Article Text

Abstract
Objectives To examine the association between prior chlamydia and gonorrhoea infections and adverse obstetric outcomes.
Methods Records of women resident in New South Wales, Australia with a singleton first birth during 1999–2008 were linked to chlamydia and gonorrhoea notifications using probabilistic linkage. Obstetric outcomes and potential confounders were ascertained from the birth record. Logistic regression, adjusted for potential confounders was used to estimate the association between a disease notification prior to the birth and adverse birth outcomes: spontaneous preterm birth (SPTB), small for gestational age (SGA) and stillbirth.
Results Among 354 217 women, 1.0% (n=3658) had a prior chlamydia notification; 0.06% (n=196) had a prior gonorrhoea notification. The majority of notifications (>80%) occurred before the estimated conception date. 4.1% of women had a SPTB, 12.1% had a SGA baby and 0.6% of women had a stillbirth. Among women with a prior chlamydia notification, the risk of SPTB and stillbirth was increased, aOR 1.17 (95% CI 1.01 to 1.37) and aOR 1.40 (95% CI 1.00 to 1.96) respectively but there was no association with SGA, aOR 0.99 (95% CI 0.89 to 1.09). For women with gonorrhoea the risks for SPTB, stillbirth and SGA were respectively aOR 2.50 (95%CI 1.39 to 4.50), 2.35 (95% CI 0.58 to 9.56) and 0.98 (95% CI 0.58 to 1.68). Among women with a prior chlamydia diagnosis, the risk of SPTB did not differ between women diagnosed >1 year prior to conception, within the year prior to conception or during the pregnancy, (p=0.9).
Conclusions Sexually transmissible infections in pregnancy and the preconception period may be important in predicting pregnancy outcomes.
- Chlamydia Infection
- Public Health
- Reproductive Health
- Epidemiology (General)
Statistics from Altmetric.com
Introduction
Diagnoses of sexually transmitted lower genital tract infections, in particular chlamydia, have been increasing rapidly among young adults in many countries although it is unclear what proportion may be due to increased testing.1 ,2 Some studies suggest that infections such as chlamydia and gonorrhoea diagnosed during pregnancy may predispose women to serious adverse obstetric outcomes such as spontaneous preterm birth (SPTB), low birth weight and stillbirth but other studies have not found such associations.3–5 This may be due to inconsistent outcome definitions and limited consideration of other factors contributing to poor outcomes, such as smoking during the pregnancy.6 ,7 It has also been suggested that in relation to preterm birth, the timing of genital tract infections is important, with infections occurring earlier in the pregnancy and potentially prior to conception having a role.8 As most studies have limited their analyses to infections diagnosed during pregnancy rather than prior to conception, in this report we sought to investigate the associations between a prior diagnosis of chlamydia or gonorrhoea, the timing of the diagnosis in relation to the pregnancy, and the likelihood of serious obstetric outcomes (SPTB, small for gestational age (SGA) and stillbirth) in a large cohort of women having their first birth.
Methods
This study was conducted using record linkage of two statutory databases in New South Wales (NSW), Australia's most populous state with over 7 million inhabitants. The NSW Perinatal Data Collection includes all births in NSW (defined as ≥20 weeks’ gestation or birth weight ≥400 g) and records are available for linkage from 1994. Each record includes parity, information on antenatal risk factors such as hypertension, diabetes and smoking, the labour and delivery details including labour onset, and neonatal information including gestational age and birth weight. The NSW Notifiable Conditions Information Management System9 contains a record of all diagnoses of conditions considered notifiable under Australia's Public Health Act. In NSW laboratories and health practitioners are required under statute to notify diagnoses of genital chlamydia and gonorrhoea. Other infections including syphilis, hepatitis B and hepatitis C are also notifiable. Records for all conditions are available from 1994 except chlamydia, which only became notifiable in NSW from 1998. The records include identifying details of the individual, the condition notified, the onset date (for chlamydia and gonorrhoea this is equivalent to the specimen collection date) and the type of specimen. Notifications are made based on standard case definitions.10 Records from both datasets collated up until 31 December 2008 were available for this study.
