Article Text

Abstract
Objectives Partner notification is crucial for sexually transmitted infection (STI) control. We developed Suggestatest.nl (SAT), an internet-based notification system for verified diagnoses of STI/HIV.
Methods SAT uses email, short message service, postal letter or a gay dating site to notify sexual contacts. SAT was piloted at the Public Health STI clinics in two major cities in the Netherlands. We evaluated SAT from March to July 2012 by analysing SAT notifications linked with epidemiological data. Determinants for SAT use were assessed using multivariable logistic regression analysis.
Results Of 988 index clients receiving a SAT code, overall 139 (14%) notified through SAT, sending 505 notifications (median 2), 84% by text messaging and 15% by email; 88% non-anonymously. Of those intending to use SAT, 23% notified with SAT. Intention to use SAT was the only independent determinant of SAT use in heterosexuals and men who have sex with men. Among the 67 SAT users in Rotterdam, 56% (225/402) of their partners at risk were contactable, and 95% (213/225) of those were notified using SAT. 58% of SAT-notified partners accessed the SAT-website and 20% of them subsequently consulted the STI clinics. STI positivity in partners was lower in those notified by SAT (28% (32/116)) than in those with contact cards (45% (68/152); p<0.001).
Conclusions Although the challenges posed by non-contactable partners are not solved by SAT, it is a valuable novel tool for notification of verified STI diagnoses by index patients and providers. In addition to current standard partner notification practice it suits a small number of clients, especially those reporting more than one partner.
- Partner Notification
- Public Health
- Health Serv Research
Statistics from Altmetric.com
Introduction
A cornerstone in the control of sexually transmitted infections (STIs) is notification, testing and treatment of (asymptomatic) sexual partners of patients diagnosed with treatable STIs, referred to as partner notification (PN).1 ,2 Testing of notified partners generally yields a higher rate of STIs compared with individuals unselectively screened for STIs.3 Furthermore, treatment of infected partners reduces the likelihood of index patients being reinfected, complications from untreated infections, and, most likely, further transmission.4 Many index patients find it difficult to notify their partners.5 PN can be assisted by contact cards mentioning the verified STI and advice. The index patient hands out these cards to partners personally.
In the past few years, internet-based PN services, such as InSPOT, Let Them Know and The Drama Down Under, have been developed in the USA and Australia, which allow individuals to send either named or anonymous e-cards, emails or short message service (SMS) messages to their partners.6–9 This way of informing partners is seen as less confronting, more convenient, and less time-consuming than informing partners face-to-face or by phone.9 ,10 Although website user statistics (with high absolute numbers) suggest frequent visits to these services,6–9 evaluations of these publicly accessible websites show limited use and effectiveness.11–13 These internet services are not based on verified diagnoses and not developed for use by providers.
We developed ‘suggestatest.nl’ (SAT), an internet-based notification system for verified diagnoses of STI/HIV, to support the individual (index patient) and nurses in the process of PN. SAT was piloted at the Public Health STI clinics in Amsterdam and Rotterdam, the Netherlands. In this paper we aim to evaluate SAT use and partner response during the pilot, by linking SAT data to clinical data. Acceptability of SAT in index patients and notified partners will be reported in a separate paper.
Methods
Suggest-a-test
After counselling the index patient in the STI clinic, the nurse logs in into the SAT website and enters the specific STI, sex and sexual preference details of the index patient; SAT then creates a personal login code for the index patient with these data encrypted. The nurse enters this code and the patient's PN preference (SAT or non-SAT) manually in the electronic patient system (EPS). The index patient receives the index code automatically in print (Amsterdam) or by SMS (Rotterdam). Even when patients prefer to notify partners in person, they are supposed to receive a SAT code to enable them to use SAT in case they reconsidered. SAT also allows provider referral, where the nurse can login into SAT with the index code and inform partners anonymously with data received from the index patient.
Index patients can login at http://www.suggestatest.nl with their code at any convenient time. For each sexual partner they can choose to send a notification via email, SMS, a postal letter, or a personal message on a gay dating site (gay.nl). STI notifications are standardised texts, which can be sent anonymously (default) or non-anonymously. The SAT code can only be used for 10 logins whereafter it is blocked. Partners then receive a notification from the STI clinic via SMS, email, postal letter or to their inbox at http://www.gay.nl. This message consists of a personal partner code and a short text saying that they have had sex with somebody who has recently been diagnosed with a STI and advising them to read their online notification and to get tested.
