Article Text

Abstract
Objective In the Netherlands, men who have sex with men (MSM) are advised via informal guidelines to test for STI at least annually. We estimated the proportion of HIV-negative MSM testing repeatedly at 12-month or smaller intervals at a large STI clinic in the Netherlands. In addition, we explored whether repeated testing is related to risk behaviour.
Design and methods Longitudinal data of HIV-negative MSM visiting the Amsterdam STI clinic between 2009 and 2012 were analysed. To estimate the timing of repeated testing, Kaplan–Meier methods were used. Determinants for repeated testing (distinguishing testing at 12-month or smaller intervals and less than 12-monthly testing, with single testers as reference group) were identified using multivariate multinomial logistic regression analyses.
Results In total, 19 479 consultations of 9174 HIV-negative MSM were identified. Of these MSM, 35% (95% CI 33% to 36%) were estimated to return to the STI clinic within 1 year following baseline consultation. Among 1767 men with at least two consultations and at least 2 years between baseline and last consultation, 43% tested repeatedly at 12-month or smaller intervals in those first 2 years. Repeated testers reported higher sexual risk behaviour (ie, only casual or both casual and steady sex partners, higher numbers of sex partners) at baseline compared with single testers. This effect tended to be slightly stronger for men testing repeatedly at 12-month or smaller intervals.
Conclusions The proportion of MSM testing for STI annually is low. MSM testing repeatedly had higher baseline levels of risk behaviour. Strategies to motivate MSM to test annually should be explored.
- TESTING
- HOMOSEXUALITY
- GUIDELINE DEVELOPMENT
Statistics from Altmetric.com
Introduction
In many Western European countries, new HIV infections are predominantly diagnosed among men who have sex with men (MSM) and rates of STI in this group are high.1 ,2 Prevention of STI/HIV and regular testing for STI/HIV among MSM are therefore considered important.
An Australian study estimated that annual HIV testing among MSM could significantly reduce HIV incidence.3 Several countries recommend annual testing, like the US Centers for Disease Control and Prevention (CDC) and Australia who recommend in their guidelines annual STI/HIV testing of sexually active MSM and more frequent STI/HIV testing (ie, at 3–6-month intervals) for MSM practising high-risk behaviour.4 ,5 In Europe, official guidelines regarding the frequency of STI/HIV testing for MSM are lacking, but many physicians and healthcare workers in several European countries recommend annually testing for MSM and 6-monthly testing for MSM practising high-risk behaviours.6
As in other European countries, the Netherlands has no official guidelines about testing frequency of MSM. A major Dutch non-governmental organisation, however, recommends sexually active MSM to test at least 6-monthly.7 The STI clinic in Amsterdam tends to advise MSM to return for testing, which is offered free and anonymously, after 6–12 months depending on the reported risk behaviour (personal communication T. Heijman of the STI clinic, Amsterdam). We used longitudinal data from the Amsterdam STI clinic over a 4-year period to gain insight into the proportion of HIV-negative MSM following the advice of testing at 12-month or smaller intervals. In addition, we explored whether repeated testing is related to risk behaviour by comparing characteristics of repeated and single testers.
Methods
Study population and design
We selected longitudinal data of all consultations of HIV-negative MSM attending the Amsterdam STI clinic between 1 January 2009 and 31 December 2012. The Amsterdam STI clinic covers approximately 40% of all MSM consultations reported at STI clinics in the Netherlands. STI test results and information about demographics, sexual behaviour and STI history at every consultation were registered in an electronic patient file. An anonymous patient identification code allowed linkage of sequential consultations of an individual. The STI testing procedures are described in detail elsewhere.8
MSM is defined as a man who reported having sex with a man at least once in the past 6 months at any visit during the 4-year study period. MSM who tested HIV positive during the study period were included up to, and including, the first positive test consultation. MSM who opted out for an HIV test (4% at last consultation), and therefore had an unknown HIV status, were also included. MSM participating in screening programmes or research protocols with regular planned visits were included up to, and including, the moment they entered such a programme. Examples of such programmes include the high-risk MSM screening programme (not yet published) and the H2M study on the relation of HPV and HIV.9 In addition, men were fully excluded if they (1) ever participated in the Amsterdam Cohort Study during the study period;10 (2) ever tested through outreach screening programmes and (3) ever tested through the online MSM screening programme (http://www.mantotman.nl). During outreach activities, healthcare workers visit locations that MSM often attend, like bars, ‘cruising areas’ and saunas, to offer a test directly at the location. Men ever tested through outreach were excluded since their STI-testing behaviour could be influenced by these activities. Through the online screening programme MSM can anonymously test for STI at a laboratory in Amsterdam. Only referrals to the STI clinic following a positive test result were registered in the database; therefore, these men were excluded.
