Article Text

Abstract
Objective This study examines the proportions and causes of virological failure after one year of antiretroviral therapy (ART) among people living with HIV (PLHIV) in Vietnam. It also evaluates the positive predictive value (PPV) of immunological criteria to detect treatment failure.
Method A retrospective cohort of 3449 people with HIV who started ART between 1 January 2005 and 31 December 2009 in 13 outpatient clinics in Vietnam was studied. Multivariate logistic regression modeling was used to calculate crude and adjusted ORs and 95% CIs for associations between patient characteristics and virological failure.
Results An estimated 6.5% (226/3449) of HIV patients in the participating clinics in Vietnam had confirmed virological failure one year after the start of ART. After adjusting for other factors, patients with a baseline CD4 count of 50–100 cells/mm3 and 101–200 cells/mm3 were statistically significantly less likely to have virological failure, compared to those with a baseline CD4 count lower than 50 cells/mm3 (OR=0.61, 95% CI 0.23–0.89; and OR=0.43, 0.18–0.78, respectively). In contrast, patients with a history of injecting drug use were statistically significantly more likely to have viraemia than otherwise (OR=1.32, 1.16–1.67). The PPV of the WHO immunological criteria was 60.1% (57.1–69.3%).
Conclusions Routine viral load tests should be conducted early to detect virological failure and prevent unnecessary changes to second-line treatments. To improve treatment outcomes, timely ART initiation and adherence to treatment among those with history of injecting drug use should be promoted.
- VIROLOGY HIV
- ANTERETROVIRAL THERAPY
- HIV
- ADHERENCE
Statistics from Altmetric.com
Introduction
Failure of antiretroviral therapy (ART) is commonly diagnosed by clinical, immunological and virological criteria. Virological failure—that is, treatment failure diagnosed using virological criteria, occurs first, followed by immunological and then clinical failure—that is, treatment failures diagnosed using immunological and clinical criteria, respectively.1 Thus, viral load testing, which provides an early indication of treatment failure, is the preferred approach to monitoring treatment.1
In Vietnam, ART was first introduced in three clinics in Hanoi and Ho Chi Minh City (HCMC) in 2004. The number of ART sites increased from 74 in 2005 to 287 in 2009 and to 320 (including 305 sites for adults and 122 sites for children) in 2011.2 ,3 In 2012, a total of 63 provinces and cities had ART clinics. In addition to the greater number of sites, the availability of ART was further increased in 2010 when Vietnam adopted the WHO recommendation to start ART when CD4 cell counts are ≤350 cells/mm3, replacing the previous threshold of 200 cells/mm3.3
Patients receive group and individual counselling before starting ART. The standard first-line ART regimen is a fixed-dose combination of stavudine (2′,3′-didehydro-2′,3′-dideoxythymidine (d4T)), lamivudine (2′,3′-dideoxy-3′-thiacytidine (3TC)) and nevirapine (d4T-based therapy). Treatment response, drug side effects and treatment adherence are monitored 2 weeks after the start of treatment and monthly thereafter. CD4 cell counts are carried out for all patients before ART and every 6 months after starting treatment.4 In Vietnam, viral load testing is not routine in most outpatient clinics owing to high test costs (about US$50 per test) and the requirement for dedicated sample transport networks. It is mainly conducted to confirm treatment failure among those with immunological or clinical failure.5 Tests are carried out in only four laboratories located at the National Hospital of Tropical Diseases (HCMC), the National Institution for Infectious and Tropical Diseases (Hanoi), the National Institute of Hygiene and Epidemiology (Hanoi) and the Pasteur Institute (HCMC). These laboratories assess viral load using a real-time reverse transcriptase PCR assay (generic HIV viral load assay, Biocentric, Bandol, France), which has a detection threshold of 250 copies/mL4 This is a sophisticated nucleic acid-based method requiring well-functioning laboratory facilities supported by qualified technicians.5
To date three studies have examined the predictors of virological failure in Vietnam. They studied targeted viral load testing in 100 patients with HIV from a clinic in Hai Phong, a province in north Vietnam;6 228 patients from a clinic in HCMC, a province in south Vietnam;7 and a further 138 patients from 10 clinics in HCMC.8 These studies, however, examined the results from targeted, not routine, viral load testing, and such results are poor predictors of virological failure.1 Further, all three studies used single viral load test results, which might have been biased by transient increases in viral load.1 Although it is recommended that evaluation of possible treatment failure should be carried out at 6 months or 1 year after starting ART,1 none of these studies evaluated virological failure at these times. In addition to using small samples from one clinic or province, none of these studies investigated the reliability of using the WHO immunological criteria to detect treatment failure, despite their widespread use to detect treatment failure in Vietnam.