With this partner code, partners can login into SAT to find out more about the notified STI, possible treatment and how to make an appointment at the STI clinic. They are asked to print this personal notification and bring it to the STI clinic or their general practitioner (GP) for testing and treatment. The verified-diagnosis notification through SAT is comparable with the existing method of contact tracing cards: if indicated, treatment will be started immediately.
In SAT, patient information is dealt with the highest confidentiality. The SAT codes provided to the index patients and the notified partners are unique, randomly created letter and number combinations. A secure server is used and data are encrypted. After sending a notification to partners, all personal data of notified partners are automatically removed leaving an anonymous database. To assure confidentiality, no connection between notified partners and the index patient is possible. To stress authenticity, we made a clear link at suggestatest.nl to the STI clinic websites, as well as to the STI Aids helpline in the Netherlands.
This study was waived by the Medical Ethical Committee of the Erasmus University of Rotterdam, because SAT is an extension of standard care.
Data analysis
The evaluation period for this pilot was from 1 March to 30 June 2012 in Amsterdam and from 23 April to 20 July 2012 in Rotterdam. Study size was determined by resources and feasibility. PN data from the Amsterdam and Rotterdam EPS were linked to data from the SAT database by the SAT code given to the index patient. Due to initial problems of registering the SAT code in the EPS, a few codes could not be linked to EPS data.
From the SAT database we assessed number of codes created, used for login, and used to send notifications; method and anonymity of notifications; and number of notifications by sex, sexual preference, STI and by clinic. We calculated the percentage of partners logging in by all partners notified by SAT. Lead time between creating the index code and login of the index patient and between sending a notification and login of the partner was calculated.
From the linked SAT and routinely collected EPS data, we assessed the percentage of index patients not receiving a code and the reason for this. The percentage of patients with STI using SAT to notify partners, as well as those intending to use SAT, was calculated using all patients with STI as denominators. Percentages were compared using the χ2 test, considering p < 0.05 as statistically significant.
Determinants for using SAT such as age, sex, sexual preference, ethnicity, STI and number of sex partners in the previous 6 months were assessed. We categorised the STI/coinfections into STI groups: Chlamydia including lymphogranuloma venereum (CT); gonorrhoea (Go); CT/Go coinfections; new HIV infections including coinfections like CT, Go or syphilis; and syphilis including coinfections except HIV. We performed univariable and backward multivariable logistic regression analysis to asses determinants of SAT use. Analyses were performed using SPSS V.19 (SPSS, Chicago, Illinois, USA).
It was not possible to compare effectiveness of PN (ie, number of notified partners per index patient) during the pilot with the months preceding the pilot, as prepilot registration of PN was found to be poor. Therefore, we used three proxy measures to evaluate SAT.
Results
SAT codes provided and SAT use by index cases and notified partners
During the intervention period, 1717 patients were diagnosed with STI in the Amsterdam clinic, versus 578 in the Rotterdam clinic. In Amsterdam, 61% of patients with STI did not receive a SAT code, mostly because they preferred another PN method (57%) or because PN was not necessary or already done (27%). In Rotterdam, 44% of patients with STI did not receive a SAT code, mainly because PN was already done (52%) or for unknown reasons (34%).