Statistical analyses
First, a description of the study population was given, including a comparison of characteristics of MSM at the included and excluded consultations.
Second, to gain insight into the timing of testing, we estimated the cumulative probability of returning for a subsequent consultation following the first consultation after the start of the study period, hereafter baseline consultation, using Kaplan–Meier methods. Follow-up was defined as the time from baseline consultation until the end of the study period (ie, 31 December 2012), a HIV-positive diagnosis or entry into a screening programme, whatever occurred first. Time to event was calculated as the time from baseline consultation until the subsequent consultation (ie, the event). Time to event was censored at the date of the end of follow-up when there was no event.
Third, we estimated the proportion of men testing repeatedly for STI at 12-month or smaller intervals among those with at least two consultations. The proportion was described separately for MSM with at least 2 and 3 years between baseline and last consultation. To rule out the possibility that a person was not included because he came shortly after the 12-month time period, we set an upper margin of 1 month, meaning that all consultations within 13 months were included.
Finally, we used multivariate multinomial logistic regression analysis to identify independent determinants of (1) men testing repeatedly, but less than 12-monthly and (2) men testing repeatedly at 12-month or smaller intervals, both relative to men testing only once (ie, single testers). This analysis was restricted to 3935 MSM with at least 2 years of follow-up. The multivariate model included demographical and sexual behavioural covariates describing risky behaviour for gaining an STI. In addition, we adjusted for place of residence which is a proxy for distance to the clinic. Since the number of sex partners had a very skewed distribution and the effect was expected to be non-linear, these values were transformed to the logarithmic scale.
Results
Description of study population
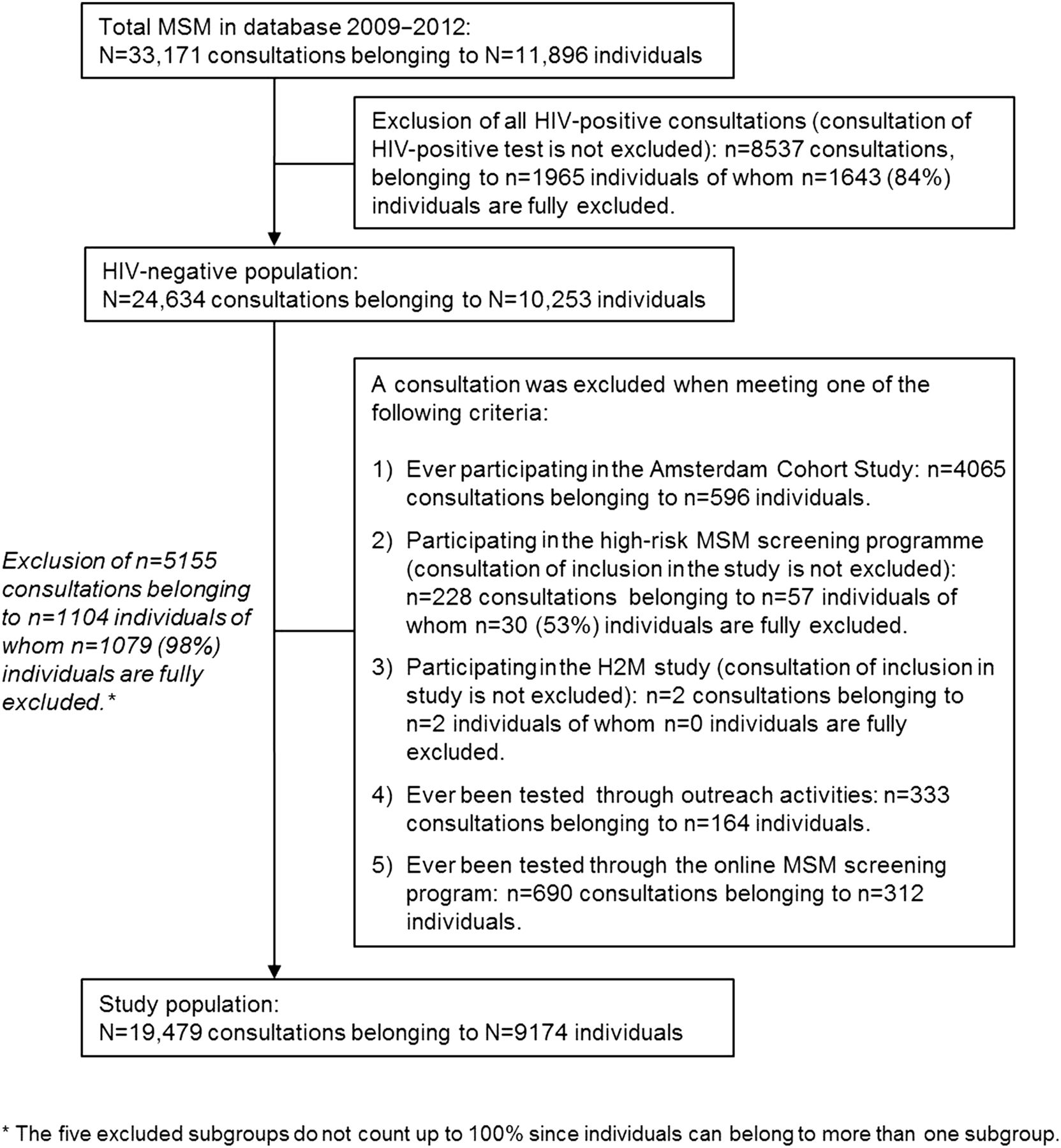
