Article Text

Abstract
Objectives We sought to assess the prevalence and correlates of seroadaptive behaviours (ie, sexual history incorporating some unprotected anal intercourse (UAI)) and conventional risk reduction behaviours (ie, consistent condom use or no anal intercourse) among men who have sex with men (MSM) in San Francisco in 2011. We compared the prevalence of seroadaptive behaviours between serial cross-sectional surveys from 2004, 2008 and 2011.
Methods We analysed data from the 2011 wave of the National HIV Behavioral Surveillance system in San Francisco. We categorised men's self-reported sexual behaviour history in the past 6 months into a schema of seroadaptive behaviours and conventional risk reduction behaviours. We compared the prevalence of behaviour categories by self-reported HIV serostatus, HIV testing history, awareness of pre-exposure HIV prophylaxis (PrEP) and diagnosis of a sexually transmitted infection (STI).
Results Seroadaptive behaviours remained common in San Francisco MSM, with a 2011 prevalence of 46.6%, up from 35.9% in 2004. Consistent condom use or no anal intercourse was more common than seroadaptive behaviours in HIV-negative MSM, men who had not heard of PrEP and men without an STI diagnosis. Seroadaptive behaviours increased from 2004 to 2011.
Conclusions HIV seroadaptive behaviours remain common in San Francisco MSM, have increased in the last decade and are practiced differently by MSM with different sexual health knowledge and outcomes. Public health researchers and officials should continue to document the prevalence, intentionality, efficacy and safety of seroadaptive behaviours among diverse communities of MSM.
- HIV
- HOMOSEXUALITY
- SEXUAL BEHAVIOUR
- CONDOMS
- GAY MEN
Statistics from Altmetric.com
Introduction
From the beginning of the epidemic to the present day, a large majority (>90%) of San Francisco's HIV-affected population has been men who have sex with men (MSM).1 Recent work has characterised the trajectory of the HIV epidemic in this population, describing the most recent phase (2004–the present) as a period of increased testing and antiretroviral therapy (ART) access, with correspondingly decreased HIV incidence.2 This contrasts with earlier predictions that HIV incidence would persist at high levels in San Francisco MSM due to stabilised or increased risky sexual behaviours.3
Another factor that characterises the most recent phase of San Francisco's HIV epidemic is the widespread adoption of seroadaptive behaviours. Broadly, seroadaptive behaviours are a diverse set of community-originated strategies for reducing risk of HIV transmission/acquisition by choosing partners or sex acts based on knowledge of self and partner's HIV serostatus.4 ,5 These strategies differ from established public health messages delivered to MSM in that they incorporate unprotected anal intercourse (UAI) in some circumstances, when recent serostatus is known (as of last HIV test), and risk is thought to be low. Seroadaptive behaviours received attention from researchers and public health officials early last decade.6–8 Research demonstrated that seroadaptive behaviours were widespread among MSM in the developed world9 ,10; in San Francisco, seroadaptive behaviours in aggregate were found to be more common than consistent condom use.5 ,11 Along with broad ART access, seroadaptive behaviours in San Francisco MSM have been posited as an explanation for decreased HIV incidence in the absence of decreased risk behaviour.2 ,12
Little is known about seroadaptive behaviours in the present phase of San Francisco's HIV epidemic beyond 2008, a period marked by proof of antiretroviral therapy as prevention (including pre-exposure HIV prophylaxis (PrEP)),13 ,14 high-frequency HIV testing among MSM15 and the treatment of all HIV infection regardless of disease stage.16 There is also little known about which behavioural and health-related factors may be correlated with seroadaptive behaviours.17 ,18 Richer detail on the predictors and current practice of seroadaptive behaviours will aid in the continuing effort to establish the prevalence of seroadaptive practices, their intentionality19 ,20 and their efficacy in preventing HIV.21 Therefore, we analysed the 2011 round of San Francisco's National HIV Behavioral Surveillance (NHBS) data for MSM. We characterised the prevalence of seroadaptive behaviours by health-related correlates including self-reported HIV serostatus, testing behaviour, awareness of PrEP and diagnosis of a sexually transmitted infection (STI). We calculated the proportion of men practicing any seroadaptive behaviour (ie, strategic UAI) versus those practicing no UAI (ie, conventional risk reduction), and charted these proportions across the three rounds of San Francisco's MSM-NHBS data, from 2004, 2008 and 2011.