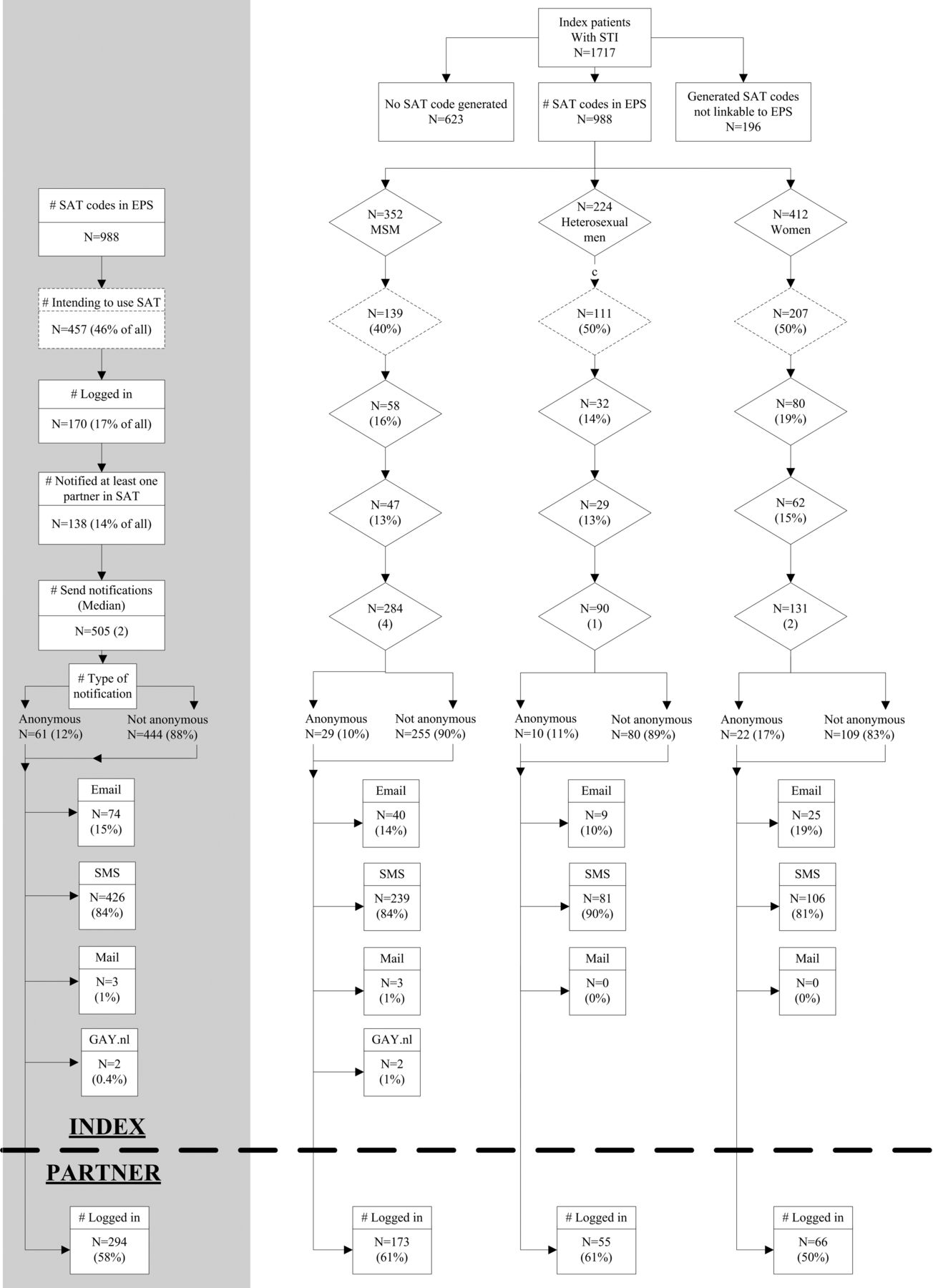
During the evaluation period, 1184 SAT codes were provided to index patients; 988 of these could be linked to medical records in the EPS (figure 1).

Use of suggest a test (SAT) of index patients and notified partners, overall and by sex and sexual orientation. EPS, electronic patient system; MSM, men who have sex with men.
Of these 988 index patients, 17% logged in into SAT, although 14% actually used SAT to notify partners. SAT use was higher in Rotterdam than in Amsterdam (21% vs 11%, p < 0.001, results not shown). Of the 457 index patients who expressed the intention to use SAT, 23% actually used SAT, compared with 6% not intending to use SAT.
The percentage using SAT did not differ between men who have sex with men (MSM), heterosexual men and women (p=0.7). The median number of notified partners per index patient was 2 (IQR 1–4). This was 4 for MSM (IQR 1–7; maximum 40), 1 for heterosexual men (IQR 1–3; maximum 21) and 2 for women (IQR 1–3; maximum 7). Provider notification was done in 17% (8/47) of MSM, in 11% (7/62) of women and none in heterosexual men.