Within the 4-year period, 11 896 unique MSM visited the STI clinic accounting for 33 171 new consultations. In total, 8537 consultations of known HIV-positive MSM and 5155 consultations of HIV-negative MSM participating in screening programmes or research protocols were excluded (figure 1). This resulted in a study population of 9174 HIV-negative MSM accounting for 19 479 consultations.
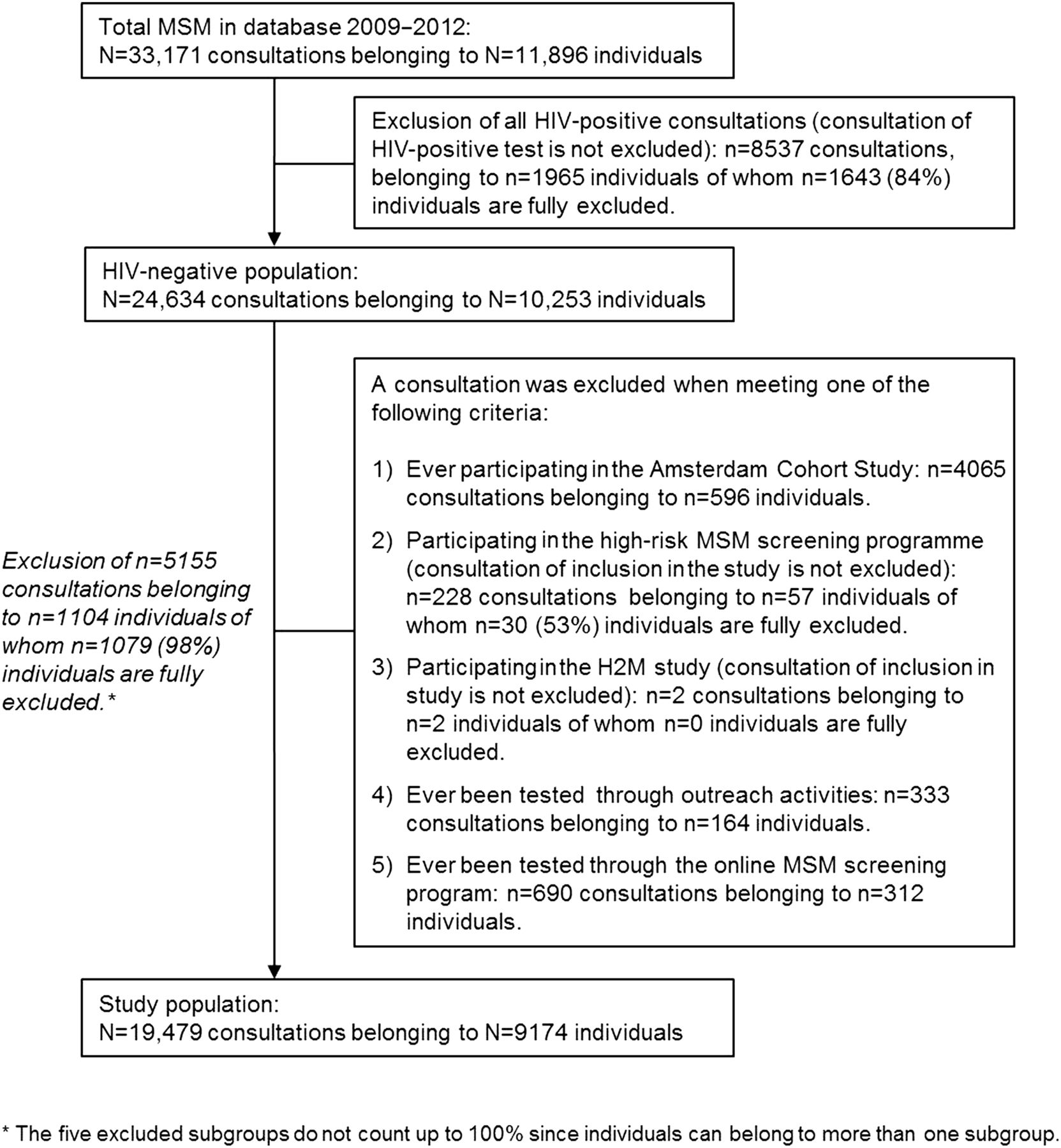
Flowchart of the excluded population. MSM, men who have sex with men.
Comparing characteristics of MSM at the included consultations with those of HIV-negative MSM at the excluded consultations, included men were slightly younger (median: 35 years (IQR: 28–45) vs 38 years (IQR: 33–43), respectively), were less often of Dutch ethnicity (69% vs 85%, respectively) and lived less often in Amsterdam (73% vs 77%, respectively). The median number of reported sexual partners in the preceding 6 months at included and excluded consultations was similar (5 (IQR: 3–10) vs 5 (IQR: 2–12), respectively), and the STI positivity was slightly higher at the included versus the excluded consultations (18% vs 16%, respectively).