Methods
Sampling and recruitment
We analysed data from three waves of National HIV Behavioural Surveillance among MSM in San Francisco: 2004 (N=525), 2008 (N=552) and 2011 (N=510). Details of the NHBS system have been published elsewhere.22 All three waves sampled MSM using time-location sampling (TLS).23 TLS samples hard-to-reach populations in venues where they are known to congregate, providing a quasi-probabilistic cross-sectional sample. Briefly, in the formative phase we identified the universe of venues where MSM congregate (87 venues, including gay-identified venues such as bars and clubs and non-gay-identified venues such as parks, cafes and gyms). Venues were randomly sampled between July and December 2011, and study staff intercepted and recruited men from selected venues. Eligibility requirements were age 18 years or older, male at birth, residence in one of the 10 Bay Area counties, attendance at a randomly selected venue, ability to complete the interview in English or Spanish and having ever had oral or anal sex with a man. Men provided verbal consent and completed an anonymous survey administered by study staff in the venue. Further recruitment details of the San Francisco NHBS are available elsewhere.5 This surveillance activity received ethical review and clearance from the Centers for Disease Control and Prevention, the University of California, San Francisco's Committee on Human Research and the Institutional Review Board of Oregon Health & Science University.
Seroadaptive behaviours
NHBS participants were asked to report on up to five sexual partnerships in the past 6 months. Participants were asked to enumerate each partner's HIV serostatus (negative, positive or unknown) and the number of episodes of insertive and receptive anal intercourse, protected and unprotected. Based on their self-reported HIV serostatus and self-reported sexual behaviour, we categorised men in the sample into the mutually exclusive, hierarchical schema of seroadaptive behaviour patterns and risk reduction behaviour patterns that we have described previously.5 ,17 We emphasise that the accuracy of this categorisation depends on the participant's testing history, honest self-report, and in the case of partners’ serostatus, the participant's and the partner's honesty and accuracy in reporting. Our analysis thus reflects the uncertainly inherent in serosorting.
In order of ascending risk, men were categorised as having had no sex, no anal sex or having used condoms consistently (ie, 100% of the time for anal sex). We refer to this group of behaviour categories in aggregate as ‘conventional risk reduction preventive strategies’ because they conform to conventional public health messages to MSM to avoid UAI, whereas seroadaptive strategies by definition include some UAI. Again in order of ascending risk, men who reported some UAI but whose partners were all of the same reported serostatus were categorised as engaging in ‘pure serosorting’. ‘Condom serosorting’ was defined as engaging in some UAI and some serodiscordant anal sex, but only UAI with seroconcordant partners. ‘Seropositioning’ was defined as having some serodiscordant (or unknown seroconcordance) UAI, but in the position that minimises risk of HIV transmission (ie, insertive for HIV-negative MSM and receptive for HIV-positive men).24 These three categories were collectively considered seroadaptive behaviours. The final category was made up of men who engaged in sexual behaviour with highest risk for HIV transmission: unprotected receptive anal intercourse with an unknown or serodiscordant partner for HIV-negative men, and unprotected insertive anal intercourse with an unknown or serodiscordant partner for HIV-positive men.
Behavioural and health-related covariates
We analysed several health-related and behavioural measures to assess their associations with seroadaptive behaviours versus conventional risk reduction behaviours. Participants’ self-reported result of their last HIV test was used to categorise men as HIV-positive or HIV-negative, by the logic that self-perception of one's own serostatus guides seroadaptive behaviours. Men who did not know their last result or who refused to answer were excluded from analysis.
Testing frequently and disclosing results to partners is a cornerstone of seroadaptive behaviours for HIV-negative men; therefore, we analysed apparent seroadaptive behaviours in conjunction with testing recentness. The CDC recommends that sexually active MSM test every 6 months.25 Therefore, for HIV-negative men, we categorised this variable as ‘tested within the last 6 months’ and ‘last test more than 6 months ago’, and compared prevalence of behavioural patterns in both groups.
