Article Text

Abstract
Objectives Recently, we reported a high prevalence (16%) of urogenital Chlamydia trachomatis infections among women in a rural setting in South Africa. Molecular epidemiological studies on C. trachomatis infections could provide insights into the characteristics of this epidemic, yet such data are not available. The objective of this study was therefore to assess the distribution of C. trachomatis strains among women from a South African rural community, the Mopani district, and to compare it with strains from Amsterdam, the Netherlands.
Methods High-resolution multilocus sequence typing (hr-MLST) was used to study urogenital C. trachomatis infections in women visiting primary healthcare facilities across rural Mopani District in Limpopo Province, South Africa. Sequence types (STs) were compared with 100 strains from women visiting the sexually transmitted infection clinic in Amsterdam, the Netherlands.
Results Full hr-MLST data were obtained for C. trachomatis infection in 43 women from Mopani district. Using the complete hr-MLST profile of all 43 women from Mopani district, 26 STs could be identified, of which 18 (69%) were novel to the hr-MLST database. The remaining STs clustered together with strains from Amsterdam.
Conclusions Hr-MLST data revealed a diverse molecular epidemiology with novel STs and a specific cluster for the Mopani district. Also C. trachomatis types that occur worldwide were detected.
- CHLAMYDIA TRACHOMATIS
- CHLAMYDIA INFECTION
- BACTERIAL TYPING
Statistics from Altmetric.com
Introduction
Chlamydia trachomatis is the most common bacterial sexually transmitted infection (STI) worldwide. Recently, we reported a high prevalence (16%) of urogenital C. trachomatis infections among women in a rural setting in Mopani district, South Africa.1 This reported prevalence was higher compared with other studies in South Africa.2
Molecular epidemiological studies could inform prevention campaigns and health policy development by providing insight into the transmission of C. trachomatis infections in South Africa, and could therefore help to detect specific populations and networks at risk. However, molecular epidemiological data of C. trachomatis infections are not available for South Africa. Therefore, we investigated the molecular epidemiology of urogenital C. trachomatis infections among women in Mopani District, South Africa, using high-resolution multilocus sequence typing (hr-MLST) to assess the distribution of C. trachomatis strains in this population and to compare the distribution with a sample of strains from Amsterdam, the Netherlands.
Methods
This study is a subanalysis of a larger cross-sectional study as described elsewhere.1 In brief, a cross-sectional study was conducted among 604 women visiting 25 randomly selected primary healthcare facilities across rural Mopani district in Limpopo Province, South Africa. Participants were recruited between November 2011 and February 2012. Women aged 18–49 years who reported at least one sex act in the past 6 months were eligible. Data on demographics, sexual behaviour, self-reported HIV status and STI related symptoms were obtained through questionnaires. STI related symptoms were defined as having abnormal vaginal discharge, intermenstrual bleeding, blood loss during or after sexual intercourse, or dysuria. Vaginal swabs were tested for the presence of C. trachomatis DNA using the CE-IVD certified PrestoPlus CT-NG-TV assay (Goffin Molecular Technologies, Beek, The Netherlands) and the cobas 4800 CT/NG test (Roche Molecular Diagnostics, Pleasanton, CA, USA). Swabs were transported to VU University Medical Center in Amsterdam and stored at −20°C until further processing.
DNA extracts were amplified by a nested PCR and sequenced for the regions ompA, CT046 (hctB), CT058, CT144, CT172 and CT682 (pbpB).3 The cleaned primer-to-primer sequences were checked against the C. trachomatis hr-MLST database (http://mlstdb.bmc.uu.se). Only samples in which all six loci were successfully amplified, sequenced and identified obtained a full hr-MLST sequence type (ST) and were included for further analysis. Minimum spanning trees were generated with BioNumerics 7 (Applied Maths, Sint-Martens-Latem, Belgium) using the STs. A cluster was defined as a group of STs differing by not more than one locus from another ST within that group (single locus variance) and had to include at least 5% of the total number of samples.
The identified C. trachomatis clusters were compared with Dutch samples obtained from female visitors of the STI clinic in Amsterdam, the Netherlands. Matched C. trachomatis-positive urogenital samples were randomly selected for 100 women who were described in a previous study.4 We selected at least one C. trachomatis infected woman from Amsterdam, for each C. trachomatis infected woman from the Mopani district in order to get a weighted minimum spanning tree.
Differences in demographic data between participants from the two countries were tested using Pearson's χ2 test for categorical data and Mann-Whitney U test for continuous data. Analyses were performed with SPSS V.21 (SPSS, Chicago, Illinois, USA).
