Article Text

Abstract
Background Qualified decision-making for the improved management of sexually transmitted infections (STIs) requires various sources of information. We aimed to estimate the STI-associated symptom prevalence and care-seeking patterns in the general population of Iran.
Methods In 2014, using a street-based survey with a standard gender-specific questionnaire on STI-associated symptoms and willingness to seek treatment, we interviewed 9166 Iranian participants, who were selected from among the 18–60-year-old population using multistage sampling. Data were analysed via generalised estimating equation and survey analysis, taking into account a 95% confidence coefficient.
Results About 67.3% of participants, mean age 33 years, were ‘assumed sexually active’ and were therefore eligible for inclusion. Approximately 39.9% (95% CI 28.4% to 51.4%) of women and 17.6% (95% CI 13.9% to 21.6%) of men reported at least one STI-associated symptom in the current week. The occurrence of symptoms decreased with an increase in age in both genders (p<0.05). About 21.2% (95% CI 13.3% to 29.1%) of women and 7.1% (95% CI 5.4% to 7.8%) of men treated symptoms themselves after symptoms first appeared. Of the women and men with symptoms, 37.4% (95% CI 24.8% to 50.0%) and 46.8% (95% CI 39.7% to 51.4%), respectively, sought care. Most women visited a gynaecologist and midwife; men tended to visit a general practitioner and urologist after their symptoms appeared.
Conclusions The prevalence of STI-associated symptoms in Iranian adults is considerable. The results emphasise the need for appropriate and timely STI care and more attention to sexual health promotion to mitigate onward and future infections. Attention to the care-seeking pattern is fundamental to policymaking and planning.
- EPIDEMIOLOGY (GENERAL)
- SEXUAL HEALTH
- CLINICAL STI CARE
Statistics from Altmetric.com
Introduction
It is estimated that worldwide, approximately one million sexually transmitted infections (STIs), including HIV, are diagnosed daily.1 Data point to a high incidence and prevalence of STIs in developing countries.2 ,3 Based on registered data in Iran, in 2014 about 9000 cases of urethral discharge and 3000 cases of genital ulcers occurred among men. About 1700 confirmed cases of gonorrhoea and 5500 confirmed cases of chlamydia were reported in women and men; the number of confirmed cases of gonorrhoea and chlamydia in women also considerably exceeded that of men, resulting in experts questioning the validity of diagnoses and/or reporting (Center for Disease Control and Prevention, 2014).4
Iran, located in the Eastern Mediterranean and North Africa region, has a population of 75.14 million, of which 71.4% lives in urban areas, where the majority of STIs occur;2 the population is 50.4% male and 99.4% Muslim.5 Considering the religious and cultural contexts, as well as the taboo surrounding sexuality, in Iran, sexual health education—particularly for young people—has not been effective;6 the knowledge, attitude and practice of people regarding sexual health are relatively weak.7 Economic and social barriers, stigma, poor accessibility to care and treatment services, limited capacity of STI service providers, and lack of laboratory capacity in the diagnosis of STIs are some of the plausible factors that contribute to patients with STI neglecting STI testing and treatment.4 ,7 For syndromic and aetiological management, STI surveillance in Iran consists of routine STI case reporting by all health providers at the primary healthcare level as well as STI prevalence assessment in various subgroups. Although over 80% of Iranians are covered by the primary healthcare system, most patients with STIs, especially men, prefer STI services in the private sector.4
Various sources of information on STI prevalence, health-seeking behaviours, access to diagnosis tests and appropriate treatment contribute to the proper response and rational decision-making of STI control programmes.8 ,9 STI surveillance and STI reporting have not been successful in Iran; thus, the data obtained are unreliable and not valid for correct interpretation.3 ,4 Epidemiological and sociobehavioural studies in the general population and in specific subpopulations are alternative, more useful sources.8 ,9 Most epidemiological data in Iran is obtained from prevalence surveys of accessible subpopulations. For example, the prevalence of Chlamydia trachomatis among men with urethritis in north-east Iran in 2012 was 10.6%.10 The prevalence of Trichomonas vaginalis among women attending health centres in the west of Iran was about 2.1%,11 while in 2011 the prevalence of C. trachomatis, Neisseria gonorrhoeae, herpes simplex type-2 and HIV among female sex workers in the south-central region of Iran, was 9%, 1.4%, 9.7% and 4.7%, respectively.12 However, the results of these studies cannot be generalised to the entire population of Iranian adults. In addition, there are several technical, economic and social barriers that hinder the carrying out of STI screening programmes and population-based surveys on STI aetiology in Iran. Moreover, many people are unaware of the various types of STIs and the exact pathogens,13 and so are unable to report their STI acquisition accurately.