As PrEP has received increasing scientific and media attention, public health officials have speculated on the extent to which this may alter the sexual decision making and risk behaviour of MSM.26 ,27 Because knowledge of PrEP is a prerequisite for PrEP-related changes in risk behaviour, we analysed seroadaptive behaviours among HIV-negative men according to their knowledge of PrEP, measured by asking participants: “Before today, have you ever heard of people who do not have HIV taking anti-HIV medicines, to keep from getting HIV?”
Among the chief critiques of the safety of seroadaptive behaviours is the possible transmission of STIs.28 We analysed whether participants reported testing positive for bacterial STIs (gonorrhoea, chlamydia or syphilis) in the past 6 months and whether they reported ever testing positive for viral STIs (genital herpes and genital warts). We compared seroadaptive behaviours and conventional risk reduction behaviours among men testing positive for any STI and those who reported no STIs.
Statistical analysis
We compared the proportion of men in each sexual behaviour category, overall and stratified by the behavioural and health-related variables: self-reported HIV status, tested in the past 6 months, awareness of PrEP and STI diagnosis. Significance was assessed using the χ2 test and Fisher's exact test where appropriate. We used the Cochran–Armitage test for trend29 to assess the temporal trends in prevalence of aggregate seroadaptive behaviours versus conventional risk reduction behaviours across the three waves of data collection, separately for HIV-negative and HIV-positive men.
Results
Of the 479 MSM recruited for the 2011 wave of NHBS, 24 men had unknown or missing HIV serostatus, leaving an analytical sample of 455 men in this study. Among this target population of men with known serostatus, 357 were HIV-negative (78.5%). Just over half (50.7%) of HIV-negative men reported no UAI in the past 6 months (table 1). These men reported behaviours that fit into the conventional (ie, non-seroadaptive) risk reduction category, comprising no sex (16.0%), no anal sex (2.8%) and consistent condom use (31.9%). The proportion of HIV-positive men in the conventional risk reduction category was significantly smaller at 37.8% (p<0.001) (16.3% no sex, 5.1% no anal sex, 16.3% consistent condom use). Among HIV-negative men, the predominant individual strategies (those with prevalence >30%) were consistent condom use (31.9%) and pure serosorting (30.8%). No individual strategy was as common in the HIV-positive men (ie, all<30%). The most common behaviour pattern was pure serosorting (21.4%), and large proportions of men also practiced no sex and consistent condom use (16.3% each), as well as condom serosorting, seropositioning (13.3% each) and ‘no strategy’ (14.3%).
Prevalence (n, %) of seroadaptive and conventional risk reduction strategies, overall and stratified by HIV serostatus*, San Francisco, 2011
Among HIV-negative men, testing behaviour was associated with prevalence of individual behaviour patterns (p<0.001, table 2). Men who tested in the past 6 months reported more consistent condom use (36.9% compared with 26.9% for men who did not test in the past 6 months) and a lower frequency of no sex in the past 6 months (7.8% vs 23.4%). Though men who tested in the past 6 months reported lower adherence to conventional risk reduction behaviours (46.9% vs 53.8%), this difference was not statistically significant (p=0.254).
Seroadaptive and conventional risk reduction strategies (n, %) among HIV-negative men* stratified by HIV testing history†, San Francisco, 2011
Comparing between HIV-negative men reporting awareness of PrEP and those unaware of PrEP, the difference between individual behaviour patterns was not significant (p=0.418, table 3). However, in the aggregate, men unaware of PrEP reported a higher proportion of behaviour patterns with no UAI (57.5% vs 45.6% in men aware of PrEP, p=0.069), while men who were aware of PrEP were likelier to adhere to a seroadaptive strategy (50.5% vs 40.5%).
Seroadaptive and conventional risk reduction strategies (n, %) among HIV-negative men* stratified by awareness of PrEP, San Francisco, 2011
Among HIV-negative men, 35% reported an STI diagnosis; among HIV-positive men, prevalence was 57%. For men reporting STI diagnosis, prevalence of individual’s behaviour patterns varied significantly among HIV-negative men (p=0.002, table 4). HIV-negative men with no STI diagnosis reported higher rates of consistent condom use (35.3% vs 25.6% in men with an STI diagnosis), lower rates of seropositioning (3.4% vs 15.2%) and an overall higher rate of conventional risk reduction behaviours involving no UAI (56.9% vs 39.2% of men with an STI diagnosis, p=0.005). For HIV-positive MSM, individual behaviour patterns varied significantly (p=0.044). Compared with HIV-positive men with an STI diagnosis, HIV-positive men without an STI diagnosis reported higher rates of pure serosorting (26.2% vs 17.9%) and lower rates of seropositioning (7.1% vs 17.9%). In the aggregate, the rate of conventional risk reduction behaviours was similar among HIV-positive men with and without reported STI diagnosis (p=0.527).
