Article Text

Abstract
Objective To test the hypothesis that a brief, clinic-based, single-session programme will reduce the rate of 10 selected condom use errors in a clinical sample of young black men (YBM) ages 15 through 23 years.
Methods Data were collected in clinics treating patients with sexually transmitted infections (STI) in three southern US cities. Males 15–23 years of age who identified as black/African–American, and reported recent (past 2 months) condom use were eligible. Only those also reporting condom use in the 2 months prior to a 6-month follow-up assessment (n=311) were included in this secondary analysis of data from a randomised, controlled trial. Difference scores were used to capture a Group×Time effect.
Results YBM reported 2232 condom use events in the 2 months preceding study enrolment and 2042 in the 2 months preceding the follow-up assessment. Mean baseline error rates were 1.32 and 1.13 for young men randomised to the intervention and control conditions, respectively. Follow-up rates were 1.11 and 3.59 for young men randomised to the intervention and control conditions, respectively. Controlled findings yielded a significant effect for the influence of group assignment on the difference score (baseline to follow-up) in the condom use error rate (β=0.13; p=0.02).
Conclusions A brief, clinic-based counselling programme produced modest reductions in condom use errors among YBM attending STI clinics in the southern USA Intensified clinic-based intervention that helps YBM improve the quality of their condom use behaviours is warranted.
Trial registration number NCT00849823.
- Contraception
- Sexual Behaviour
- Sexual Health
Statistics from Altmetric.com
Introduction
In the USA, young black males (YBM) continue to be disproportionately likely to acquire sexually transmitted infections (STI), including infection with HIV.1–5 Of more than 21 000 new HIV infections occurring among black US residents each year, approximately 34% occur among those 13–24 years of age. The problem is most pronounced in the southern USA.6–8
Condom use remains a primary public health strategy to prevent HIV and other STIs in YBM.9–11 However, evidence strongly suggests that condoms are only efficacious when they are also used correctly.12 Despite the urgency to prevent infections with HIV and other STIs among YBM, most research on male condom errors and problems has neglected this population. However, one clinic-based intervention has demonstrated efficacy in reducing STI incidence among black males 18–29 years of age.13 A central premise of that single-session programme was that teaching YBM to overcome issues with condom use errors would lead to improved quality of condom use (eg, less breakage and slippage) and even more frequent use. Indeed, an emerging body of evidence indicates specific errors in condom use that predispose men to experience condom failures.14–19
To date, intervention studies have not specifically investigated whether a brief, clinic-based intervention for YBM who are very young (less than 24 years of age), can effectively reduce their rate of condom use errors. Accordingly, the purpose of this study was to test the hypothesis that a brief, clinic-based, single-session programme will reduce the rate of 10 selected condom use errors in a clinical sample of YBM ages 15 through 23 years. Data for this study were drawn from a randomised, controlled trial (under review) of a HIV prevention programme designed for YBM residing in southern USA.
Methods
Study sample
A convenience sample of 702 YBM was recruited for participation from a larger NIH-funded randomised controlled trial (RCT) of a safer sex intervention programme designed for this population. This secondary analysis was conducted subsequent to the final analysis of the intervention trial. A pretest, post-test design was used for this RCT, with follow-up assessments occurring 2 and 6 months after randomisation. The 10 selected condom use errors used for the current study were not analysed as part of the planned outcome measures in that RCT. The study was registered with Clinical Trials.gov (Protocol ID: 080666/Clinicaltrials.gov ID: NCT00849823).