In light of the above considerations, we conclude that, as an alternative approach, a population-based survey on STI-associated symptoms and health behaviours among Iranian adults is a reasonable solution for reducing the information gap in Iran. A study in 2011 showed that about 85% of women and 36% of men in high-risk groups and the general population of Iran have experienced at least one episode of STI symptoms in their lifetime. (M Nasirian, M Karamouzian, K Kamali, et al. The pattern of care seeking of patients with sexually transmitted infections in Iran. IJHPM 2015; under review). However, that study did not mention specific and sensitive STI-associated symptoms with respect to gender. Hence, in the present study we have estimated the population-based prevalence of sensitive, specific and non-specific STI-associated symptoms among 18–60-year-olds, and inspected care-seeking patterns of those who suffered these symptoms via a gender-specific questionnaire. The information obtained will be used to prepare basic information for future studies and qualified decision-making for the improved management of STIs in Iran.
Materials and methods
In summer 2014, a cross-sectional study, in partnership with the Ministry of Health and Medical Education and the United Nations Population Fund (was performed with the aim of estimating the prevalence of STI-associated symptoms in the (18–60-year-old) Iranian population and assessing care-seeking patterns among those people who have experienced such symptoms.
Study setting
Four cities were selected as representative of the 31 provincial capitals of Iran with respect to geographical distribution: Tehran in the centre, Shiraz in the south-central region, Sari in the north and Kerman in the south-east.
Sample size and sampling
In the absence of valid data, based on 6.3% prevalence of curable STIs in the world,14 and the opinions of Iranian experts, a total of 9166 participants were recruited proportionate to size (city population, gender, age group) from the 18–60-year-old general population through a multistage sampling method, in a period of 1 week. First, with respect to capital of province as cluster, Kerman, Tehran, Sari and Shiraz were chosen using cluster sampling. In the second phase, municipal areas of each city were considered as strata, and then participants were selected from various crowded public places and streets at various times of the day (morning, noon and evening) using quota sampling, taking into account gender and age groups proportionate to size. This was gleaned from previous research, which showed that due to cultural and religious sensitivities in Iran, people were more likely to disclose sensitive information such as that relating to STIs or sexual activity in street-based surveys, rather than household surveys.15
Eligibility criteria
Due to the occurrence of STIs in the more sexually active age groups, 18–60-year-old women and men, who were Iranian citizens and had lived in the aforementioned areas for at least 5 years, were recruited to the study. To analyse data (ie, survey analysis) and estimate rates, we wanted to use the estimated 18–60-years-old population size from the latest national census results;5 therefore, we tried to account for national census regulations for the residency time frame. One of the criteria in the national census project was being resident for at least 5 years in a specific geographical area. Adolescents (15–17-year-olds) were excluded as they were under the legal age for participation and there existed the impracticality of acquiring informed consent from their parents. Cultural sensitivities in Iran are such that questioning participants as to whether they are sexually active, as per the eligibility criterion at the beginning of the interview, was not feasible. Therefore, all participants eligible by age, gender and citizenship were included and interviewed, and only at the end of the interview were participants asked about their current relationship status through indirect questions (ie, married, temporary marriage or have a fiancée or a boy/girl friend whether they were unmarried). Participants were assumed sexually active according to their responses to those questions regardless of their marital status.