The personal identifying details (name, date of birth, sex, address) from each data collection were used to probabilistically link records from all birthing mothers to disease notifications. The linkage was conducted independently by the NSW Centre for Health Record Linkage (CHeReL) using record linkage software and full details are available on the CHeReL website.11 The validity of probabilistic linkage was extremely high12 for this study; the CHeReL reported the false positive and negative linkages as <0.5%. Records belonging to individual women were assigned a unique number and deidentified records were provided to the researchers for analyses. The study was approved by the NSW Population and Health Services Research Ethics Committee, the University of NSW Human Research Ethics Committee and the NSW Aboriginal Health and Medical Research Council Ethics Committee.
Definitions
A woman was defined as having a SPTB if she had a spontaneous labour with delivery at <37 weeks gestation or if the gestational age was missing (0.02% of records), a birth weight <1500 g. We also included in the definition of SPTB women who had preterm rupture of membranes and were subsequently induced with a live birth at <37 weeks. Other births with delivery <37 weeks gestation that were induced were classified as a ‘planned preterm birth’. SGA was defined as <10th centile birth weight for gestational age by infant sex.13 Stillbirths were identified in the birth record.
Women were categorised as having a history of chlamydia or gonorrhoea infection if they linked to a past notification record for either infection. Only notifications where the onset date occurred before the woman's delivery date were considered and if a woman had more than one notification of the same infection, the date was taken as the one closest to the date of delivery. The timing of the chlamydia notification in relation to the outcome of SPTB was also examined by classifying women into three categories, those with a notification at >1 year prior to the estimated conception date, within 1 year prior to the estimated conception date or during the pregnancy.
Analyses
Analyses were restricted to women resident in NSW who had a record of a first singleton birth, between 1999 and 2008 in the Perinatal Data Collection. Each of the three outcomes, SPTB versus term birth, SGA versus not SGA and stillbirth versus live birth were examined separately, however outcomes were not mutually exclusive (eg, stillbirths could also be classified as SGA). Logistic regression was used to estimate associations with a notification record of either chlamydia or gonorrhoea. Analyses included the potential confounders, maternal age (in 2.5 year age categories from <17.5 years to ≥37.5 years), socioeconomic status (in quintiles based on a standard index using Australian census information and residential postcode14), area of residence (major city vs not major city15), Aboriginality (based on a woman being reported as Aboriginal or Torres Strait Islander or both on the perinatal record; ascertainment of Aboriginality used information from all of a woman's perinatal records, not just the first birth, based on methods previously described16), country of birth (Australia or overseas), year of giving birth (as a continuous variable), smoking during the pregnancy (yes/no), late booking for antenatal care (>20 weeks vs ≤20 weeks gestation), hypertensive disease (yes/no), gestational and pre-existing diabetes (yes/no). The presence of other notifiable infections including syphilis, and hepatitis B and hepatitis C were categorised separately. In this report syphilis was not a focus as its association with the outcomes of interest is well established17 and it is uncommon in this population,18 thereby limiting statistical power in analyses. Information on HIV was not available to be linked, but its prevalence in this population is also very low.18
The association between each potential confounder and each of the three outcomes was first examined in univariate analyses. For multivariate analyses, women were classified into having no notifiable infections, chlamydia only, gonorrhoea only, chlamydia and gonorrhoea, or another notifiable infection (syphilis or viral hepatitis) and the model included age, socioeconomic status, and all other variables if they met a prespecified level of association (p<0.05) in the univariate analysis. As screening for chlamydia among young women aged less than 25 years was recommended and more commonly practiced from about 2005,19 we conducted sensitivity analyses by restricting analyses on chlamydia to the subset of women birthing from 2005 and aged less than 25 years.