To deal with these gaps, this study aimed to (i) identify the proportion of HIV patients with virological failure one year after initiating ART, (ii) identify patient characteristics that are significantly associated with virological failure after 1 year of ART using two consecutive viral load tests to confirm failure, and (iii) examine the positive predictive value (PPV) of WHO immunological criteria to detect treatment failure by comparing it with viral load as a ‘gold standard’.1
Methods
Study design and sample size
The study population, comprising 3449 HIV-positive adults starting ART in Vietnam between 1 January 2005 and 31 December 2009 in 13 outpatient clinics in Vietnam, was examined retrospectively. Details of the cohort have been described in detail elsewhere.9 ,10 Briefly, 13 ART outpatient clinics were selected from six provinces of Vietnam: Hanoi, Bac Giang, Hai Phong, Quang Ninh, HCMC and Binh Duong. These provinces represent diverse geographical regions in Vietnam (eg, urban, rural, mountainous), including four provinces with a relatively high HIV prevalence (Hanoi (0.8%), Hai Phong (0.4%), Quang Ninh (0.3%) and HCMC (0.6%)) and two provinces with a relatively low HIV prevalence (Bac Giang (0.1%) and Binh Duong (0.2%)). The 13 clinics were at different levels of the state health system (eg, provincial, district) and received funding from different donors (eg, Global Fund, the National Program and the US President's Emergency Plan for AIDS Relief). Ethical approval was given by the Hanoi School of Public Health ethical review board (ethics committee approval number: 019/2011/YTCC-HD3) and the University of New South Wales ethical review board (ethics committee approval number: HREC 11321) before data were collected.
Data collection and measurements
Baseline information recorded at the start of ART was manually extracted by the first author and clinic staff and included demographics (age, gender, residential location and height and weight used to calculate the body mass index), HIV confirmation test date, history of injecting drug use (IDU), history of unsafe sex (USS), date of ART initiation, baseline CD4 count test date, referral source, initial ART regimen, presence of tuberculosis (TB) and other opportunistic infections at baseline, WHO clinical stage and co-trimoxazole (CTX) prophylaxis use before the start of ART. Time-dependent variables were also extracted from patient records, including viral load test results and dates, CD4 cell count test results and dates and treatment adherence. Adherence in the first year of ART was designated as ‘good’ for patients who self-reported their adherence rate as ≥95% and ‘poor’ for those who self-reported it as <95%.
The most recent CD4 cell count, 9–12 months after the start of ART, was used as the CD4 count after 1 year of ART. Viral load measured within the first 1 year of ART was used as the viral load after 1 year of ART. Virological failure was defined as two consecutive viral load tests ≥1000 copies/mL, and the date of the first viral load was used as the date of virological failure.
Data, collected between May and November 2010, were transferred into Microsoft Excel and 10% of the records were double-checked by the first and third authors. A total of 3499 patients were included in the analysis.
Statistical analysis
Mean values and SDs were calculated for the continuous variables age and baseline body mass index. Proportions of all patients were calculated for (i) WHO stage IV, (ii) history of IDU, (iii) history of USS, (iv) gender, (v) baseline TB, (vi) baseline opportunistic infections, (vii) baseline CTX use and (viii) treatment adherence.