Data collection
To collect data, two gender-specific questionnaires were designed including current experience of certain specific and non-specific STI-associated symptoms (women: 12 symptoms and men: 11 symptoms) (figure 1), reactions to symptoms, seeking, and referral to aetiological testing, as well as sexual activity and demographic information. Content validity of questionnaires was evaluated by a number of clinicians and STI experts. Then, both questionnaires were standardised through a pilot study. The Kuder Richardson reliability of questions on STI-associated symptoms was around 0.57; in addition, the covariance matrix showed no statistically significant correlation between most questions (p>0.05).
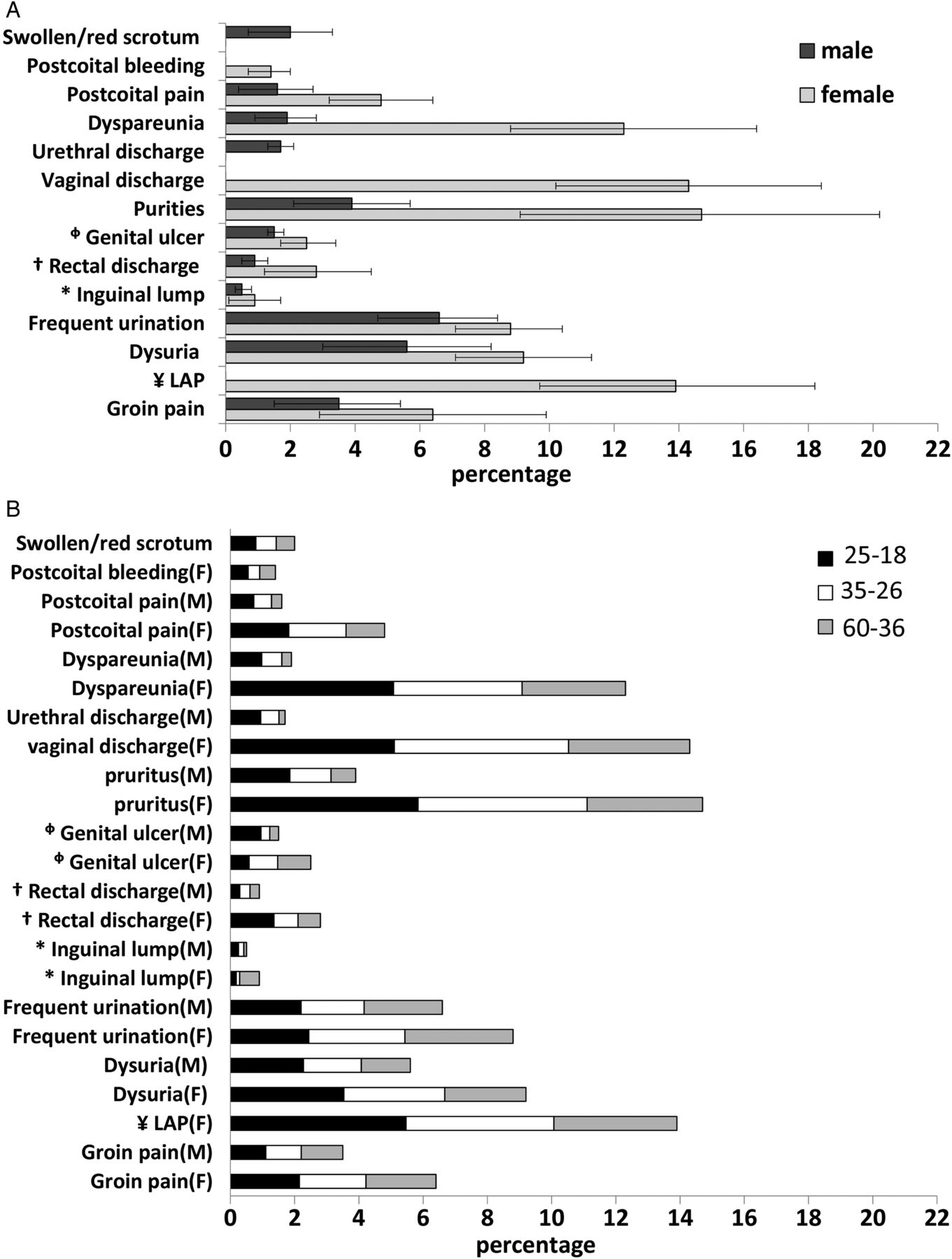
Prevalence of each sexually transmitted infection (STI)-associated symptom at the time of interview based on gender (A) and age group (B). *Swollen, red or colourless, palpable, †Bloody or non-bloody, ΦPainful or painless, bullous or non-bullous, ¥Lower abdominal pain.