Results
Between 1998 and 2008 there were 354 217 NSW resident women who had a singleton first birth recorded in the Perinatal Data Collection. Among these women, 3658 (1.0%) had at least one chlamydia notification before the birth with 81.3% (n=2973) of diagnoses made before the estimated date of conception. For gonorrhoea, 196 (0.06%) women had at least one notification before the birth with 84.7% (n=166) of diagnoses made before the estimated date of conception. Half (51%) of the women with a gonorrhoea notification also had a prior chlamydia notification. Of all women, 353 661 (99.8%) could be classified according to whether their birth was preterm and 353 258 (99.7%) according to whether the birth was SGA. Of all women, 4.1% had a SPTB and 12.1% had infants who were SGA. There were 2234 (0.6%) recorded stillbirths.
Table 1 shows women's characteristics according to whether they had a preterm birth (planned, spontaneous at 34–<37 weeks, spontaneous at <34 weeks), a SGA baby or a stillbirth. Based on a significance level of p<0.01, compared with women with a term birth, women with a SPTB were on average younger, more likely to be of lower socioeconomic group, Aboriginal and born in Australia, and less likely to be resident in a major city. They were also more likely to be smokers, booked late into antenatal care and have diabetes, but less likely to have hypertensive disease. More women with SPTB had had a prior notification of chlamydia, gonorrhoea or hepatitis C. Women with a planned preterm birth were generally similar to women with term births except they were on average older, and more likely to have a diagnosis of hypertensive disease or diabetes. Compared with other women, those with a SGA baby were younger, more likely to be of lower socioeconomic group, Aboriginal, born outside of Australia, smokers during pregnancy, booked late into antenatal care, have hypertensive disease and have higher diagnosis rates for all five of the notifiable infections. Compared with women having a live birth, women with stillbirths were more likely to be of lower socioeconomic group, Aboriginal, smokers, but less likely to have a diagnosis of hypertension or diabetes. They were more likely to have a prior diagnosis of chlamydia.