Multivariate logistic regression modelling was used to calculate crude and adjusted ORs and 95% CIs, to examine associations between patient characteristics and virological failure (two consecutive viral load testing results >1000 copies/ml) (n=226), (Figure 1). All baseline demographics and HIV risk characteristics were included as explanatory variables. Univariate analysis was performed to identify the baseline characteristics that were likely to be associated with the outcome (p<0.25), and these variables were subsequently fitted into the initial multivariate logistic regression model. Of the variables that were not significantly associated with the outcome (p>0.05), the one that was least significant (highest p-value) was removed and the model was refitted with the remaining variables. This procedure was repeated in a backward stepwise manner until the final model was obtained, containing only those variables where p<0.05. All analyses were performed using SAS (version 9.2).
The PPV of immunological criteria was defined as PPV=number of true positives/(number of true positives + number of false positives) where a true positive result represents a patient who tested positive using both immunological and virological criteria and a false positive result represents a patient who tested positive using immunological criteria and negative using virological criteria.

{kind=link}
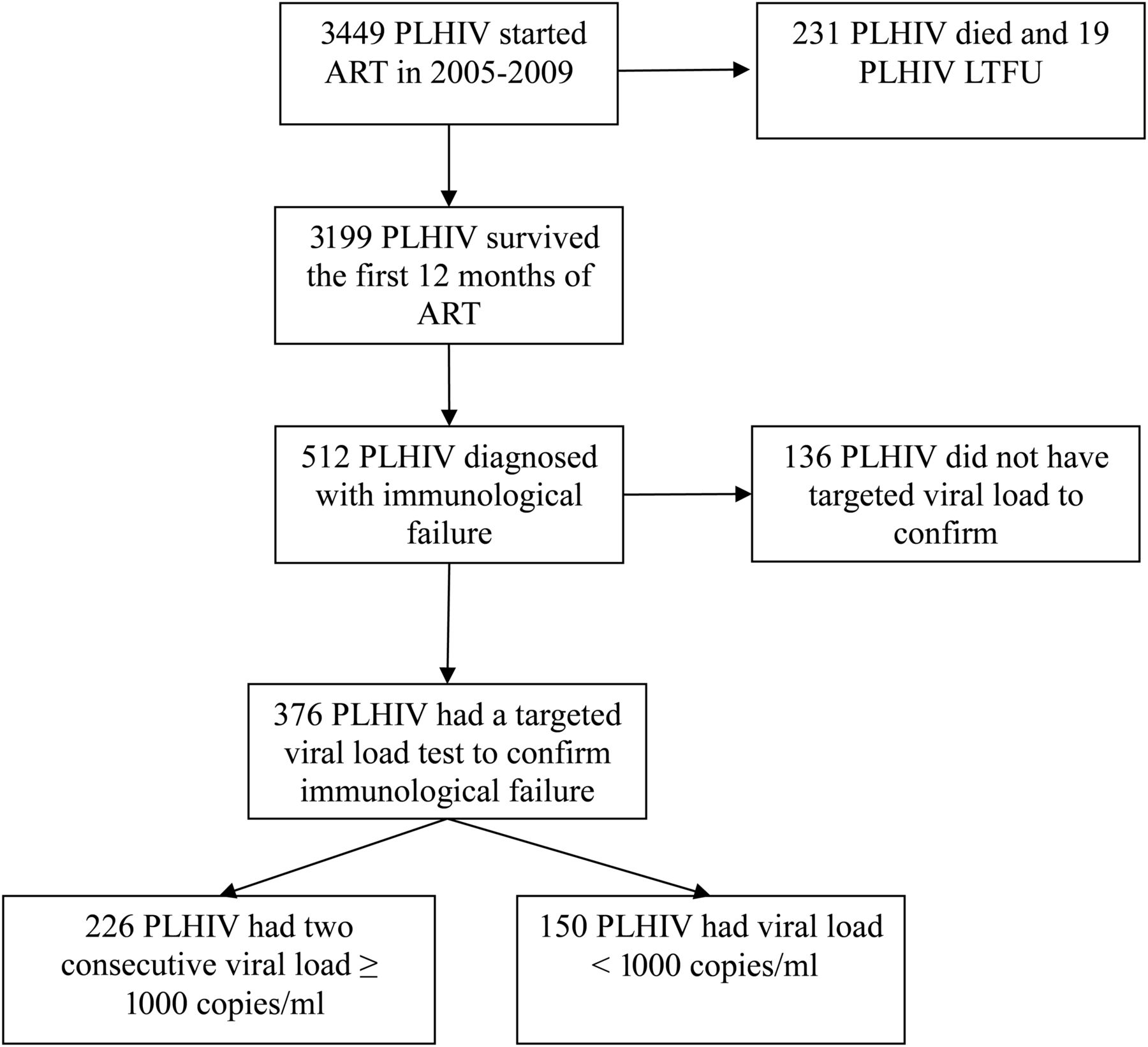
Access to routine viral load test of 3449 people living with HIV (PLHIV) in 13 outpatient clinics after 1 year of antiretroviral therapy (ART) started between 1 January 2005 and 31 December 2009. LTFU, lost to follow-up.
Results
Characteristics of the study cohort
A total of 3449 ART patients were included in the study between 1st of January 2005 and 31st December 2009, of whom 75% were males. The mean age at baseline was 30 years old and 65% were infected through sharing of injecting equipment (table 1). Figure 1 shows that of the 3449 patients, 231 died and 19 were lost to follow-up after 12 months on treatment. A total of 512 patients (14.8%) were diagnosed with immunological failure (using immunological criteria), of whom 376 (73%) had a subsequent viral load test and 226 (60%) confirmed their virological failure status.