To diminish respondents’ misconceptions of STI-associated symptoms, especially among the illiterate or those with a low level of literacy, and based on previous investigation, interviewing was carried out, rather than relying on a self-administered method. Experienced male and female interviewers, familiar with the local culture in each city, were selected and then trained using a role-playing method. The interviewers explained the survey objectives, interviewing method, independency response, anonymity, confidentiality of information, and provided an educational pamphlet on STI prevention and treatment as an incentive for participation after selection of potential participants. Following receipt of verbal informed consent, participants were interviewed.
Data analysis
After checking responses for errors, data were coded and entered into Stata software (V.11) via double data entry method and then cleaned. Participants who were not ‘assumed sexually active’ in the year of study were excluded from analysis. The missing data rate was lower than 1% in the whole data bank; however, missing data in age were imputed (ie, simple mean imputation).16 The weight of samples in each city was reviewed using survey analysis. Frequency, proportion and percentage were used for descriptive analysis. In order to examine the crude and adjusted effects of predictors on outcome variables, generalised estimating equation analysis was applied, taking into account response clusters for each participant, with 95% confidence coefficients. As a consequence of dissimilarity in STI-associated symptom prevalence and the magnitude in different ages, three age groups were decided upon for analysis: 18–25 years, 26–35 years and 36–60 years.
Ethical consideration
The questionnaires were anonymous. Participation in the survey and answering of each question was optional. Due to certain cultural issues, and in order to increase response rate and decrease improper answers, verbal informed consent was applied.17
Results
Participants’ demographics
A total of 9166 participants (50.3% female) 18–60 years old were enrolled. The proportion of subjects in each age group, 18–25 years, 26–35 years and 36–60 years, was in accordance with the general population. Due to the lack of availability of detailed information, comparison between the demographic characteristics of participants and the general population was not possible. Approximately 67.3% of respondents (66.2% of women and 68.3% of men) were ‘assumed sexually active’ in the year of study and eligible to be included in the analysis. The mean age of eligible participants was 35.4 (95% CI 34.2 to 36.6) years: age 34.4 (95% CI 33.9 to 34.7) for women and 36.4 (95% CI 35.4 to 37.5) for men (table 1).
Demographic characteristics of eligible participants by city and gender
Experience of STI-associated symptoms
In general, 39.9% (95% CI 28.4% to 51.4%) of women and 17.6% (95% CI 13.9% to 21.6%) of men reported having at least one STI-associated symptom under consideration (figure 1) at the time of study.
Prevalence of the most specific STI-associated symptoms such as genital ulcers in women and men and male urethral discharge were 2.5% (95% CI 1.7% to 3.4%), 1.5% (95% CI 1.3% to 1.8%) and 1.7% (95% CI 1.3% to 2.1%), respectively. Frequency of each symptom fluctuated by age group and gender (figure 1). Overall, the odds of symptoms occurring decreased with an increase in age in both genders (p<0.05). In contrast to the lack of a statistically significant association between formal marriage history and reported symptoms (p>0.05), men with no formal marriage history reported significantly more symptoms compared with those without history, with respect to education and age (p≤0.0001) (table 2).