Recruitment occurred in clinics that diagnose and treat STIs. Inclusion criteria were: (1) self-identification as black/African–American; (2) aged 15 to 23 years; (3) engaged in penile-vaginal sex at least once in the past 2 months; and (4) not knowingly HIV-positive. Recruitment occurred from approximately 2010 through 2012, in a primary site (New Orleans, Louisiana, USA) and two secondary sites (Baton Rouge, Louisiana and Charlotte, North Carolina, USA). Age-eligible black males were approached in clinic waiting rooms and asked about their interest in volunteering for an HIV prevention study. Those expressing interest were screened for eligibility and those meeting the requirements were then invited to enrol. The overall study participation rate was 60.4% (n=702). The 6-month retention rate among young men randomised to the intervention condition was 78.5%, with a comparable (p=0.16) rate for those in the control condition (73.9%). For this secondary analysis, only YBM who reported recent (past 2 months) condom use at baseline and at the 6-month follow-up assessment were eligible (n=311; 153 assigned to the intervention condition and 158 to the control condition). Figure 1 displays the flowchart showing how the analytic subsample was obtained (web-only version).
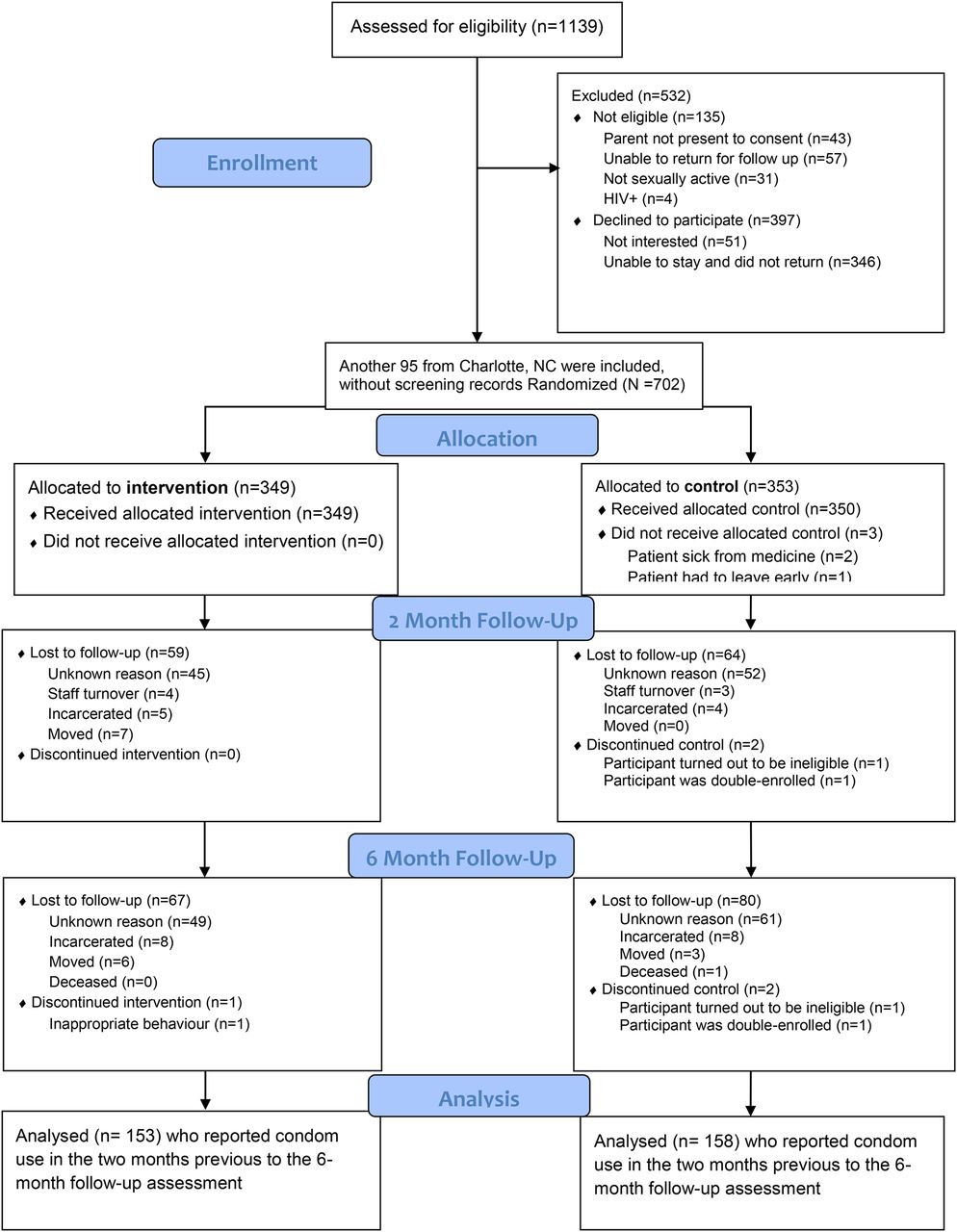
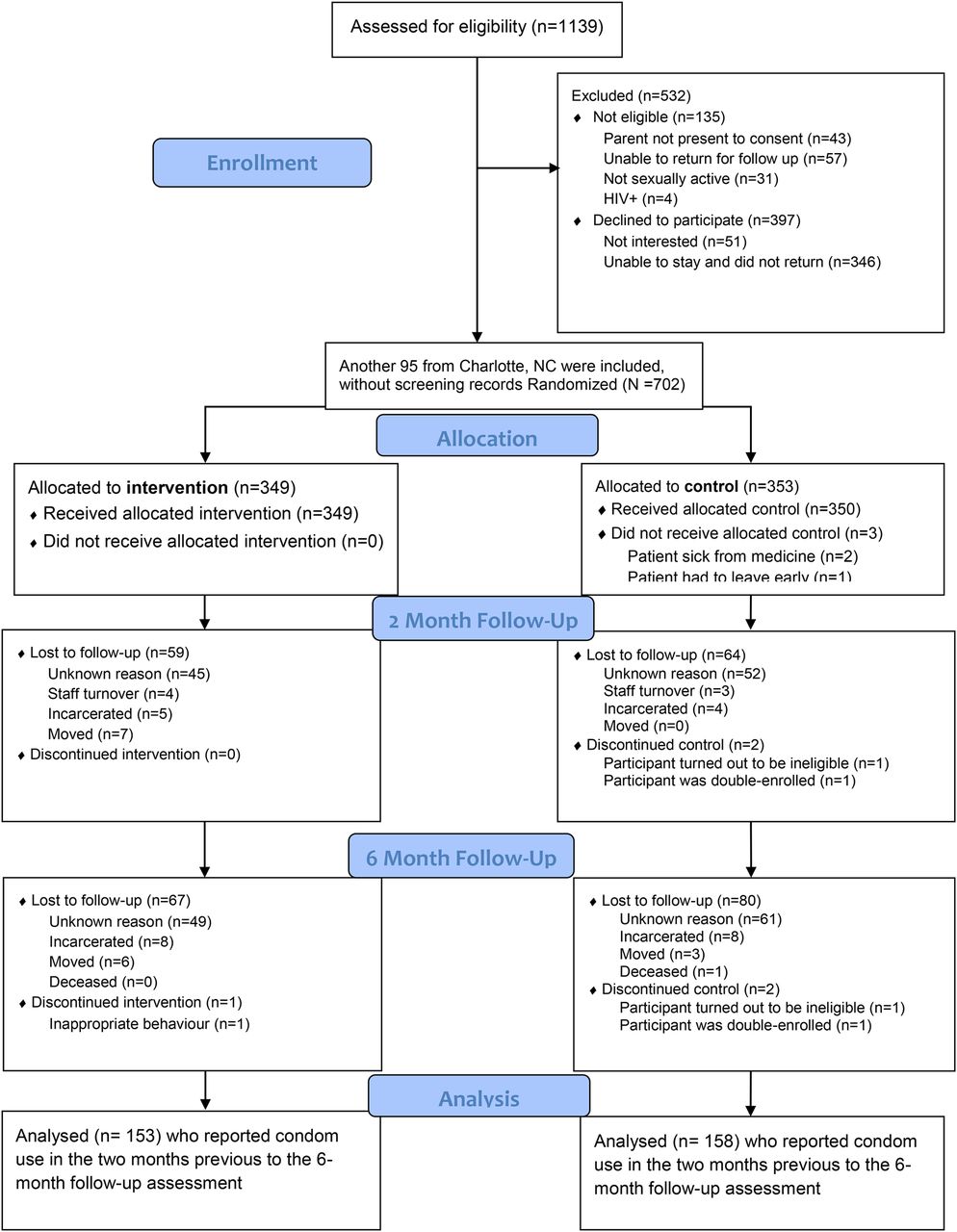{kind=link}
Enrolment and Allocation.