Timing of STI testing
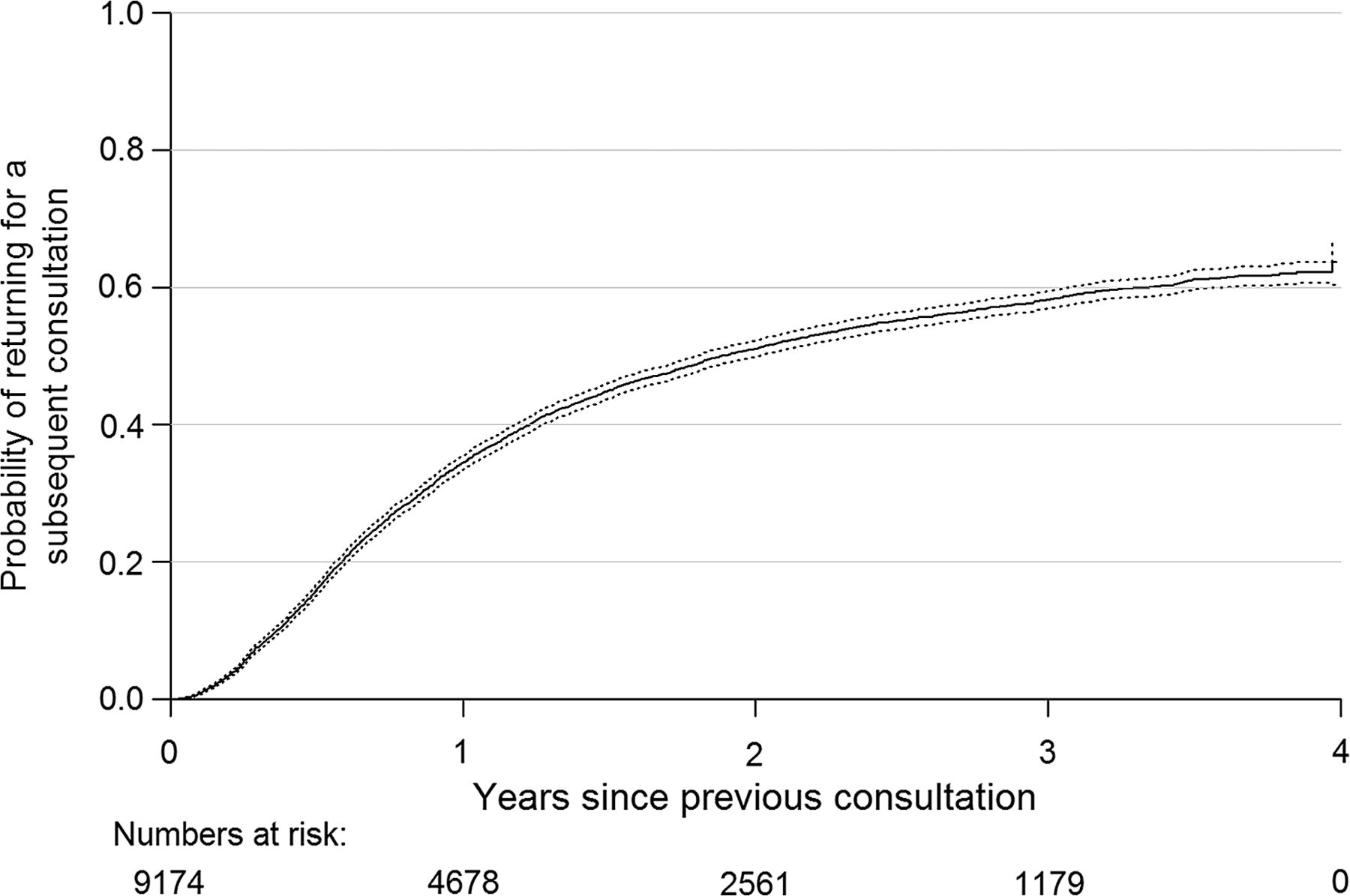
Using Kaplan–Meier methods, we estimated that 16% (95% CI 15% to 17%) of men returned for a second consultation within 6 months following baseline consultation, 35% (95% CI 33% to 36%) of men returned within a year, 51% (95% CI 50% to 52%) within 2 years and 64% (95% CI 61% to 67%) within 4 years (figure 2).
{kind=link}
{kind=link}
Kaplan–Meier curve showing the probability (including 95% CIs (=dashed lines)) of returning for a subsequent consultation following baseline consultation at the Amsterdam STI clinic between 2009 and 2012.
Repeated 12-monthly STI testing
In total, 4170 men (45%) had two or more consultations during the study period. Of the men with multiple consultations and at least 2 years between baseline and last known consultation (n=1767), 43.4% tested repeatedly at 12-month or smaller intervals during the first 2 years following baseline consultation. When selecting men with at least 2 years between baseline and last consultation (n=691), only 36.0% tested repeatedly at 12-month or smaller intervals during these 3 years following the baseline consultation.