Summary of baseline patient characteristics HIV infected patients in 13 outpatient clinics in Vietnam (N=3 449)
Patient characteristics significantly associated with virological failure after 1 year of ART
Findings from the multivariate logistic regression analyses of virological failure were presented in Table 2. Gender, age, baseline WHO stage, baseline TB, history of USS, baseline CTX and treatment adherence use were not significantly associated with virological failure in our analyses. However, after adjusting for other factors, patients with a baseline CD4 count of 50–100 and 101–200 cells/mm3 were statistically significantly less likely to have virological failure, compared to those with a baseline CD4 count lower than 50 cells/mm3 (OR=0.61, 95% CI 0.23–0.89; and OR=0.43, 95% CI 0.18–0.78, respectively). In addition, patients with a history of injecting drug use were statistically significantly more likely to have viraemia as those without a history of drug use (OR=1.32, 95% CI 1.16–1.67).
Multivariate logistic regression model of virological failure in people with HIV in 13 outpatient clinics in Vietnam (N= 376)
Positive predictive value (PPV) of WHO immunological criteria to detect treatment failure
Viral load testing was used as the gold standard to calculate the PPV of immunological criteria to detect treatment failure in this population.3 Among 376 patients in whom immunological failure occurred, 226 had HIV RNA counts >1000 copies/mL. The PPV of WHO immunological criteria was therefore 60.1% (95% CI 57.1% to 69.3%). Stratifying by specific immunological failure classifications, PPV was 56.7% (95% CI 47.8% to 69.0%) among those whose CD4 count declined to pre-ART levels, 61.4% (95% CI 58.1% to 68.2%) among those whose CD4 count declined to <50% of the peak while receiving ART and 64.1% (95% CI 57.2% to 69.8%) among those whose CD4 cell count was <100 cells/mm3 (table 3).