Most notifications were done non-anonymously (88%, figure 1). The percentage anonymous notifications did not differ between MSM, heterosexual men and women (p=0.15). Of the index patients using SAT, 26% (36/138) sent at least one notification anonymously. SMS was the most used method (84%), followed by email (15%); three letters were sent (1%) and http://www.gay.nl was only used twice. Of the 505 notified partners, 294 (58%) logged in into SAT to read their STI notification. This percentage did not differ for anonymous versus non-anonymous notifications (p=0.3), nor for notifications sent by MSM, heterosexual men or women (p=0.11). Ninety per cent of index patients notified within 1 week, and 98% within 2 weeks; for the log in time of notified partners this was 84% and 95%, respectively.
SAT use was 13% in CT cases, 15% in gonorrhoea cases, 13% in CT/Go cases, 26% in syphilis cases and 20% in HIV cases (p=0.14). For HIV, SAT use was 10% (2/21) in Amsterdam versus 44% (4/9) in Rotterdam. In Rotterdam, all HIV notifications were sent by the nurses (provider notification). Nurses reported that some patients with coinfections were willing to notify via SAT for the STI but not for HIV.
Univariable analysis of SAT use for heterosexual men and women in both cities showed that the number of sex partners in the past 6 months (1, 2, 3–4, 5+) was correlated with SAT use, with patients reporting only one partner using SAT less often (8%) than those with 2 (15%; OR 2.2 (95% CI 1.0 to 4.7)), 3–4 (19%; OR 2.9 (95% CI 1.4 to 6.1)) and 5+ partners (14%; OR 2.1 (95% CI 0.9 to 4.8)). Although not significant, native Dutch patients used SAT slightly more often (18%) than patients of non-Dutch origin (12%; OR 0.7 (95% CI 0.4 to 1.0)). Patients from the STI clinic of Rotterdam used SAT more often (20.5%; OR 2.2 (95% CI 1.4 to 3.4)) than those from Amsterdam (10.6%). Patients who preferred to use SAT notified more often using SAT (21.4%; OR 3.4 (95% CI 2.0 to 5.6)) than patients who did not prefer or from whom preference was unknown (7.4%). Age, sex and STI category were not correlated with SAT use. In multivariable analysis, only preference for SAT use remained significant in the final model (OR 3.4 (95% CI 2.0 to 5.6)).
For MSM, only STI category was significantly associated with SAT use; MSM diagnosed with syphilis used SAT more often than MSM having CT (27% vs 9%, respectively, OR: 3.9 (95% CI 1.5 to 9.9)). MSM from the STI clinic of Rotterdam used SAT more often (23.3%; OR 2.5 (95% CI 1.3 to 4.8)) than those from Amsterdam (10.9%). MSM who preferred to use SAT notified more often using SAT (27.5%; OR 8.7 (95% CI 4.0 to 18.7)) than MSM who did not prefer or from whom preference was unknown (4.2%). Age, number of sex partners in the past 6 months and ethnicity were not correlated with SAT use. In multivariable analysis, only preference for SAT use remained significant in the final model (OR 8.7 (95% CI 4.0 to 18.6)).
SAT evaluation
The percentage of all reported, eligible (at risk) and contactable partners notified through SAT by clinic
SAT users notified 51–56% of their partners in the previous 6 months in SAT (see table 1). As the number of partners eligible for PN may be lower than the total partners in the last 6 months, a different picture arises taking this into account. Of the 67 index patients who used SAT in Rotterdam, 96% of their partners were eligible, but only 56% (225/402) of these were reported to be contactable. This percentage was 36% for MSM, 70% for heterosexual men and 99% for women. Comparing these percentages to those of patients not using their SAT code, patients who used SAT overall have a lower proportion of partners that are contactable (56% vs 65%, p<0.001). In contrast to MSM and heterosexual men, women who used SAT reported 99% of their eligible partners to be contactable versus 51% for women who did not use SAT. When looking in more detail into the EPS files of the women who did not use SAT, we found that six of them were sex workers with around 100 sex partners per 6 months, of whom the vast majority was not contactable. The remaining 110 women (who did not use SAT) reported that 95% of their eligible partners are contactable.