Seroadaptive and conventional risk reduction strategies (n, %) among HIV-negative and HIV-positive men*, stratified by STI diagnosis†
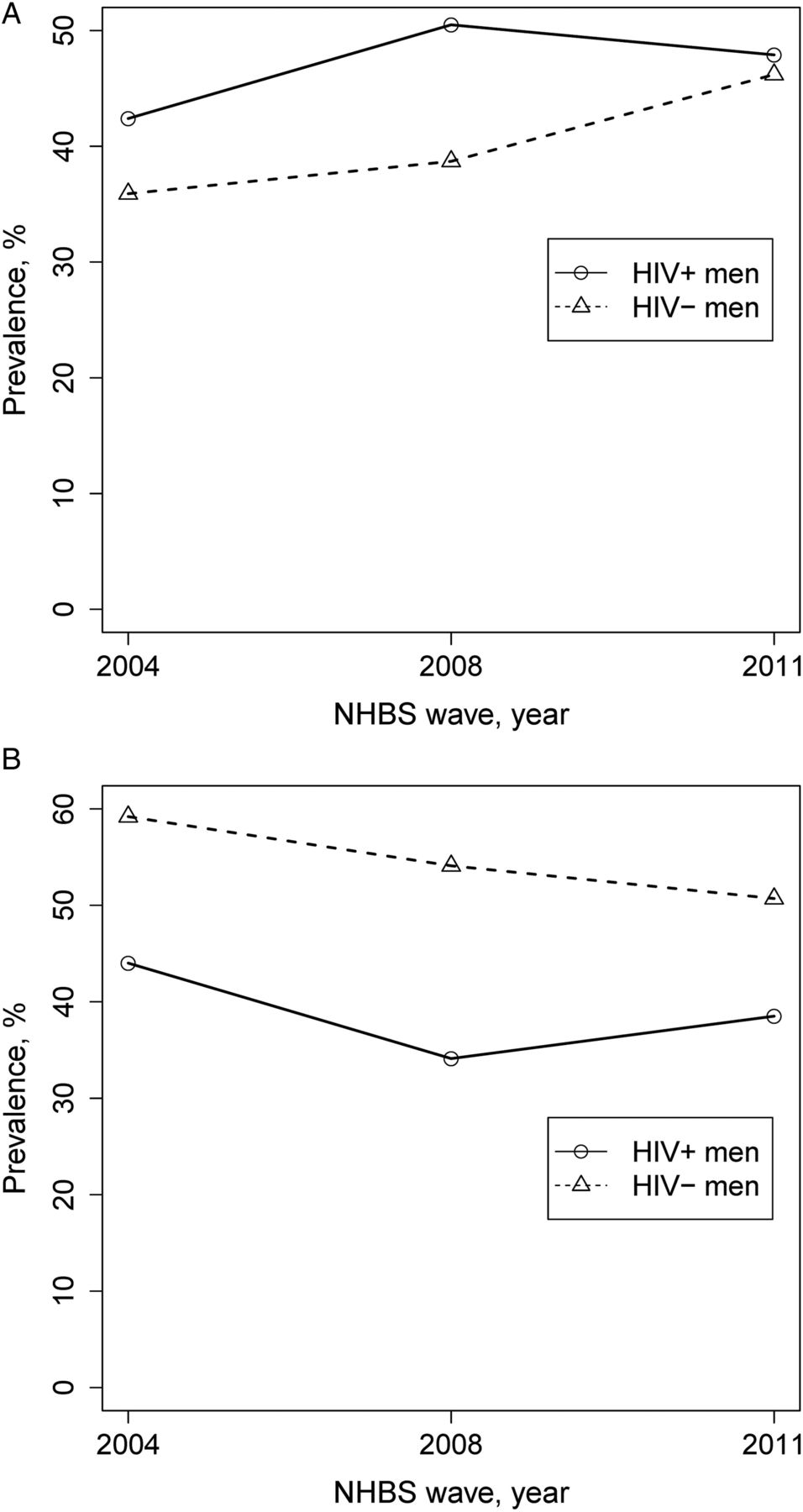
We examined temporal trends in seroadaptive behaviours by calculating the proportion of men reporting some seroadaptive behaviour and the proportion reporting some conventional risk reduction behaviour across the three waves of NHBS data (figure 1). Between 2004 and 2011, an increasing proportion of HIV-negative and HIV-positive men reported some seroadaptive behaviour (ie, had some UAI in the past 6 months). Among HIV-negative men, the proportion significantly increased from 35.9% in 2004 to 46.2% in 2011 (p<0.001 for trend, figure 1A). The rate also increased among HIV-positive men, peaking in 2008, and reaching 47.9% in 2011 (not statistically significant, p=0.251). Correspondingly, the proportion of men reporting a conventional risk reduction behaviour (ie, no UAI in the past 6 months) decreased among men of both serostatuses between 2004 and 2011 (figure 1B).
{kind=link}
Prevalence of (A) aggregate seroadaptive behaviors and (B) aggregate risk reduction behaviours not involving unprotected anal intercourse across three waves of National HIV Behavioral Surveillance data collection, San Francisco.
Discussion
The prevalence of individual seroadaptive strategies remained high and increased among San Francisco MSM from 2004 to 2011 (by more than 25% in HIV-negative men).5 ,11 HIV-negative men were more likely to adhere to a conventional risk reduction behaviour with no UAI compared with HIV-positive men who were more likely to engage in seroadaptive behaviour patterns and also to engage highest transmission risk sex.
We found key differences in behaviour patterns by health-related covariates. HIV-negative men who were aware of PrEP were less likely to report conventional risk reduction behaviours and likelier to report some seroadaptive behaviour pattern. HIV-negative men reporting STI diagnosis were also likelier to report a seroadaptive behaviour pattern and less likely to report a conventional risk reduction strategy—an association that logically follows engaging in UAI as defined by seroadaptive strategies. Taken together, these findings suggest that sexual health-related