relationship length). Inter-rater reliability for categorical variables was calculated as Cohen's κ (mean κ=0.79, median κ=0.84, mean agreement was 92%).32 Spearman–Brown correlations were calculated for continuous variables (mean r=0.93).33 Disagreements between raters were resolved through discussion. Interventions were also matched by country and year of initial data collection to the corresponding Human Development Index (HDI).34 ,35 The HDI is a measure of nation-level development that combines indices of life expectancy, educational attainment, and income; values can range between 0 and 1. According to the UN classification, countries are described as scoring high (HDI of 0.80 or above), medium (HDI between 0.50 and 0.79), or low (HDI between 0.50 and 0.79).
Calculation and analyses of ESs
To gauge the efficacy of each intervention, standardised mean differences, d, were calculated by subtracting the baseline mean from the first available follow-up mean and dividing by the pooled SD36; ds were corrected for sample size bias. When means and SDs were unavailable, other statistical information (eg, F-values) were used with the appropriate transformations.37 ,38 When studies reported dichotomous outcomes, ORs were calculated and transformed to d using the Cox transformation.39 The primary outcome measure was condom use with study partner. This measure included the proportion of participants reporting consistent condom use, frequencies and proportions of unprotected sex, and general condom use. Secondary outcomes included reported partner concurrency (eg, reported sexual intercourse with a partner other than the partner in the couple relationship) and condom use with concurrent partners.
When multiple measures of the same outcome were reported, ESs were averaged. When studies reported on more than one intervention condition, a separate ES was calculated for each condition. When studies included responses from both members of a couple, responses were averaged such that only one ES per outcome per intervention was included in analyses; ESs for men and women were highly correlated (r=0.97). Positive ESs indicate more sexual risk reduction following the intervention compared with baseline (eg, increased condom use, reductions in reports of concurrent partners). Two researchers calculated ESs independently and resolved discrepancies via discussion.
Analyses were conducted following fixed-effects and random-effects assumptions37 ,40 ,41 in Stata 11.2.42 The inference test of homogeneity, Q, and the homogeneity statistic index, I2, and its corresponding 95% CIs were calculated to determine the extent to which study outcomes were consistent.43 ,44 I2 provides homogeneity information on a scale from 0 to 100; higher values indicate increased heterogeneity (ie, more variation in study outcomes than would be expected by sampling error alone). Moderators of ES magnitude were examined using modified weighted least squares regression analysis with weights equivalent to the inverse of the variance. The moving constant technique was used to estimate mean ES (d+) and 95% CIs at specific moderator levels of interest.45 To test for potential reporting bias, asymmetries in the distribution of ES outcomes were examined using Begg's technique,46 trim and fill,47 and Egger's technique.48
Results
Description of studies
Twenty-two reports (see supplementary web content for references of included reports)w1–22 containing evaluations of 29 separate couple-based interventions met the selection criteria and were included (see table S1, supplementary web content). Interventions were conducted in the USA (k=15), Africa (k=10), the Caribbean (k=3), Asia (k=2) and Europe (k=1). Two interventions were conducted in multiple countries simultaneously. Participants were most commonly recruited through clinical contact, and two-thirds of those recruited agreed to participate. The average length of time from the last intervention session until first available follow-up was 7.64 months.
Overall, 5168 couples were enrolled in the 29 interventions. Across the participant samples, the mean age was 31 years old, average relationship length was 5.46 years, and 61% were married. Forty percent of individuals were living with HIV, and 18% reported having a concurrent partner. Ten interventions enrolled only serodiscordant couples and nine enrolled seroconcordant and serodiscordant couples. USA samples were, on average, 53% Latino/a, 36% African–American and 20% Caucasian. Nearly all participants (90%) attended all intervention sessions, and 78% of those present at baseline were present at the first available follow-up.
Seven of the 22 included reports simultaneously evaluated two separate couple-based HIV/AIDS prevention interventions. Only six reports incorporated a control group that either delivered intervention content to the female partner onlyw4 w16 w20 or delivered general health and wellness information to couples.w5 w6 w8 Thirteen interventions reported using a theory to guide intervention development. Interventions consisted of an average of about four sessions for a total of nearly 8 h of contact. Seventeen interventions reported providing condoms, 12 provided VCT, 7 reported addressing concurrent partners, 6 reported addressing gender, 6 reported addressing power, and 4 eroticised safer sex. Thirteen interventions included active condom use skills training (5 of which included practice with partner), and 11 interventions including active communication skills training (5 of which included practice with partner). Nine interventions reported a total of 71 seroconversions between baseline and last follow-up.