Independent determinants of repeated STI testing
Men who were of Western origin other than Dutch and men living elsewhere in the Netherlands and not reporting their residence, including men refusing to provide their zip code, being homeless and tourists, all at the baseline consultation, were less often repeated testers (table 1). Men who reported sex with both genders in the past 6 months were also less likely to test repeatedly in comparison with men who had sex with men only, whereas men who reported sex with women only in the past 6 months were more likely to test repeatedly. The type of partner also played a role in repeated testing. Men with only casual or both casual and steady partners in the past 6 months were more likely to test repeatedly in comparison with men with only steady partners. Also, the higher the number of sex partners a man had in the past 6 months, the larger the odds of repeated testing. Having unprotected anal intercourse in the past 6 months and STI test results at baseline did not have a significant effect on the testing frequency of men.
Independent determinants of MSM testing repeatedly at 12-month or smaller intervals and of MSM testing less than 12-monthly, both relative to single testers, among 3935 MSM attending the STI clinic between 2009 and 2012 with at least 2 years of follow-up
The effect of type of sex partner and the number of partners tended to be slightly stronger for men testing repeatedly at 12-month or smaller intervals than for men testing repeatedly but less often. This indicates that sexual risk behaviour is an important determinant of whether or not an MSM would return within a year or later.
Discussion
To our knowledge, this is the first study using longitudinal data over a 4-year period to explore repeated annual STI testing among HIV-negative MSM. Our main finding is that annual testing at the Amsterdam STI clinic is not common. We also found that MSM were more likely to test repeatedly when reporting sexual risk behaviour.
Where other studies only analysed time until first subsequent consultation11 ,12 or primarily measured through cross-sectional surveys whether individuals had been tested in the preceding year,13 ,14 we prospectively studied all consultations of HIV-negative MSM within a 4-year period. This enabled us to provide insight into the proportion of men returning within a year for a subsequent consultation, and into the proportion of men testing repeatedly at 12-month or smaller intervals. Furthermore, we were able to provide information about predictors of repeated testing. These results give insight into how well the informal Dutch testing advice of at least 12-monthly testing is followed.
Data used in the analyses were primarily collected for clinical purposes at the STI clinic which has its limitations. Probably the most uncertain factor in our study is the lack of information about STI tests at locations outside the Amsterdam STI clinic (eg, general practitioner (GP), hospital or other STI clinics). Self-reported data from three surveys, the European MSM Internet Survey,15 the Schorer Monitor16 and a large survey among lesbian women, MSM and transgender people,17 suggested that half to two-thirds of HIV-negative MSM living in Amsterdam had their last HIV test at locations outside the STI clinic. Although we believe that STI testing elsewhere is limited for the majority of our STI clinic population as testing is free of charge and anonymous, this might have led to an underestimation of the number of consultations per individual.
There is also some uncertainty about unique visitors. Since identification is not required at the STI clinic, unique visitors can have multiple patient files, making it impossible to identify repeated consultations for those individuals. Although we do not have insight into the percentage of men with multiple patient identifiers, this group is expected to be small. Another point of notice is that although the estimated proportion of tourists among the total population is around 1% (data not shown), inclusion of this subpopulation could also have led to an underestimation of repeated testing. A final point, during the study period, screening and research programmes took place at the STI clinic. Consultations of MSM participating in one of these programmes were excluded in this study. However, we do not think that the exclusion of these consultations biased our results much since observed differences in demographical and sexual behavioural characteristics between included and excluded HIV-negative consultations were small. Moreover, only less than 5% of MSM were partially excluded and therefore the number of falsely single consultation will be low.