Percentage of all reported, eligible (at risk) and contactable partners notified by clinic and by using SAT
Of the contactable partners, 95% were actually notified through SAT; this percentage was lowest for women (79%) and highest for MSM (111%). This means that MSM notified more partners than that they reported to be contactable during consultation at the clinic. Looking in detail into this we found that 29% of individual MSM notified more partners than identified at first, versus 25% of heterosexual men and 21% of women (data not shown). Compared with users of the SAT code, index patients not using the SAT code had less partners at risk (73% (1229/1693) versus 96% (402/419); p<0.001) and a slightly higher percentage of partners at risk was contactable (65% (802/1229) versus 56% (225/402); p<0.001). In total, of the 1027 contactable partners that were reported by index patients with STI who received a SAT code in Rotterdam, 213 (21%) were notified through SAT. However, we do not know whether the other contactable partners were not notified at all or notified using a different method.
Partners notified in SAT and tested in the two clinics
Of the total number of SAT-notified partners, 56% read their notification, and 20% of all visited one of the two STI clinics with a SAT notification. This was similar for the various STIs (p=0.5) (see figure 2).

{kind=link}
{kind=link}
Number of all partners who were notified by suggest a test (SAT), who read their online notification, and who visited the STI clinics of Amsterdam and Rotterdam, by STI. CT, Chlamydia; Go, gonorrhoea; LGV, lymphogranuloma venereum.
STI positivity in all notified partners by STI category, clinic and notification method
Of all notified persons visiting the STI clinics, 5% (59/1255) were notified via SAT in Amsterdam versus 17% (57/342) in Rotterdam, whereas 11% (143/1255) were notified by contact card in Amsterdam versus 3% (9/342) in Rotterdam. Of all notified persons presenting, 143 (11%) had been notified by contact card, 59 (5%) via SAT and 1053 (84%) through other ways without a verified diagnosis of the index patient; see table 2. In notified partners who visited the clinics during the intervention period, the percentage positive for the STI they were notified for was calculated. Overall STI positivity was lower in those notified by SAT (28%, n=116) than in those with contact cards (45%, n=152; p<0.001).
STI test outcomes by STI specific notification method among notified persons presenting to STI clinics
Discussion
This is the first study to demonstrate substantial use of online PN by index patients, particularly by those with intention to use it. Almost one in four of the heterosexual and MSM index patients who preferred to use SAT actually notified partners in SAT. Innovative in our service is the provider-led creation of a code which limits misuse by sending verified STI-specific information to partners.12
Strengths and limitations
To our knowledge this is the first study with clinic-based follow-up of use of internet-based PN that evaluates use, by index patients and by notified partners, in combination with epidemiological data. Moreover, we could monitor notified partners presenting at the clinic and their test outcome.
A main limitation of our project is that this was not a research project but a pilot implementation in daily practice with all the associated constraints. We would preferably have compared PN outcomes during the pilot with the period before. However, poor registration impaired this and proxy measures were used instead for evaluation.
Interpretation and comparison with international studies
The provided SAT codes were used by 14% of index patients. This may seem modest when compared with the high absolute numbers of people who used some other internet-based PN programmes. However, evaluation of inSPOTLA (internet PN Los Angeles) found very limited evidence of programme effectiveness among MSM in Los Angeles County.13 Awareness of that open internet site was around 15% among MSM and reported use of the site was less than 2%. Another study also shows low recognition and use of inSPOT by heterosexual STI clinic attendants (6% and 2%, respectively).12 In 3 years, only two visitors of a high-volume sexual health clinic stated having received an inSPOTLA e-card as reason for their visit13 compared with 7% (116/1597) of all notified partners presenting at our clinics. Thus, SAT use is not that low. In a substantial number of index patients, provider referral was done through SAT, which alludes to the additional value of the system for STI health professionals.