Overall efficacy of the interventions
Analyses indicated significant increases in condom use with study (or unspecified) partner from baseline to first follow-up (d+=0.94; 95% CI 0.56 to 1.33). After removing one extreme outlier that had an ES more than 3 SDs larger than the mean,w8 the mean ES for condom use remained significant (d+=0.78; 95% CI 0.48 to 1.09; figure 1; table 1). The hypothesis of homogeneity was rejected, and a large I2 value indicated large heterogeneity within study effects (I2=97.80; 95% CI 97.37 to 98.15). Trim-and-fill results showed no asymmetry for condom use with study partners; no missing studies were estimated. Begg's and Egger's tests were non-significant (Begg's z=1.76, p=0.08, and Egger's bias=4.32, t=1.70, p=0.10), suggesting no publication bias.
Mean effect sizes for study outcomes
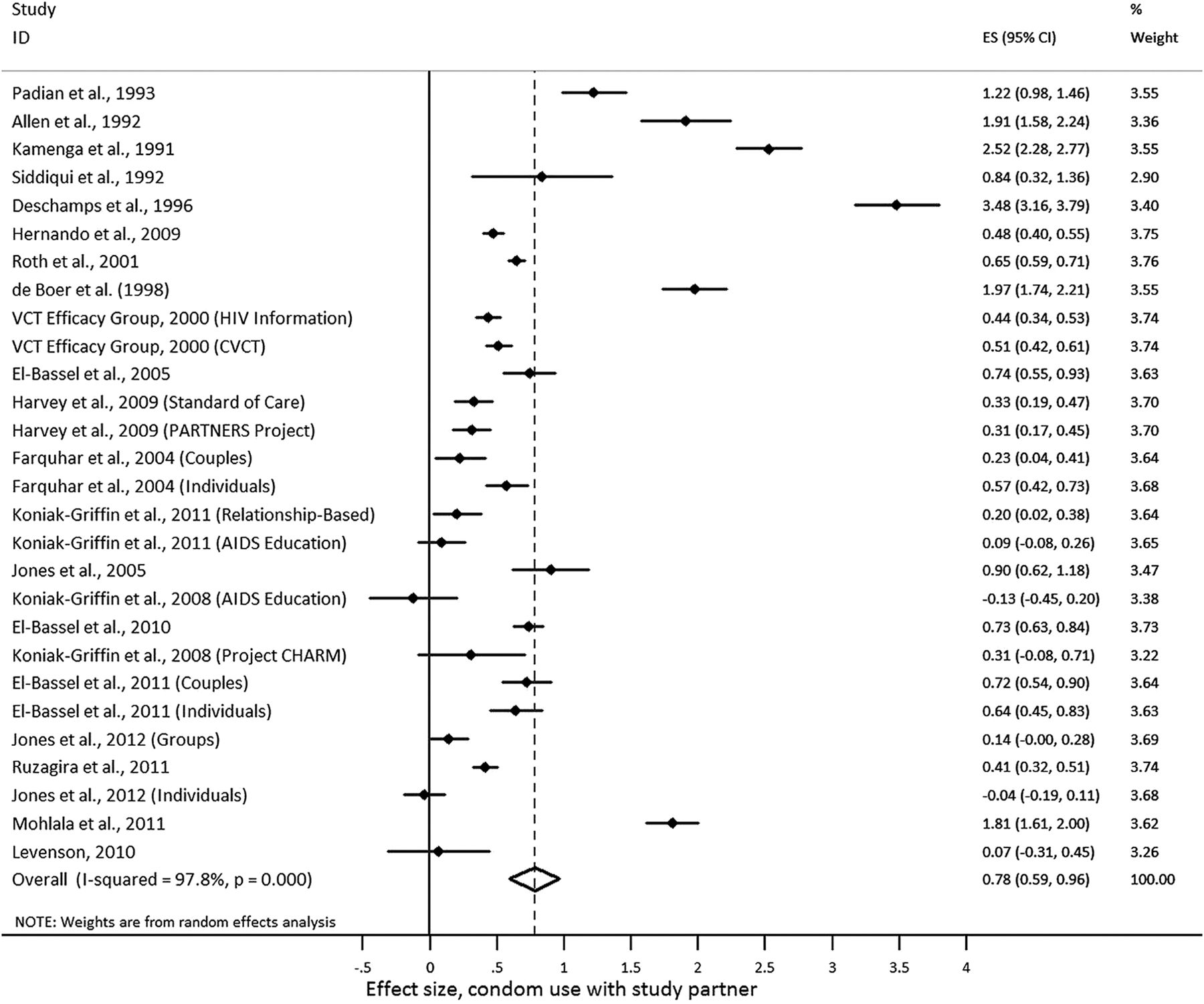
Effect size estimates for condom use with main partner. Effect sizes appear in temporal order of studies collecting earlier data first. Positive effect sizes indicate increased condom use with study partner at follow-up compared with baseline.