Demographic factors associated with reporting for those (1) experiencing sexually transmitted infection (STI)-associated symptoms and (2) seeking care for STI-associated symptoms, among the ‘assumed sexually active’ general population in Iran, by gender
Seeking care and influencing factors
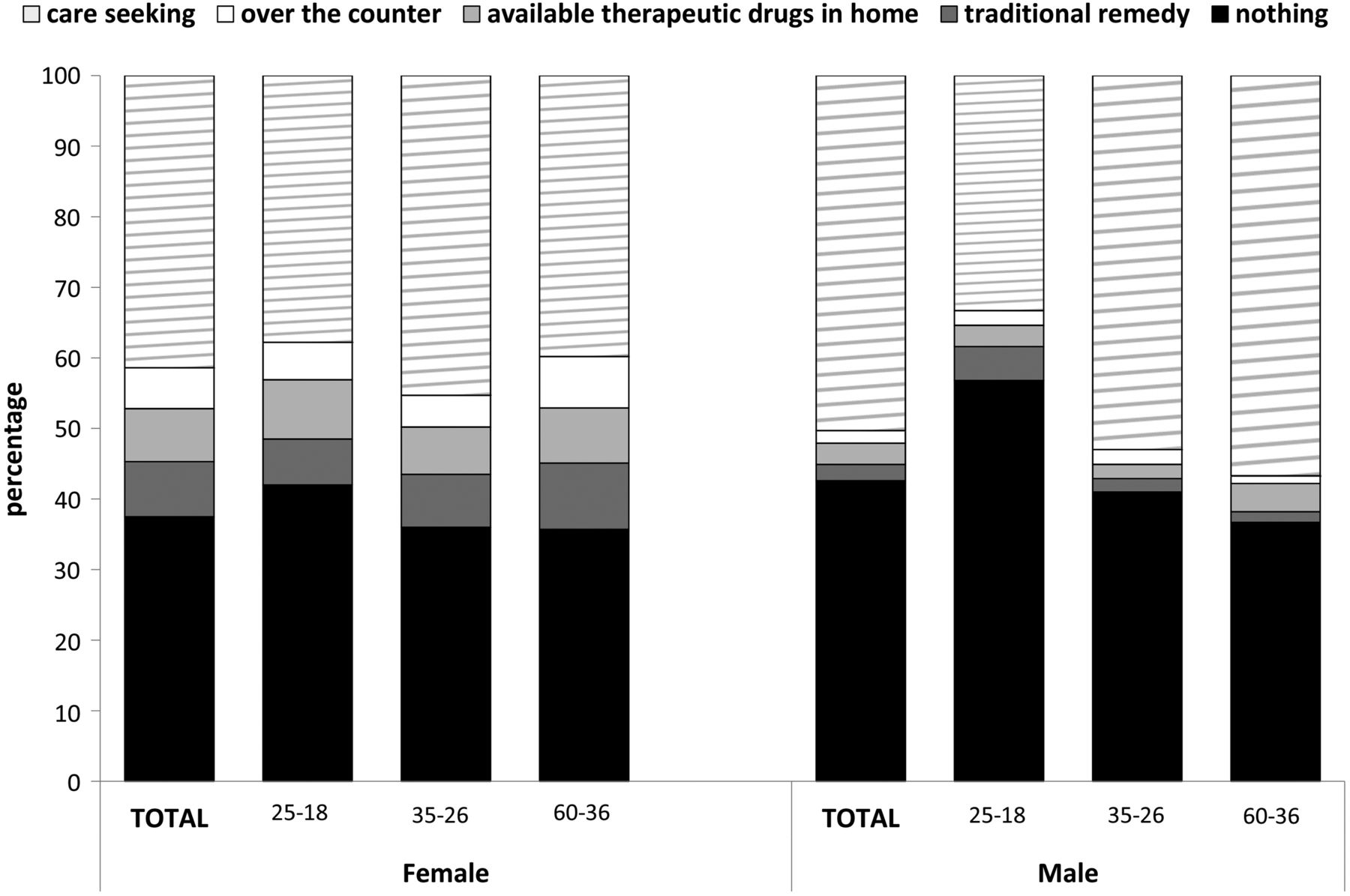
Around 37.4% (95% CI 32.8% to 42.1%) of women and 42.6% (95% CI 36.1% to 42.9%) of men took no action after symptoms first appeared. Moreover, about 21.2% (95% CI 13.3% to 29.1%) of women and 7.1% (95% CI 4.5% to 7.8%) of men treated symptoms themselves by means of traditional remedies, pharmaceutical drugs on hand at home or over-the-counter drugs. About 41.3% (95% CI 28.9% to 53.6%) of women and 50.2% (95% CI 42.5% to 57.9%) of men sought treatment for symptoms (figure 2). Reactions varied according to severity of symptoms; however, we were not able to ascertain symptom-based reactions from data available in the current study.