knowledge and sexual health history are associated with the practice of seroadaptive behaviours among HIV-negative men in San Francisco. Awareness of PrEP may be a proxy for intention to practice some strategic UAI or belonging to a social network that is more accepting of UAI. STI diagnosis is complicated because temporality of viral STIs is unknown. Practice of seroadaptive behaviours may increase risk of STI acquisition, and history of STI (especially in the case of viral STIs) may be a proxy for high-risk sexual behaviours including seroadaptive behaviours. Both factors are important in that they jointly play into the sexual risk for men who engage in seroadaptive behaviours.
The picture was more complicated for HIV testing, with no overall association between seroadaptive behaviours and recent testing. Having tested for HIV in past 6 months is likely a proxy for multiple factors, for example, intention to serosort or being sexually health conscious/risk-averse.
The limitations of this work must be taken into account when interpreting these findings. As in any analysis of sexual behaviour, data are limited by the accuracy of self-reported sexual behaviour information.30 Social desirability bias may be especially strong when specifically acknowledging placing others or oneself at highest risk of infection in an in-person interview. Furthermore, sexual risk reduction strategies and decision making are complex phenomena that resist simple classification. There are persistent questions about whether the behaviour patterns we describe here reflect intentional risk reduction strategies, post hoc justifications, availability of sexual partners, sexual preferences (self and partner's), chance or a combination of these factors.19 ,31 The proportions we present here apply to individual NHBS respondents and not sexual dyads or encounters; when considering these other levels of sexual risk, UAI is likely much less frequent.18 We lacked statistical power to stratify analyses by partner type, an important factor in determining partner selection and sexual behaviour in MSM. It is also impossible to verify the serostatus of the partners mentioned by respondents or the level of certainty with which the respondents knew their partners’ serostatus.