Our results showed that a third of men returned within a year following their baseline consultation (based on Kaplan–Meier methods) and less than half of men with multiple consultations and at least 2 years between baseline and last consultation tested repeatedly at 12-month or smaller intervals (based on descriptive analyses). Based on these estimations, we may conclude that the majority of men do not follow the informal testing advice of at least one test per year. An explanation for this low testing frequency could be the lack of clear guidelines on STI-testing frequency. However, Australia found similar numbers in a retrospective cohort study among HIV-negative MSM attending a GP or STI clinic,11 regardless of their official guidelines.5 This indicates that the low testing frequency is due to other factors as well. MSM might be poorly motivated to regularly return for a subsequent STI test or there might be a barrier to test at STI clinics. In the Netherlands, MSM are tested for all STI at the STI clinic except for HIV to which they may opt out. This mandatory full testing package could have led to the decision of not testing or testing for HIV outside the STI clinic. Offering the possibility to test for HIV only might result in an increased testing frequency if there is indeed a barrier with testing for all STI. In line with this hypothesis, the results of the Dutch survey among lesbian women, MSM and transgender people showed that the percentage of HIV-negative MSM testing for HIV in the preceding year is higher than the percentage of HIV-negative MSM who tested for all STI.17
Possible reasons for the low testing rates should be further investigated to provide information for possible strategies to increase testing frequency. When testing frequencies stay low, the impact of testing on the HIV incidence in the total population may be low. A recent modelling study from Australia, using comparable HIV prevalence rates as estimated for the Netherlands,18 estimated that only above an annual HIV testing coverage threshold of approximately 30% among the total MSM population, HIV incidence would decrease after 10 years and the observed number of newly diagnosed HIV cases would start to decline.3 When annual testing coverage would be below 30%, as we estimated in our study, HIV testing would still have an impact on HIV incidence, although the impact would be smaller and no decline in HIV diagnoses is likely to be observed.
Based on our results, it appears that repeated testing is driven by men suspecting an STI, due to risky behaviour. However, a group not considered at high risk for STI were men who reported having sex with women only in the past 6 months. Although this group of men was small, we found that they tended to test more frequently in comparison with men who only had sex with men. To gain more insight into this specific group of men, we compared their characteristics with men who reported having sex with men only in the previous 6 months. Men who reported having sex with women only were younger, more often of non-Western ethnicity, reported having a steady partner only, protected or no anal intercourse, had less sexual partners and were diagnosed more often with an STI. These findings might indicate a group of young men who have recently began exploring sex with men and also a group of men belonging to cultures where homosexuality is still stigmatised. As a result, information about their sexual experiences with men during the specific consultation may have been withheld. It is also possible that the men in this group did not have any male sexual contact in the past 6 months. Having a steady heterosexual relationship may have increased concern in this group of men about infecting their partner, due to past sexual experiences. More research into this group is necessary to identify if this is a possible hidden population to which STI prevention strategies should also be targeted.
Another interesting group were men of Western ethnicity other than Dutch. These men tested less frequently in comparison with Dutch men. This could be explained by these men living for only a specific period in the Netherlands. In addition, it is possible this group of Western men prefer to go for medical visits in their own country.
In conclusion, repeated annual STI testing in MSM in Amsterdam appeared to be low, especially over a longer time period. This study highlights the need to evaluate the implementation of testing guidelines and recommendations. The consequences for HIV and STI incidence if MSM do not annually test for STI need to be assessed, as well as the effect of different testing frequencies on STI incidence. It should be explored whether STI testing guidelines based on the reported level of risk behaviour would be easier to implement and to adhere to, as well as its effect on reducing HIV and STI infections. Finally, if MSM should test more frequently, as our results imply, novel strategies should be explored on how to motivate them.
Key messages
-
No uniform guidelines about STI-testing frequency for men who have sex with men (MSM) exist in Europe, including the Netherlands.
-
Repeated testing for STI/HIV is not common among HIV-negative MSM.
-
Repeated testers report slightly higher sexual risk behaviour in comparison with single testers.
Acknowledgments
The authors would like to thank M. van Rooijen for the data management and P. van Leeuwen for input with respect to the study design and STI procedures.
References
Supplementary materials
Abstract in Dutch
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Dutch - Online abstract
Footnotes
-
Handling editor Jackie A Cassell
-
Contributors HJV, IGS, JCMH, TH, HJCdV, RBG, MABvdS, MP contributed all to the study design and analysis. The analyses were undertaken by HJV supported by IGS, JCMH and RBG. HJV, IGS, TH, MP and HJCdV interpreted data and results for the STI clinic. HJV wrote the first draft of the manuscript, with the assistance of all coauthors. All authors contributed to and approved the final manuscript.
-
Funding Our study was funded by the Ministry of Health, Welfare and Sport of the Netherlands, which had no role in the design, conduct or reporting of the study.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.