Study procedures
After providing assent, research assistants asked young men less than 18 years of age for their permission to contact one parent or guardian to obtain consent for study participation. Young men aged at least 18 years old provided written informed consent. After enrolment, an audio computer-assisted self-interview (A-CASI) survey was administered. YBM were instructed in the use of a laptop computer to complete the A-CASI, lasting approximately 30 min. The A-CASI was completed in a private area with a research assistant being available to clarify wording if needed. Using a concealment of allocation technique, randomisation to condition then occurred. This technique uses index cards labelled ‘Intervention’ or ‘Control’ that are placed in envelopes that are randomly shuffled and kept in that same random order for use, with the top envelop always being used for the next assignment. The intervention condition was an adapted version of Focus on the Future.13 This is a highly interactive and sex-positive programme that uses a brief (less than 60 min) single-session format delivered on a face-to-face basis. The session provided young men with motivation and skills needed to practice the correct and the consistent use of condoms for the prevention of STIs, including HIV. The control condition was entirely didactic and consisted of 40 PowerPoint slides focused on male and female reproductive anatomy, basic knowledge of various STIs (gonorrhoea, chlamydia, syphilis, herpes, trichomoniasis, human papillomavirus (HPV) including genital warts, and HIV). Young men in both conditions were provided with free condoms and lubricants; all were also provided with a US$50 gift card. Six months after completing the baseline assessment, the young men were prompted to return to the clinic to complete the same A-CASI survey; at which time another US$50 gift card was provided. The study protocol was approved by the institutional review boards at all participating sites.
Measures
A brief version of the Condom Use Errors/Problems Survey was employed.20 This 10-item index was created based on empirical evidence suggesting the most likely errors that men experience when using condoms.11–22 The online supplementary table S1 displays the actual questionnaire items (web-only version). The index used a 2-month recall period. YBM were specifically instructed by the A-CASI that ‘sex means anytime you had vaginal or anal sex’ and they were asked to reply to these items using that definition of sex. Each item was prefaced with the stem, ‘In the past two months…’ and sequentially posed questions such as (1) ‘…did you completely unroll the condom before putting it on your penis?’ Items also measured whether (2) condoms contacted sharp objects, (3) were initially placed on the head of the penis with the wrong side facing up, (4) not unrolled all the way down to the base of the penis, (5) were unrolled without holding the receptacle tip to expel air, (6) unlubricated condoms were used, (7) YBM wanted to add lubricant to condoms but did not have any, (8) oil-based lubricants were used, (9) a problem occurred with a condom that required a new one to be used, and (10) condoms did not fit or feel good on the penis. Response options assessed how many times the error occurred.
Two measures of sexual behaviour were also assessed using a 2-month recall period, at baseline and the follow-up assessments. First, frequency of condom use for penile–vaginal sex was assessed. Subsequently, frequency of condom use for penile–anal sex was assessed. These measures were combined to provide distributions of reported penetrative sex frequency at baseline and at the follow-up session. Also, based on previous evidence suggesting a strong influence of having multiple sex partners on condom use errors,13 ,21 ,22 the number of penetrative (penile–vaginal and penile–anal) sex partners was assessed for the 2 months preceding the follow-up assessment. Finally, at baseline, young men's sexual orientation was assessed as either heterosexual or gay/bisexual.