Analysis also indicated significant reductions in reported partner concurrency from baseline to first follow-up (d+=0.38; 95% CI 0.13 to 0.60; figure 2), with heterogeneity present among the ESs (I2=95.33; 95% CI 93.46 to 96.66). For reports of concurrent partners, trim-and-fill results estimated six missing studies; Begg's and Egger's tests were both significant (Begg's z=2.84, p<0.01, and Egger's bias=7.59, t=4.11, p<0.01), suggesting publication bias. Yet, the fact that there was heterogeneity implies that more complex models are necessary (whereas, these statistics assume only a single population ES49).

{kind=link}
{kind=link}
Effect size estimates for partner concurrency. Effect sizes appear in temporal order of studies collecting earlier data first. Positive effect sizes indicate decreased reports of concurrent partners at follow-up compared with baseline.
ESs were not calculated for condom use with concurrent partners, as only one study reported this outcome.w22 Moderator analyses were conducted for condom use with study partner, but not reported partner concurrency, due to the small number of studies reporting a concurrency outcome and the suggested publication bias with regard to concurrency outcomes. Due to heterogeneity in study outcomes, further analyses used only random-effects assumptions.
Condom use with study partner
Several study dimensions related to ES magnitude (see table 2). Studies that were conducted toward the beginning of the epidemic and in lower HDI countries showed larger increases in condom use. Interventions that included couples who had been together for a longer period of time, included participants with STIs other than HIV, enrolled serodiscordant couples, provided VCT, had longer follow-up periods, or used face-to-face interviews to collect outcome data, all had larger ESs. When interventions included condom skills training, ES were larger to the extent that condom skills were practiced with study partner, and to the extent that interventions presented content in a variety of contexts. Interventions delivered to individuals or individual couples also showed significant increases in condom use, but interventions delivered only to groups did not. Interventions that delivered intervention content in more sessions tended to have larger ES, but this relationship did not reach statistical significance. No other coded sample characteristics (eg, age, proportion African–American, Latino, married, unemployed, reporting illegal drug use or concurrent partners) or intervention dimensions (eg, theoretical background, condom provision, or inclusion of information about gender, power, culture, or concurrent partners) were significant predictors of ES magnitude.
Moderators of effect size magnitude for condom use with main partner
Discussion
This meta-analysis is the first to assess the efficacy of couple-based HIV/AIDS prevention interventions and to identify moderators of intervention efficacy. Overall, couple-based HIV/AIDS prevention interventions significantly increased condom use with main partners from baseline to follow-up, and significantly decreased the proportion of participants reporting concurrent partnerships from baseline to follow-up, although there was marked heterogeneity in effects. It was expected that condom use with other partners would vary based on whether interventions addressed concurrent partnerships, but only one study investigated change in condom use with outside partners, making it impossible to test the second hypothesis.
Comparison with other studies
The mean ES for change in condom use was larger for couple-based interventions included in the current study (d+=0.78; 95% CI 0.48 to 1.09) than for individual-based and group-based interventions included in one prior meta-analysis (d.=0.29; 95% CI 0.24 to 0.34),25 but comparable with the ES found for a reduction of unprotected intercourse among discordant couples in a meta-analysis examining the efficacy of VCT on sexual risk behaviour (d+=0.75; 95% CI 0.59 to 0.92).24 The results of this meta-analysis also showed larger increases in condom use for interventions enrolling only serodiscordant couples (d+=1.50; 95% CI 0.80 to 2.21), consistent with previous results (d+=1.31; 95% CI 1.14 to 1.48).24 This larger increase in condom use for serodiscordant couples is likely due to greater risk perceptions among HIV-uninfected individuals in serodiscordant relationships compared with individuals in relationships where both partners are uninfected. Increased risk perception also explains why increases in condom use were larger to the extent that interventions enrolled participants with other STIs.
The results of this meta-analysis are consistent with prior studies indicating that interventions achieve better risk-reduction results when they take place in countries with a lower HDI index; interventions appear to work best where need is greatest,50 ,51 at least on relatively short-term assessments. Interventions with more intervention content, as measured by the number of intervention sessions, also trended toward greater efficacy in increasing condom use.52 Contrary to the results of previous meta-analyses of behavioural interventions for HIV prevention,26 ,52 no current evidence indicated that interventions with more skills training resulted in greater increases in condom use. Nonetheless, among interventions that provided skills training, condom use increased more to the extent that participants practiced condom use skills with their partner. It is possible that interventions that promote condom use, and include active condom use skills training to both members of a couple simultaneously, may lead to more positive condom attitudes and more supportive social norms,5 ,25 ,53 ,54 as well as shared responsibility for risk reduction.55
Limitations
Despite widespread calls for couple-focused HIV prevention programmes, only 22 reports evaluating 29 interventions qualified for the present meta-analysis. Still, the present meta-analysis builds on prior reviews by including recent reports, reflecting the current state of the research regarding couple-based interventions. The majority of studies included were conducted in the USA and in African countries, so it is difficult to generalise results to couples in other countries. Conclusions are limited by the content reported by authors in manuscripts, and at this point in time, there is only minimal evidence suggesting what specific intervention components will lead to the most risk reduction. Additionally, our search strategy only located one study reporting on the efficacy of a couple-based HIV intervention for same-sex couples,30 and while many studies measured partner concurrency at baseline and follow-up, few reported addressing concurrent partnerships and only one measured condom use with concurrent partners. There was also evidence of publication bias regarding partner concurrency. It is possible that researchers may not report changes in partner concurrency outcomes after completion of a couple-based intervention, especially if individuals report no change or increases in partner concurrency.