The plan was that nurses would create a SAT code for all patients with STI, but this was clearly not done in either clinic. Some nurses found that SAT interrupted their motivational counselling process too much. Strikingly, issuing and use of SAT codes was higher in the Rotterdam clinic than in the Amsterdam clinic. This may be related to the more frequent provision of contact cards to patients with STI in Amsterdam compared with Rotterdam. As providing a SAT code was slightly more manual work in Rotterdam, this cannot explain higher use.
SAT was designed to enable anonymous PN by the index patient, but to our surprise 85% of the notifications were sent non-anonymously. This is valuable for clinical practice, as notified partners can provide specific information about time of sexual contact during the consultation at the clinic.
SMS was used most widely (82%), followed by email (16%). The option of using chat addresses in the dating site was only used twice. Users of these sites may want to use the site exclusively for dating and not STI-related issues. Also they may have mobile numbers of their dates and notify by SMS. Further research is needed before we can decide whether or not to add other dating sites.
It is unknown for whom internet PN may be most beneficial.14 We found that heterosexuals with multiple recent partners were more likely to use SAT, suggesting that SAT is used more for notification of ex and non-regular partners than for current partners. The intention to use SAT was the only independent factor for SAT use in heterosexuals and MSM.
We noticed that patients were reluctant to use SAT for HIV notifications. Most of the HIV notifications in SAT were provider referral, which demonstrates the advantage of the system for this purpose. On the other hand, there is also a danger in providers preferring to use SAT over phoning partners to notify for HIV, knowing that many notified partners do not read their online notification. It is still preferable to do provider notification personally, and use SAT additionally. We agree with others that an online PN system is a supplemental tool to existing PN services15 and cannot replace counselling.
The major challenge in PN remains the high number of non-contactable partners in MSM due to anonymity. We do not know whether we have reached more anonymous partners than without SAT. However, 29% of MSM notified more partners in SAT than they identified first-hand in the clinic and some of these partners may not have been notified if SAT had not existed. Only 20% of the SAT-notified partners were tested at our two clinics, but partners may have been screened at their GP instead.
As with contact cards, SAT-notified partners receive a notification with a verified diagnosis, which may motivate STI testing and enable timely partner treatment. The lower positivity in SAT notifications compared with contact cards may be due to use of SAT in ex-partners and contact cards in current partners, who may still be infected.
To measure effectiveness of SAT, a randomised controlled trial comparing SAT with other PN methods with biological outcomes (partner testing and treatment) would be necessary. In practice this would be very challenging. In a project aiming at better registration of PN and training of nurses, we have shown that registration by itself improved PN and case finding in partners; of all detected new HIV cases among MSM in the Netherlands, 19% were detected through PN in 2010 versus 35% in 2012.16
Strikingly the majority of notified patients still arrive without a verifiable notification, leaving room for improvement in STI clinics (providing all index patients with either a contact card or a SAT code) as well as in GP practices. At this moment we are piloting SAT and other tools to improve PN in GP practices.
Conclusion
Although the challenges posed by non-contactable partners are not solved by SAT, it is a valuable novel tool for notification of verified STI diagnoses by index patients and providers. In addition to current standard PN practice it suits a small number of clients, especially those reporting more than one partner.
Key messages
-
In suggest-a-test (SAT), 82% of notifications with verified diagnosis were sent by text messaging, 16% by email; 86% non-anonymously.
-
Of 998 index patients with a verified STI diagnosis, overall 14% notified through SAT, and of those intending to use SAT 23%.
-
Fifty-eight per cent of SAT-notified partners checked their notification. STI positivity in SAT-notified clients was 28%.
-
SAT is a valuable tool for notification of verified STI diagnoses by index patients and providers; it suits especially those reporting more than one partner.
References
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors HMG, PV, HACMV designed the intervention and study protocol, supported by MSvR, EOdC, TH, RK. MH and FvdH were responsible for implementation and data collection at the STI clinics. HMG, MSvR did the analyses, HMG, MSvR and HACMV drafted the paper, all authors have commented on draft versions and approved the final version.
-
Funding This study was supported by the Dutch AIDS foundation (Grant number: 2009085) and the Research and Development Fund of the Public Health Service of Amsterdam.
-
Competing interests None.
-
Ethics approval This study was waived by the Medical Ethical Committee of the Erasmus University of Rotterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.