Characteristics of primiparous women with singleton births in NSW according to birth outcome, 1999–2008
Figure 1 and web table 1 show the univariate ORs for each outcome according to the demographic and antenatal characteristics and the infections. The relationship with maternal age for each outcome was non-linear, with the risks particularly high for the very young mothers. Older mothers also had poorer outcomes, especially in relation to stillbirth. For socioeconomic status, the relationship was linear, with risk increasing with greater disadvantage. This was most marked for SGA births. Aboriginal women had a higher risk of all outcomes compared with non-Indigenous women, while overseas-born women were much more likely to have a SGA baby than Australian-born women. A large number of the modifiable factors considered, including smoking and late antenatal booking, were also found to be significantly associated (p<0.05) with each of the obstetric outcomes.
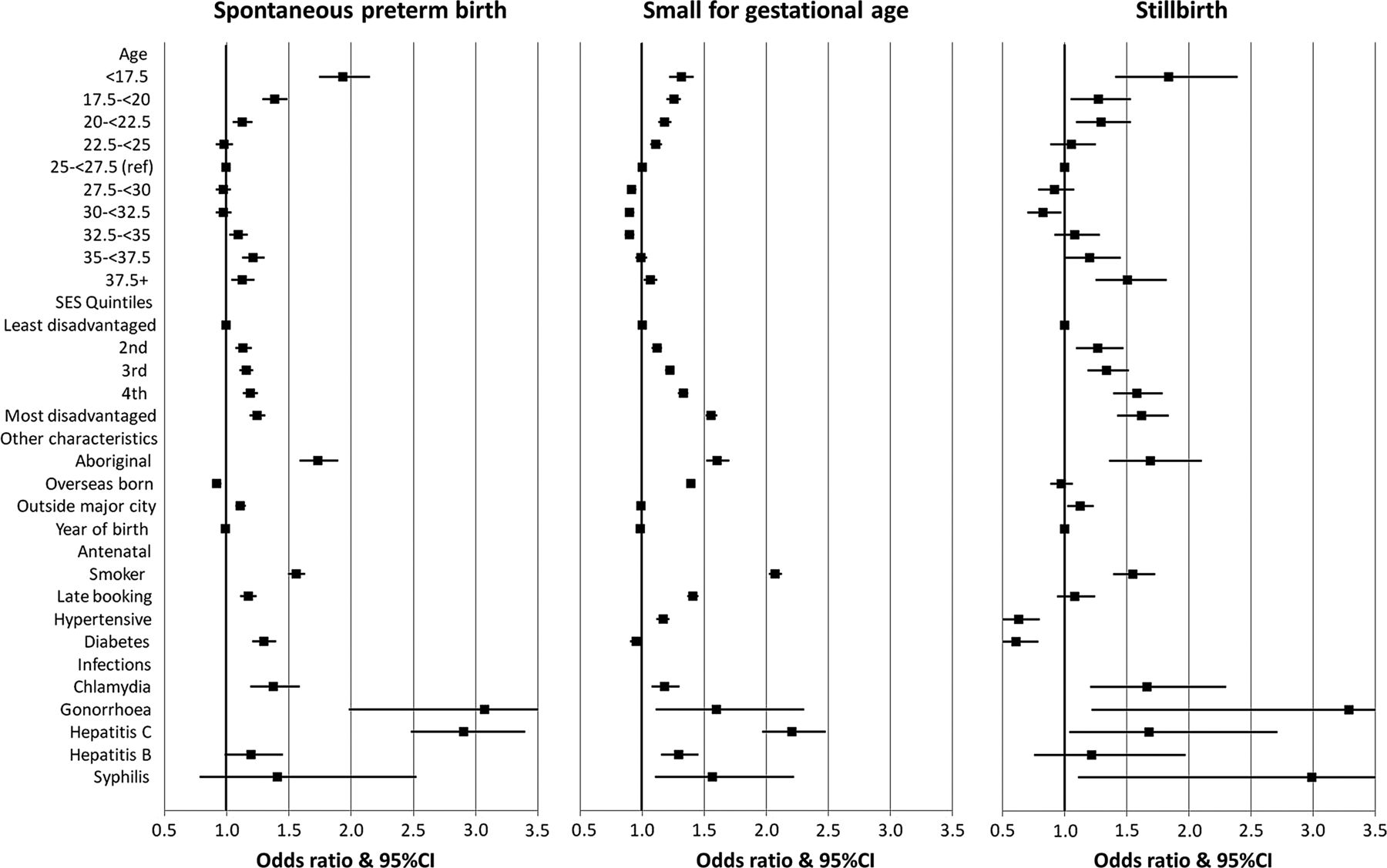
Univariate ORs for association between maternal characteristics and obstetric outcomes.
Table 2 compares the relative likelihood of each adverse obstetric outcome in women with no notifications, chlamydia only, gonorrhoea only or a combination of other notifiable infections. After adjustments, chlamydia was associated with SPTB; adjusted OR (aOR) 1.17 (95% CI 1.01 to 1.37) and stillbirth; aOR 1.40 (1.00 to 1.96). Gonorrhoea was associated with SPTB, aOR 2.50 (1.39 to 4.50) but not stillbirth; aOR 2.35 (0.58 to 9.56) although statistical power was limited due to small numbers. There was no effect of either infection on SGA, aOR 0.99 (0.89 to 1.09) and aOR 0.98 (0.58 to 1.68) for chlamydia and gonorrhoea, respectively. To provide some comparison of the magnitude of risk, the confounder adjusted effect of smoking during pregnancy on SPTB, SGA and stillbirth was aOR 1.35, 2.12 and 1.38, respectively.