The current meta-analysis is also limited in having included studies that were of varying methodological quality. For example, few studies included comparison groups, and among those that did, content, duration and mode of delivery varied; no study included a waitlist or no-treatment control group. ESs were also calculated based on self-report data, and increases in condom use were larger to the extent that data was collected in face-to-face interviews. While self-reports can be useful, it is important to collect them in a non-reactive fashion so as to reduce the extent to which participants are influenced by social desirability. Additional details regarding the limitations of couple-based HIV prevention efforts have been previously published.55
Future directions
Aside from increasing the development, testing and availability of couple-based interventions targeting various populations, additional information about implementation is needed. Future prevention efforts for couples should evaluate the efficacy of addressing gender roles and power dynamics within relationships. As very few interventions in the present meta-analysis reported including these components, their role in couple-based intervention efficacy is largely unknown. There is evidence, nonetheless, that reducing depression among women,56 including gender-specific content, empowering women and addressing power in relationships is related to reductions in risky sexual behaviour.57 Many other studies have linked unequal power in relationships to risky sexual behaviour.58–61 Clearly, future couple-based interventions should address these concerns as well as others such as disclosure of risk factors,10 ,11 shared resources and social networks,5 and eroticisation of safer sex.62 The results of the present meta-analysis also indicate that delivering intervention content in multiple formats (eg, incorporate both couple-only as well as group formats) and providing active skills training with one's partner can promote risk reduction. Finally, the role of concurrent sexual partners in HIV transmission continues to be debated. Some researchers stress that there is no empirical basis for the idea that concurrent partnerships increase HIV transmission above and beyond what would be expected from having multiple, non-concurrent sexual partners63; others argue that limited HIV prevention resources should be directed toward implementing interventions shown to decrease sexual risk by decreasing overall numbers of sexual partners as opposed to decreasing partner concurrency in particular.64
Conclusions
The results of the present meta-analysis demonstrating increased condom use and decreased partner concurrency among couples participating in interventions are encouraging, but we are far from a comprehensive understanding of how relationship dynamics contribute to increased HIV transmission risk, or how relationship dynamics may be harnessed to reduce HIV transmission. The small number of available couple-based HIV interventions and increasing calls for couple-based prevention strategies9–11 ,55 suggest that researchers are likely to target prevention efforts toward couples in the near future. Additionally, in its global health sector strategy on HIV/AIDS, 2011–2015, WHO outlined plans to increase HIV counselling and testing for couples in an effort to reduce transmission between serodiscordant partners1 and has recently published guidelines on couple-based VCT.24 Researchers should continue to develop and test the efficacy of couple-based HIV prevention efforts.
Key messages
-
This meta-analysis is the first to assess the efficacy of couple-based HIV/AIDS prevention interventions, and to identify moderators of intervention efficacy.
-
Couple-based HIV/AIDS prevention interventions increased condom use with main partners and decreased partner concurrency from baseline to follow-up.
-
Moderators of intervention efficacy included year of data collection, Human Development Index scores, and delivery of intervention content in multiple contexts.
-
Serodiscordancy, length of relationship, STI history, VCT and practicing condom skills with one's partner were all related to larger increases in condom use.
-
Future research should evaluate the efficacy of interventions that address gender roles, power in relationships, risk disclosure and eroticisation of safer sex.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
- Data supplement 3 - Online references
- Data supplement 4 - Online table
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors JML performed the literature search, selected, acquired, and coded studies, calculated effect sizes, analysed the data, and led the writing of the article. JAP assisted with the literature search, selection of studies, coded studies, and calculated effect sizes. CAL assisted with selection of studies and data interpretation. BTJ assisted with data interpretation. All authors assisted with study conceptualisation and provided critical revisions of the article.
-
Funding This work was supported by the National Institute of Health under U.S. Public Health Service Institutional National Research Service Award number T32-MH074387 and grant number R01-MH58563.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.