Results
In total, 97 from 604 (16%) women from Mopani district were diagnosed with urogenital C. trachomatis infection. Of those, 85 samples (88%) were available for further typing analysis. In 54 of 85 samples (64%), sufficient quantity of chlamydial DNA could be demonstrated using qPCR, and for 43 (51%) full hr-MLST profiles were obtained. Characteristics of these 43 women are shown in online supplementary table S1. The median age of South African women was 26 years (IQR, 22–30). Most of these participants reported to have had one sexual partner in the previous 6 months. Seven women (16%) were HIV-positive, 25 (58%) were HIV-negative and the remaining 11 (26%) had an unknown HIV status. More than half (n=26; 61%) of the women experienced STI related symptoms. Significant demographical differences were seen between women from the Mopani district and from the randomly selected group from the Amsterdam population (see online supplementary table S1).
Since ompA is part of the hr-MLST scheme, genovars could be assigned to all samples. Among the women in Mopani district, we identified 8 different genovars: D, 37% (n=16); E, 12% (n=5); F, 7% (n=3); G, 21% (n=9); H, 2% (n=1); I, 2% (n=1); J, 14% (n=6); and K, 5% (n=2). This genovar distribution differed when compared with the distribution found among women in Amsterdam (see online supplementary table S1, p<0.001). Using the complete hr-MLST profile of all 43 South African women, 26 STs could be identified, of which 18 (69%) were novel to the publicly available C. trachomatis hr-MLST database (http://mlstdb.bmc.uu.se).
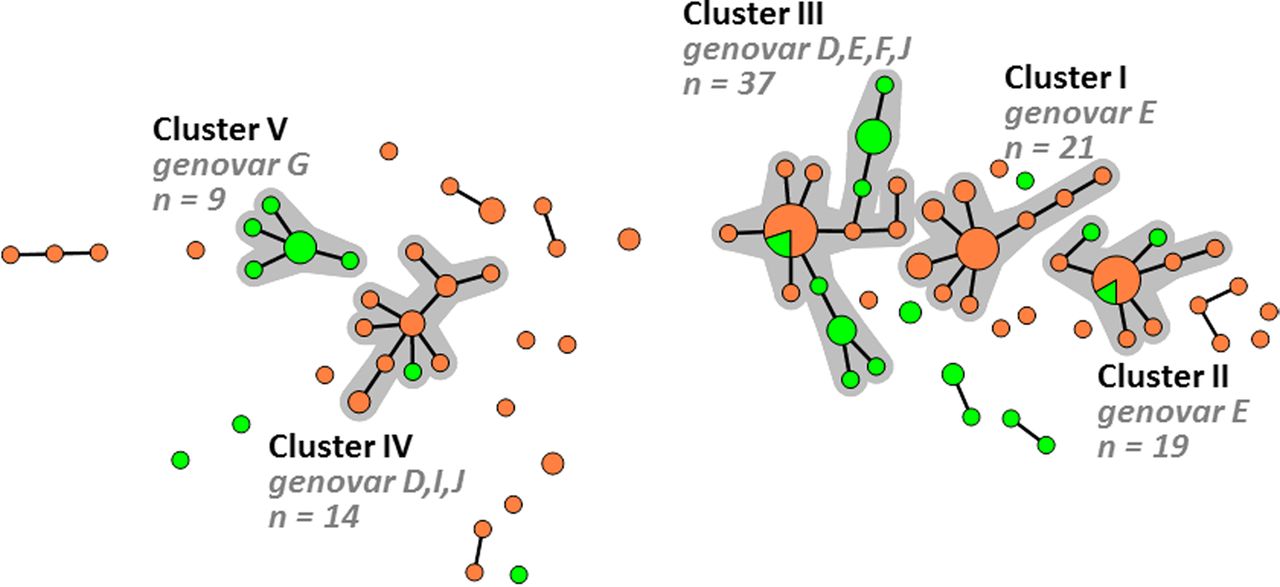
A minimum spanning tree was generated, using 43 samples from Mopani district and 100 reference samples from Amsterdam, in which five large clusters could be identified (figure 1). Cluster I (n=21) consisted exclusively of samples from Amsterdam, whereas cluster V (n=9) consisted exclusively of samples from Mopani district. Cluster III (n=37) was a mixed cluster and contained nearly equal numbers of samples from Amsterdam (51%) or Mopani district (49%). The remaining clusters II, IV and the residual group were also mixed clusters, but consisted predominantly of samples from Amsterdam (74–93%). However, despite the mixed clusters only two STs were identical for samples from Mopani district and Amsterdam.
{kind=link}
Minimum spanning tree showing the high-resolution multilocus sequence typing (hr-MLST) pattern of 43 Chlamydia trachomatis positive samples from Mopani district, South Africa (2011–2012) and 100 reference samples from Amsterdam, The Netherlands (2012). Each circle represents one sequence type (ST). Size of the circles is proportional to the number of samples with identical ST profiles, the smallest circles representing one sample. Bold lines connect types that differ for one single locus. Halos indicate the distinct clusters. Colours indicate location of sampling; green: Mopani district, South Africa (n=43) and orange: Amsterdam, the Netherlands (n=100).