Association between infections and adverse obstetric outcomes
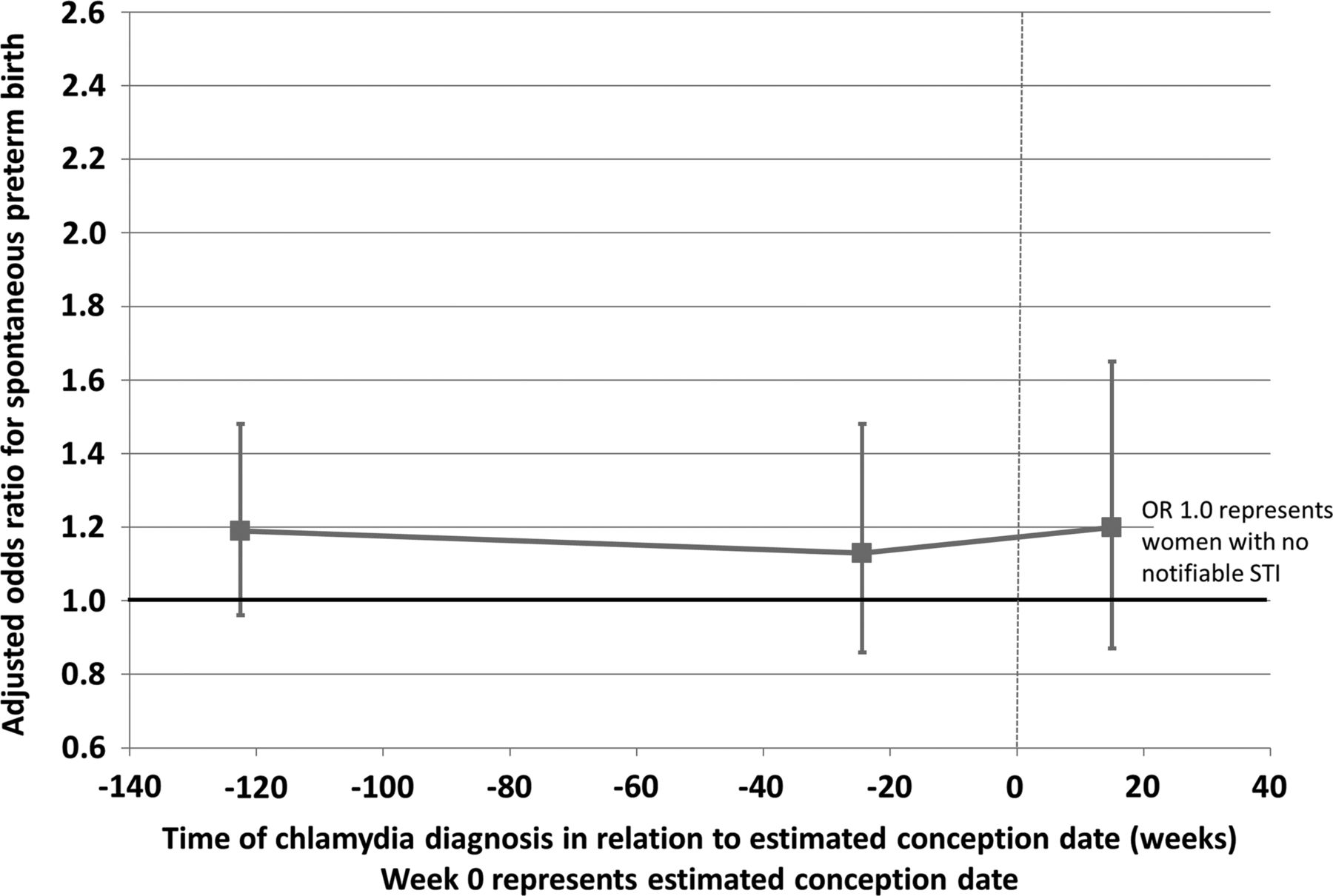
When we examined the timing of the chlamydia notification in relation to the estimated date of conception, compared with women with no notifiable infections (figure 2, web table 2), we did not find any differences in the risk of SPTB. For women with a notification more than 1 year before pregnancy (median 2.4 years), within the year prior to pregnancy (median 0.5 years) and during the pregnancy (median 15 weeks into pregnancy) the aORs were 1.19 (0.96 to 1.48), 1.13 (0.86 to 1.48) and 1.20 (0.87 to 1.65), respectively; p value for heterogeneity 0.9.