Data analysis
A summative score of condom use errors was calculated for the baseline and follow-up assessment periods. To obtain the rate of errors, these summative scores were divided by their respective number of condom use events. Rates were then compared between groups at baseline and follow-up sessions. A difference score (to test for Group×Time effects) was then generated by subtracting the 6-month error rate from the baseline error rate. This difference score was then compared by group assignment using an independent groups t test. Using multiple linear regression, the difference score was then regressed on group assignment and three identified covariates (number of sex partners preceding the follow-up assessment, sexual orientation and age). Significance was defined by an α of 0.05. All analyses were conducted using SPSS, V.20.0.
Results
Characteristics of the sample
The mean age of the sample was 19.8 years (SD = 1.8 years). About one-half (52.9%) reported attending school. Most (70.4%) had graduated from high school. The vast majority (95.1%) received public assistance of some kind. An income of less than US$500 per month was reported by 48.2% of the sample. All YBM self-reported having at least one STI in the past. Baseline testing conducted as part of the randomised trial found that 17.9% of participants tested positive for chlamydia and/or gonorrhoea. The mean number of penetrative sex partners reported for the 2 months prior the follow-up assessment was 3.56 (SD=7.30). About one of every seven young men (13.1%) identified as gay or bisexual.
Descriptive findings
A summative score of the errors was produced for the baseline and 6-month assessments. The baseline score yielded a mean of 6.49 errors, with a SD of 13.47 and a range of 0–123, with 94 of the 311 young men indicating an absence of errors. The 6-month score yielded a mean of 6.17 errors, with a SD of 25.27 and a range of 0–385, with 123 of the 311 young men indicating an absence of errors.
In combining the measures of condom use for penile–vaginal sex with those for penile–anal sex, the sample reported 2232 condom use events in the 2 months preceding study enrolment. In the 2 months preceding the follow-up assessment, the total number of condom use events reported was 2042. These values were used as denominators to calculate rates of errors reported at baseline and follow-up sessions. Because multiple errors occurred for many young men during single events of condom use, these rates exceed the value of 1.00. The mean baseline error rate was 1.22 (SD=2.18; range=0–25, with 97 young men indicating 0). The mean follow-up error rate was 2.33 (SD=12.52; range = 0 to 160, with 123 young men indicating 0).
Baseline error rates were 1.32 (SD=2.55) and 1.13 (SD=1.73) for young men randomised to the intervention and control conditions, respectively. An independent groups t test indicated equivalence in these two rates (t=0.78, df=309, p=0.44). Follow-up rates were 1.11 (SD=3.73) and 3.59 (SD=17.41) for young men randomised to the intervention and control conditions, respectively. An independent groups t test indicated a marginal difference in these two rates (t=1.75, df=309, p=0.08).
Findings
A difference score in the rates reported as baseline and those reported at follow-up was calculated. The mean difference score for the intervention group was 0.21, indicating a modest improvement in errors over time. The mean difference score for the control group was −2.47, indicating an increase in the number of errors over time. An independent groups t test yielded marginal significance (t=1.90, df=309, p=0.06).
The multiple linear regression model was significant (F=10.03; df=4304; p<0.001). Controlled findings yielded a significant effect for the influence of group assignment on the difference score in the condom use error rate (β=0.13; p=0.02). The control variable (number of penetrative sex partners in the past 2 months) was also significantly associated with the difference score β=−0.30; p<0.001), with the inverse value indicating a decline in the difference score as the number of partners reported increased. Age was not significantly associated with the difference score (β=−0.04; p=0.45). Finally, sexual orientation was significantly associated with the difference score (β=−0.13; p=0.02), with the inverse value indicating a decline in the difference score for young men not identifying as heterosexual.