Discussion
In this study, we identified C. trachomatis strains that are specific to Mopani district, and we identified STs that have not been described before and are completely novel to the international hr-MLST database (http://mlstdb.bmc.uu.se). We also observed C. trachomatis strains that were present in both geographical locations.
In Mopani district, genovars D, G, J and E were most prevalent whereas in Amsterdam genovars E, D, F, I and J were most prevalent. Using hr-MLST, we observed that clusters of C. trachomatis strains associated with both countries were mostly mixed. Only two clusters could be associated with either Mopani district (cluster V) or Amsterdam (cluster I). The remaining clusters and the residual group contained samples from Mopani district and Amsterdam, indicating C. trachomatis strains that were genetically closely related but not identical on both locations. Only two STs were identical (ST-12d and ST-3). We recently reported similar findings for Nanjing, China, as we observed specific strains for Nanjing, but also others that clustered together with strains from Amsterdam.5 Interestingly, we now observed identical STs between Amsterdam and Mopani district that were also shared between Nanjing and Amsterdam. A possible explanation for the occurrence of these identical strains is sexual mixing between partners from both geographical locations. However, this sexual mixing is highly unlikely for these populations, given the geographical distance. In addition, the rural and traditional population in the Mopani district is infrequently visited by tourists and foreigners. The occurrence of identical STs in these geographically distant locations is therefore most likely explained by the genomic stability of some C. trachomatis strains over a long period of time and these STs may be regarded as ‘founder strains’. Another possibility is that these strains have an intrinsic factor for successful infection in humans all over the world.
Besides geographical variation, we also observed demographic differences between women from Mopani district and Amsterdam due the totally different study populations (see online supplementary table S1). However, these differences in age, number of sex partners, STI related symptoms and HIV status are associated with the acquisition of a C. trachomatis infection, and not with the distribution of different C. trachomatis types of strains.6–9 Therefore, it is unlikely that these demographic differences explain the observed C. trachomatis strain distribution.
Some potential limitations of this study should be noted. A large proportion of the samples from Mopani district was excluded due to insufficient amount of chlamydial DNA for typing after long-term storage. This resulted in a small sample size and a potentially biased population. It is, however, unlikely that we missed specific strains using our inhouse qPCR and hr-MLST methods, since for qPCR conserved nucleotide sequences of the pmpH gene are targeted, that proved to have good diagnostic performance.10 In addition, hr-MLST regions were randomly missed in all partially typed samples, suggesting that no specific strains were missed. Moreover, this study was conducted in a rural area of South Africa and was limited to only one district. Therefore, this study cannot be considered representative for the distribution of C. trachomatis strains in other regions of the country or continent. Using this limited population, we nevertheless show a diverse molecular epidemiology with novel STs and a specific cluster for the Mopani district. A larger study with inclusion of more healthcare facilities in rural and urban areas of South Africa could therefore provide further valuable insight into the molecular epidemiology and transmission of C. trachomatis. This knowledge may be essential to inform prevention campaigns and health policy design.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Abstract in Dutch
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Abstract in Dutch - Online abstract
Footnotes
Handling editor Jackie A Cassell
Acknowledgements The authors thank Michelle Himschoot for technical assistance and expertise. The authors also thank Jolein Pleijster, Dewi de Waaij en Stephan Verweij for CT detection, Lisette van der Eem for cohort collection in South Africa and Dr Sander Ouburg for STI detection coordination.
Contributors RPHP, SMB and SAM contributed to the design of this study to assess the distribution of Chlamydia trachomatis strains in Mopani district. RPHP and JHD collected the samples and data. SAM, JHD and RPHP were involved in the testing of samples for C. trachomatis positivity. BV carried out the hr-MLST typing. BV, SMB and RPHP performed the data analyses. BV and SMB drafted the paper. All authors contributed to the interpretation of the results, writing the manuscript and gave intellectual feedback. All authors have contributed to, have seen, and approved the final, submitted version of the manuscript.
Funding This work was supported by the Public Health Service of Amsterdam, the Netherlands and the Dutch Society for Tropical Medicine (NVTG), the Netherlands.
Competing interests SAM, full-time employee of the VU University Medical Center Amsterdam, has been involved in the technical development of the PRESTO-Plus CT-NG-TV assay (marketed by Goffin Molecular Technologies, Houten, the Netherlands) via Microbiome.
Ethics approval Human Ethics Research Committee of the University of the Witwatersrand, South Africa. (Ref: M110726).
Provenance and peer review Not commissioned; externally peer reviewed.