{kind=link}
{kind=link}
Risk of spontaneous preterm birth in relation to timing of Chlamydia diagnosis.
When we confined our analyses to women who were more likely to have been tested for chlamydia, that is aged <25 years and giving birth during 2005–2008 (N=38 908), we found 4.6% (N=1784) of women had a prior chlamydia notification (web table 3). Comparing women with no notifiable infections to women having a chlamydia notification only, the risk of SPTB was increased, aOR 1.46 (1.19 to 1.79), but the relationship with SGA and stillbirth was similar to that in the total sample, aOR 0.95 (0.82 to 1.09) and aOR 1.40 (0.87 to 2.25), respectively. The effect of the timing of the chlamydia notification did not differ among this restricted population: for women diagnosed more than 1 year before pregnancy, within the year prior to pregnancy and during the pregnancy aORs for SPTB were 1.61 (1.21 to 2.15), 1.30 (0.91 to 1.87) and 1.40 (0.94 to 2.09), respectively.
Discussion
In this study of first-time mothers having singleton births we found that a prior history of infection with either chlamydia or gonorrhoea was associated with an increased risk of SPTB, a history of chlamydia was associated with stillbirth, but neither infections were associated with a SGA birth. The association of chlamydia with SPTB did not differ according to the timing of the diagnosis in relation to conception.
The strengths of our study include the large whole population sample and the reliability of systematically collected birth records for the outcomes of interest and potential confounders.20 As the notifications of infections are based on laboratory report and required under statute, those identified with a diagnosis would have been likely to have had one. Despite such a large study, as gonorrhoea is not commonly diagnosed in Australian women, we were still relatively underpowered to examine associations with SPTB and stillbirth and this should be considered in interpreting our findings.
Other factors that affect interpretation include the lack of information on individual testing. Throughout the study period antenatal screening for syphilis and hepatitis B was routine19 ,21 and so we can presume that women who did not link to a notification did not have these infections. Annual screening for chlamydia was only recommended for young women aged <25 years after 200519 and data suggests that despite this recommendation, testing in this population is still relatively low at <15%.22 Our study found that 1.0% of women having their first birth had a prior chlamydia notification record but when confined to those aged <25 years giving birth after 2005 this increased to 4.6%. A recent study of over 1000 women aged 16–25 years attending antenatal care in four Australian centres who were all screened for chlamydia found a chlamydia prevalence of 3.2%.23 These data suggest that our estimate of prior diagnosis rates from linked notifications are probably underestimates of true chlamydia prevalence. The results of our sensitivity analysis, restricted to a population of women more likely to be tested for chlamydia, suggest that this underascertainment of chlamydia diagnoses will have underestimated the size of the association with SPTB, aOR 1.46 (1.19 to 1.79) versus 1.17 (1.01 to 1.26) in the entire population. Gonorrhoea is much less frequently diagnosed in Australia24 and unlike chlamydia, for women, there is no evidence to suggest testing would have changed substantially over time.25 However Aboriginal women are known to have a higher prevalence of gonorrhoea than non-Aboriginal women24 and may be more likely to be tested. They are also known to have a higher risk of adverse obstetric outcomes.26 While this potentially confounds our results, we were able to adjust for Aboriginality in our analyses and did not find this substantially attenuated the estimates of association between gonorrhoea and SPTB. We could adjust for a large number of potential confounders that other studies have not been able to account for including late antenatal booking and smoking, however we did not have information on other non-notifiable infections such as bacterial vaginosis and trichomonas vaginalis that have been reported to be associated with SPTB6 and also associated with chlamydia and gonorrhoea infection.27 Therefore there is the potential for unmeasured confounding to affect our estimates of association.