Discussion
This secondary analysis (involving more than 4000 condom use events) of an RCT demonstrates that a brief, clinic-based intervention has the ability to reduce the frequency of condom use errors among high-risk YBM engaging in penile–anal and/or penile–vaginal sex with females and/or males. By virtue of their attendance to STI clinics, this sample stands apart from a population-based sample of YBM. This reduction in condom use errors may be an especially important contribution to STI prevention given that these young men may practice higher-quality condom use throughout their lifetimes. Clearly, STI clinics are well positioned to offer one-to-one teaching sessions that instruct and motivate YBM to improve the quality of their existing condom use behaviours. This type of low-intensity intervention is consistent with recent recommendations from the USA Preventive Services Task Force.23 Also worth noting is that a recent RCT (enrolling more than 5000 patients) found no effects of HIV post-test counselling to promote safer sex on STI incidence.24 It is possible that one reason this programme did not work involves inadequate attention to the reduction of condom use errors. Given the frequency of errors observed in our study, increased emphasis on correcting these errors during counselling sessions is certainly warranted.
The observed intervention effect is intriguing because only a modest reduction in condom use errors was reported by young men randomised to the intervention condition. Instead, the effect was created by a rather large increase in errors reported by those in the control condition. This set of findings suggests that demand characteristics (ie, intervention participants answering assessment questions with responses they perceive as being consistent with what they learned during the intervention session) were probably not operating simply because that phenomenon would have produced a much greater decline in condom use errors for those receiving the intervention. It is, however, plausible that condom use errors may naturally increase over time (as occurred in the control group) as a function of becoming progressively less intent on using condoms perfectly with each passing use of condoms. The findings suggest that a similar increase would have occurred for the intervention group in the absence of the programme. The observed influence of number of partners and sexual orientation was also intriguing, with findings suggesting that reduction in errors is more likely for those having a greater number of sex partners and for those identifying as heterosexual. Thus, intervention efforts targeting YBM who identify as heterosexual may need to be more intensive compared to those not making this identification. Each of these colliery findings warrants further empirical investigation.
Of importance, it should be noted that YBM were recruited from clinics that diagnose and treat STIs in three southern US cities. Condom use errors were common, and occurred across all phases of the condom use process. These errors may be a prominent source of condom failure issues such as breakage and slippage among YBM throughout the South. Magnified over such a large population at elevated risk of STI acquisition and transmission, the observed baseline error rate may substantially detract from the existing efforts YBM are making to protect themselves and others against STIs. A recent study of more than 900 clinic-attendees found that condoms were not protective against non-viral STIs unless the occurrence of problems such as breakage and slippage was factored into the analysis.12
Limitations
The geographic diversity of the sample is limited to patients attending STI clinics, thus, generalisability of the findings to other populations of YBM is problematic. Also, study findings are limited by the validity of participants’ self-reports of condom use errors and their frequency of condom use. However, problems associated with recall are minimised by the use of a short recall period. The one disadvantage of the 2-month recall period is that it could serve only as a proxy of the reductions (or increases) in errors over the 6-month period of the RCT.
Conclusion
Brief, clinic-based, intervention programmes may have the potential to serve as part of a larger public health response to the AIDS crisis experienced by African–Americans as well as the co-occurring STI epidemic in this population. In particular, the findings from this study suggest a potential in relationship to a modest reduction in condom use errors; one that was contrasted to what may have been a natural increase in errors among those not receiving the intervention programme.
Key messages
-
Among young black males attending sexually transmitted infection clinics in the USA, errors and problems with condom use may be common.
-
The frequency of condom use errors and problems among young black males may increase over time in the absence of education designed to avert these occurrences.
-
A brief, clinic-based, condom education programme delivered to young black males may actually reduce the occurrence of condom use errors and problems.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors Both authors, RC and LFS made substantial contributions to the conception or design of the work, the acquisition, analysis and interpretation of data. They were involved in the drafting the work or revising it critically for important intellectual content. Both authors also gave final approval of the version to be published, and both agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Funding This study was funded by a grant from the National Institute of Mental Health to the first author, R01MH083621.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval University of Kentucky Office of Research Integrity.
-
Provenance and peer review Not commissioned; externally peer reviewed.