{kind=link}
{kind=link}
Reaction of those who experienced sexually transmitted infection (STI)-associated symptoms at the time of study by gender and age group.
In contrast to women, care-seeking in men increased with age (p≤0.0001). Although illiterate men sought treatment significantly more often than graduates, the opposite occurred in women (p≤0.0001) (table 2).
Most women looking for care visited gynaecologists and midwives as their first choice and second choice of healthcare professionals. In addition, the large number of men who required care preferred to be treated by a general practitioner or urologist, in comparison to other healthcare professionals (see online web appendix table 3). About 48.9% (95% CI 44.3% to 55.4%) of women and 62.4% (95% CI 48.4% to 76.5%) of men who visited healthcare professionals were referred to the laboratory for aetiological diagnosis tests. The percentage of patients referred to the laboratory differed significantly dependent on the type of healthcare provider (pwomen=0.021, pmen=0.003); dermatologists and urologists tended to refer the most.
Discussion
Results showed that more than a third of adult women and a sixth of adult men in Iran had at least one STI-associated symptom at the time of study; symptoms, which were similar between both genders, were generally more frequently reported in women. This may be due to the low sensitivity and/or low specificity of some STI-associated symptoms.18 Furthermore, women tend to be more interested in their health, to pay more attention to symptoms, and subsequently to report them more often.19 ,20 An Iranian study in 2011 showed that 13.7% of women and 4.9% of men reported ever having had ulcers, and 8.3% and 40%, respectively, reported discharge, in their lifetime. (M Nasirian, et al, 2015; under review).
Since STIs are spread by sexual activity and because this is such a stigmatised topic, household sampling was not feasible; the study was, therefore, limited to street-based convenience sampling, which may not be representative of the general population. In addition, because of the sensitive nature of the questions, the Iranian cultural context and the interview location, the occurrence of response bias was probable. While excluding sexual activity as an inclusion criterion diminished the rejection rate, we ended up excluding around a third of the participants due to their ‘assumed sexual inactivity’ in the final analysis; an unfortunate loss of money and time. Self-reported data and resilient misconceptions of symptoms despite interviewers’ descriptions are the other limitations. Also, a significant proportion of STIs are asymptomatic and many reported symptoms are neither sensitive nor specific as a proxy for STIs. We therefore cannot estimate STI prevalence and disease burden in this study. Aetiological surveys on the general population and/or indirect estimation methods are recommended for the estimation of STI prevalence.
The prevalence of self-reported symptoms varied between age groups; STI symptoms tended to occur more often in younger sexually active age groups. It appears that sexual activity patterns in Iran have changed over generations; risky sexual behaviour, such as extramarital sex, has increased in the younger generation.6 ,21 It was not feasible to ask participants about their sexual behaviours and partners (eg, number of partners, whether partners had other partners) as possible factors for STI transmission in the current study. For future studies, an analysis of the reasons for greater number of reported symptoms in the younger generation is suggested.
Half of women and men took no action after the onset of symptoms. At the time of interview, symptoms may have only just developed and the interviewees who report having taken no action yet, may in fact be about to seek care. As such, we cannot conclude that they did not ever seek care for symptoms. However, a fifth of women and a tenth of men treated symptoms themselves; less than half of the participants sought treatment. An Iranian study in 2011 showed 31.6% of those who had STI symptoms in the previous year did nothing to improve their symptoms, 8.0% tried self-treatment and 60.9% sought treatment. (M Nasirian, et al, 2015; under review). Regarding our study, younger Iranians did not seek care for STI symptoms as often as older participants did. Perhaps this is because older people already had health problems other than STIs that forced them to visit healthcare providers. In due course, some of the stated STI-associated symptoms would be alleviated by medicines prescribed for other diseases. A study in Pakistan demonstrated a significant relationship between genital ulcers and ageing with seeking care.22 Our results showed that the self-treatment rate in women was more than twice that of men. A study in Morocco showed that women were more likely to use traditional remedies, because they are more affordable than therapeutic drugs from the pharmacy.23
Although self-medication is common worldwide and especially in developing countries,24 ,25 behaviours of failing to seek care lead to some health difficulties. Untreated STIs can be transmitted, as well as facilitate HIV transmission.8 Drug resistance, such as antibiotic resistance in Neisseria gonorrhoea, is one of the main implications of self-treatment with inappropriate regimens and/or incorrect doses.26 Stigma and the ability to purchase over-the-counter drugs seem to be the main reasons for self-treatment in Iran.4 As we could not explore further those people who attempt to treat symptoms themselves or decide to do nothing, an investigation into the causes of these behaviours is essential. In addition, since delay in seeking care is an important aspect of care-seeking behaviour, as well as increasing the odds of STI transmission,27 ,28 an investigation on how long people wait before seeking care and the causes of these delay behaviours is proposed.