An important distinction in our study compared with previous work is that over 80% of the chlamydia and gonorrhoea infections were diagnosed before conception, and therefore our results are not directly comparable with other studies. Despite this, a systematic review that included 12 studies of chlamydia infection diagnosed during pregnancy and reproductive health outcomes, suggested chlamydia infection was associated with an increased risk of preterm labour (relative risk (RR)=1.35 (1.11, 1.63)), low birth weight (RR=1.52 (1.24, 1.87)) and perinatal mortality (RR=1.84 (1.15, 2.94)).3 Our estimates of the association of chlamydia infection and SPTB and stillbirth are consistent with the results of this review. Studies examining low birth weight as an outcome do not take into account gestational age, and so may have inadvertently been considering the outcome of preterm birth. This may explain the difference between our findings for SGA and the results of the systematic review, which considered low birth weight. Fewer studies have examined gonorrhoea and adverse obstetric outcomes although a recent case-control analysis that was able to account for many factors including bacterial vaginosis, trichomonas, syphilis and chlamydia reported an increased risk of preterm birth associated with gonorrhoea diagnosed in the antenatal period; aOR: 2.01(1.02 to 3.97).4 The consistency of our findings with these other studies that examined chlamydia and gonorrhoea diagnosed in pregnancy also supports our observation that the risks of adverse obstetric outcomes appear similar regardless of whether the diagnosis of chlamydia or gonorrhoea infection is made prior to or during the pregnancy.
Given the limitations of our data it is difficult to speculate on whether the associations observed are causative or if chlamydia and gonorrhoea are simply markers of a higher-risk obstetric population and that unmeasured causal factors may have explained the associations that we and others have found. There is certainly some evidence to suggest that the mechanisms that trigger SPTB and stillbirths are related to chronic inflammation6 ,28 and it is well known that chlamydia and gonorrhoea infection can lead to chronic inflammation of the upper genital tract. However evidence against a causative role is that trials of prophylactic antibiotics that would treat chlamydia infection given during, or even prior to the pregnancy, have not been able to demonstrate efficacy in the prevention of SPTB.8 ,29
Currently there are no trials of screening for chlamydia or gonorrhoea in antenatal women examining if such an intervention may improve obstetric outcomes. However as our results suggest the association with poor obstetric outcomes exists even before the pregnancy starts; it would add to our understanding of the true role of these infections if trials of screening for chlamydia, that aim to reduce prevalence in the general population, included longer-term outcomes, such as the incidence of adverse obstetric events. SPTB and stillbirth have major consequences for the mother and the child and our study demonstrates that the number of births affected in a high-income country such as Australia is still substantial, with 4.1% of first-time mothers having a SPTB and 0.6% a stillbirth. Preventative strategies in the preconception period may be an important area for further research.
Key messages
-
A diagnosis of a chlamydia or gonorrhoea infection prior to pregnancy was associated with spontaneous preterm birth and a diagnosis of chlamydia was associated with stillbirth.
-
The risk of spontaneous preterm birth did not differ between women diagnosed with chlamydia before pregnancy or during pregnancy.
-
Our results suggest that sexually transmissible infections in pregnancy and the preconception period may be important in predicting adverse obstetric outcomes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors BL instigated the study, conducted the analyses and wrote the initial draft. BL, CLR and LJ obtained the data for the study. All authors advised on the analyses, interpretation of results and edited drafts of the paper.
-
Funding The NSW Centre for Health Record Linkage conducted the linkage of the datasets. The NSW Ministry of Health provided deidentified data to the researchers. The study was funded by the National Health and Medical Research Council (NHMRC) grant #1020628. The funder had no input into the study design, analysis, interpretation, writing or decision to submit for publication. BL and CLR are supported by NHMRC fellowships.
-
Competing interests None.
-
Ethics approval NSW Population and Health Services Research Ethics Committee; University of New South Wales Human Research Ethics Committee; Aboriginal Health and Medical Research Council Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Linked data from this study are available through an ethics application to the NSW Population and Health Services Research Ethics Committee and approval by the NSW Ministry of Health.