Our previous research attempted to address several of these concerns through a prospective study of seroadaptive behaviours in San Francisco.18 By assessing men's stated intentions for the ensuing year and measuring their reported behaviours a year later, we confirmed that a large proportion of men did intend to adhere to seroadaptive behaviours for risk reduction, but their adherence to these strategies was generally low (<50% in most cases). However, it is worth noting that adherence to seroadaptive strategies was not lower than adherence to risk reduction strategies that involve no UAI, such as 100% condom use.20 Thus, the issue of adherence to sexual behaviour intentions appears to cross-cut all preventive strategies for MSM and is a factor to consider across the board as public health officials continue to weigh the safety and effectiveness of seroadaptive strategies compared with conventional risk reduction. Given the complexity of documenting seroadaptive behaviours and their safety, additional prospective, longitudinal studies are warranted. Further, although analyses of seroadaptive behaviours commonly exclude men with unknown/unreported HIV status, future research should specifically analyse this group as they are of great interest for HIV prevention.
We found evidence that an increasing proportion of HIV-negative and HIV-positive MSM in San Francisco are practicing seroadaptive behaviour over the last 10 years, with an attendant decline in the proportion reporting no UAI in the past 6 months. A variety of factors may explain this trend. Temporal changes in social and sexual networks among gay and bisexual men (including the explosion of online and smart-phone brokered sexual encounters) might be correlated with changes in sexual risk behaviour.32 ,33 Encouragingly, our previous research has indicated that the differences between online and TLS samples of MSM may be small.34 Migration and changes in venue attendance in the city could also explain differences between the survey waves, especially given the recession during the years of the NHBS. Finally, there is a possibility that chance may explain our findings.
Nevertheless, this study confirms that seroadaptive practices, that is, those involving some instances of UAI, are a prevalent and persistent characteristic of sexual behaviour among MSM in San Francisco. Given the continued high level of seroadaptive behaviours in our sample populations, and the apparent decrease in men reporting no UAI in the previous 6 months, research must continue to study the prevalence and correlates of these behaviours in communities of MSM worldwide. Our data also suggest that the rollout of PrEP in San Francisco and the developed world may affect decisions on seroadaptive and conventional risk reduction strategies adopted by MSM, how they are communicated and how they are perceived in terms of transmission risk.27 While there is ample evidence of seroadaptive practices in developed countries,31 ,35 little is known about the adoption of these practices by MSM in the rest of the world, particularly considering lower levels of HIV testing and status awareness.36–38 As the established HIV epidemics in MSM in the developed world continue to evolve, and communities of MSM in the rest of the world become larger and more visible, a thorough understanding of seroadaptive behaviours—their prevalence, intentionality, effectiveness and safety—can help guide HIV and STI prevention efforts.
Key messages
-
The proportion of men whose behaviour can be described as seroadaptive increased from 2004 to 2011, with a corresponding decrease in men reporting no UAI.
-
Seroadaptive behaviours remain common in San Francisco MSM; they are more common than risk reduction strategies that do not incorporate unprotected anal intercourse.
-
Knowledge of pre-exposure HIV prophylaxis and diagnosis of a sexually transmitted infection were both associated with a higher propensity to practice seroadaptive behaviours.
References
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors JMS and HFR generated the concept of the paper. JMS conducted data analysis and drafted the manuscript. CW selected the key covariates of interest for the analysis. CW and HFR contributed to framing the questions and analysing the data. HFR provided primary oversight of the study, including data collection/management and manuscript preparation. WM provided overall scientific oversight of the study, including conceptualization of the research question and study methods, and made final edits to the manuscript. All authors edited the manuscript and approved the final version. All authors had access to the data and take responsibility for the integrity of the data and the accuracy of the data analysis.
-
Funding JMS is supported by grant R40 MC 25694-01-00 from the Maternal and Child Health Research Program, Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration, Department of Health and Human Services. CW is supported by grant R00MH093201 from the National Institute of Mental Health. NHBS activities are supported by grant U1BPS003247-01 from the Centers for Disease Control and Prevention.
-
Competing interests None.
-
Ethics approval Centers for Disease Control and Prevention, the University of California, San Francisco's Committee on Human Research and the Institutional Review Board of Oregon Health & Science University.
-
Provenance and peer review Not commissioned; externally peer reviewed.