The majority of women who sought care visited gynaecologists and midwives as their first choice and second choice of healthcare professionals; men tended to visit general practitioners or urologists after their symptoms appeared. A study in 2011 in Iran showed similar results. (M Nasirian, et al, 2015; under review) Being informed of the population's preferences in choosing a health provider can contribute to localisation of patients with STI and allow us to provide more care services and concentrate more studies there. Moreover, sentinel sites for STI surveillance in Iran can be set up in these locations (CDC 2015). Our data did not inquire into affecting factors, such as types of symptoms, education, age, cultural background and available facilities, when choosing a healthcare provider.
Over half of the men and women who visited healthcare providers were referred to a laboratory for the diagnosis of the aetiology of symptoms; urologists and dermatologists tended to refer patients for aetiological tests more often. In another study in Iran, 44% of those seeking care reported being referred for STI testing by health providers. (M Nasirian, et al, 2015; under review). Because this is a cross-sectional study using a non-randomised sample, we cannot produce predictive models to assess symptom type and referral to laboratory.
The results of our study contribute indirectly to achieving an overview of the STI situation in Iran. Providing policy makers with information regarding the distribution of STI-associated symptoms and care-seeking patterns in different groups assists them in planning care and treatment services and targeted education. With the knowledge of the population's preferences regarding health providers, they can allocate STI services in suitable settings.
Conclusion
The frequency of STI-associated symptoms in the general population in Iran is considerable. The results emphasise the need for appropriate and timely STI care, including diagnosis and treatment, and the need for more attention to health promotion to mitigate onward and future infections. Paying due attention to the care-seeking pattern is fundamental for policy making and planning with respect to STIs, and this, unfortunately, has been neglected.
Key massages
More than a third of women and a sixth of men reported experiencing at least one STI-associated symptom at the time of interview.
A fifth of women and a tenth of men declared treating symptoms themselves, while less than half sought care and treatment.
Most women visited a gynaecologist and midwife; men tended to visit a general practitioner and urologist after their symptoms appeared.
Acknowledgments
The authors thank all those whose assistance proved to be a milestone in the accomplishment of their end goal; the Ministry of Health and Medical Education and the United Nations Population Fund supported them generously.
References
Supplementary materials
Abstract in Persian
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in Persian - Online abstract
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table
Footnotes
Handling editor Jackie A Cassell
Collaborators Abbas Sedaghat; Zahra Rajab Poor; Zahra Gholami Poor; Zahra Hasan Poor; Mozhgan Sabet; sorour Fouladi; Fatemeh Navaeian.
Contributors MN designed the study, analysed and interpreted the data, and drafted the manuscript. MRB supervised the analysis and revised the manuscript critically. KK contributed to the conception and design of the work substantially, and revised the manuscript. AAH supervised all parts of the work and approved the final version of manuscript.
Funding This work was supported by the Ministry of Health and Medical Education (grant number 1/54177).
Competing interests KK is supported by CDC and the Ministry of Health. The remaining authors declare that they have no conflicts of interest.
Ethics approval The research ethics committee of Kerman University of Medical Sciences, KMUECR, approved the study protocol via the ethical code ‘IR.KMU.ECR.1394.171’.
Provenance and peer review Not commissioned; externally peer reviewed.