Positive predictive values (PPV, %) of immunological criteria to detect treatment failure after 1 year of antiretroviral therapy (ART)
Discussion
Study's strengths and implications
A major strength of this study is that it was conducted in 13 outpatient clinics in six provinces, representing diverse geographical regions and differing HIV prevalence in Vietnam. It is the first study to use two consecutive viral load test results to confirm virological failure. This study provides strong evidence to support routine viral load testing and draws attention to important gaps between immunological and virological monitoring strategies.
Key findings
Our study has three key findings. First, it showed that an estimated 6.5% (226/3449) of HIV patients in participating clinics in Vietnam had confirmed virological failure one year after ART initiation (two consecutive viral load tests with consistent results of ≥1000 copies/ml). Second, low baseline CD4 cell count and history of injecting drug use are significant predictors of virological failure. Third, the PPV of WHO immunological criteria in predicting treatment failure is low (60%) in the population studied.
The 27% patients who did not have their initial diagnosis of immunological failure confirmed by viral load test (136/512 patients, Figure 1) most likely reflects the unavailability of viral load testing in five of the six provinces included in this study (Dien Bien, Bac Giang, Hai Phong, Quang Ninh, and Binh Duong). Targeted viral load testing to confirm treatment failure before switching treatment regimens would be more effective if it could be performed universally throughout all Vietnamese provinces for patients diagnosed with clinical or immunological failure.1 This strategy may involve greater laboratory costs, but these costs are lower than those associated with second-line treatments,11 ,12 indicating a feasible cost-saving approach.11 ,12
Strategies to remove barriers to viral load testing, such as decentralising laboratory clinics, reducing viral load testing costs and increasing laboratory capacity, should be considered.13 Measurement of HIV viral load in Vietnam remains centralised, and is carried out by a limited number of laboratories. Decentralising these laboratories is one possible way of increasing access to viral load testing.13 However, decentralisation is difficult as it requires a trained primary health care workforce and a comprehensive quality management system, both of which require considerable resources. Consequently, this option is unlikely to be pursued in Vietnam where external funds have been reduced substantially.2 Point-of-care viral load testing may be a lower cost alternative for increasing access to viral load testing. However, this method has its own challenges as its reliability with the low viral load threshold used for virological failure (1000 copies/mL) has yet to be convincingly demonstrated.1 Another possibility, which has already been used for methadone treatment in Vietnam, is implementing a co-payment model. This payment strategy has proved successful in reducing the cost of methadone treatment and increasing willingness to pay among patients and has enhanced its use.14
Low baseline CD4 cell count was found to be significant predictors of virological failure one year after the start of ART, which is consistent with a number of other studies.15 ,16 These findings underline the importance of removing barriers to timely ART initiation. In Vietnam, a low baseline CD4 cell count is also an independent predictor of early mortality and LTFU.8 Furthermore, recent research has reported that 69% of people with HIV in a similar cohort did not initiate ART until their CD4 cell count dropped to <50 cells/mm3.17 Having a baseline WHO stage IV was not significantly associated with virological failure in our study although patients with a baseline WHO stage IV generally had low baseline CD4 cell counts and more advanced immune deficiency. However, this finding is in line with a number of studies in Uganda,18 Zambia,19 and Malawi.20
Poor treatment adherence was not a predictor of virological failure in our study. This finding is consistent with two similar previous studies in Vietnam4 ,5 but contradictory to findings from others.6 ,21 The absence of a statistical significance may be explained by the fact that patients were enrolled in these ART programs when their immunodeficiency was already too far advanced to protect them from treatment failure despite having good treatment adherence. Alternatively, this result may reflect the inconsistencies in measuring treatment adherence in different clinics. In Dien Bien, Bac Giang and Binh Duong provinces, for example, clinics relied on patients' self-reported adherence, while clinics in Hai Phong, Quang Ninh, and Ho Chi Minh city evaluated treatment adherence based on time to drug pick-up, time of appointments and history of ART drug stock-outs.
The finding that injecting drug users were more likely to experience virological failure is consistent with studies conducted in other developing country settings.22 ,23 The previously reported association between suboptimal treatment adherence among former and current IDU, compared to non-IDU may be a key explanation for this finding in our study,24 especially given evidence that most IDU continue to inject drugs even after initiating ART.25–27 Nevertheless, our study did not provide information on the current injecting drug-use status.
The PPV of WHO immunological criteria in predicting treatment failure was low in our study (60%). The limited utility of CD4 cell count changes to predict treatment failure found in this study is consistent with a number of previous studies.28 The PPV of immunological criteria was estimated to be 37% in South Africa,29 and 71% in India.30 Given this low PPV, our study supports the recommendation by Gale et al that the routine use of CD4 counts to monitor treatment progress, particularly among those who have viral suppression less than 200 copies/ml and CD4 count ≥300 cells/mm3, must be thoroughly examined.31
Study's limitations
This study has several limitations. First, our evaluation was limited to patients for whom viral load measured within the first 12 months of ART could be obtained, those retained in ART and those who had not been switched to second-line treatments within 12 months of starting ART. However, published data have indicated high early mortality and LTFU in the first year of ART.8 Those who died or were LTFU in the first year of ART are likely to have had treatment failure. Therefore, our results may be an underestimation of virological failure. Second, this study was limited to 13 outpatient clinics. Thus, the extent to which these findings are generalisable to all of Vietnam is unclear. Third, at the time of this study, all study clinics relied on patient self-reported treatment adherence. Without validation, the reliability of such self-reported adherence is uncertain. Finally, data used in this analysis were provided at the discretion of clinic staff, which resulted in incomplete data for some patients.
Conclusion
An estimated 6.5% (226/3449) of HIV patients in the participating clinics in Vietnam had confirmed virological failure one year after the start of ART. Among patients with confirmed virological failure one year after initiating ART, those who initiated ART at a later stage (CD4 cell counts of <50 cells/mm3) and who reported previous or current injecting drug use were statistically significantly associated with higher rates of ART treatment failure. WHO immunological criteria were found to have low PPV (60%) to predict treatment failure. Treatment adherence and the timeliness of ART should be improved to reduce treatment failure. Viral load testing within 6 months of ART is recommended for early detection of treatment failure and prevention of unnecessary moves to second-line treatments.
Key messages
-
6.5% (226/3449) of HIV patients in the participating clinics in Vietnam had confirmed virological failure one year after the start of ART.
-
Low baseline CD4 cell counts and a current or previous history of injecting drug use were significant predictors of treatment failure one year after the start of ART.
-
The positive predictive value of WHO immunological criteria in predicting treatment failure was low (60%); therefore, CD4 counts should be used less often, particularly among stable patients (who have viral suppression <200 copies/mL and CD4 count ≥300 cells/mm3).
Acknowledgments
We appreciate the support provided by Professor Anh Vu Le, head of Hanoi School of Public Health, and are grateful for the resources provided by the VINE project. We thank Associate Professor Peter Hill for technical support.
References
Supplementary materials
Editor's note
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
Footnotes
-
Correction notice This article has been modified. Please see the editor's note online.
-
Handling editor Jackie A Cassell
-
Contributors DAT collected the data, reviewed the literature, set up the model and drafted the manuscript. DPW helped in the data analysis. AS helped in the data analysis, provided editorial comments and contributed to drafting of the manuscript. ADN contributed to interpretation of the data and provided editorial comments. CD helped in data collection and provided editorial comments. LZ assisted with data analysis and contributed to editing the manuscript. All authors reviewed and agreed on the final version of the manuscript before submission. The corresponding author has full access to all data in the study and takes final responsibility for the decision to submit the paper for publication.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Hanoi School of Public Health and The University of New South Wales.
-
Provenance and peer review Not commissioned; externally peer reviewed.