Article Text

Abstract
Background Apart from penile–anal intercourse, other anal sexual practices (rimming, fingering and saliva use as a lubricant for anal sex) are common among men who have sex with men (MSM). The aim of this study is to evaluate whether these anal sexual practices are risk factors for rectal gonorrhoea in MSM.
Method A cross-sectional survey was conducted among MSM attending Melbourne Sexual Health Centre between 31 July 2014 and 30 June 2015. Rectal gonorrhoea cases were identified by culture.
Results Among 1312 MSM, 4.3% (n=56) had rectal gonorrhoea. Other anal sexual practices were common among MSM: receptive rimming (70.5%), receptive fingering or penis dipping (84.3%) and using partner's saliva as a lubricant for anal sex (68.5%). Saliva as a lubricant (adjusted OR 2.17; 95% CI 1.00 to 4.71) was significantly associated with rectal gonorrhoea after adjusting for potential confounding factors. Receptive rimming and fingering or penis dipping were not statistically associated with rectal gonorrhoea. The crude population-attributable fraction of rectal gonorrhoea associated with use of partner's saliva as a lubricant for anal sex was 48.9% (7.9% to 71.7%).
Conclusions Saliva use as a lubricant for anal sex is a common sexual practice in MSM, and it may play an important role in gonorrhoea transmission. Almost half of rectal gonorrhoea cases may be eliminated if MSM stopped using partner's saliva for anal sex.
- NEISSERIA GONORRHOEA
- GAY MEN
- SEXUAL BEHAVIOUR
- PUBLIC HEALTH
- PREVENTION
Statistics from Altmetric.com
Introduction
Gonorrhoea has been rapidly increasing in men who have sex with men (MSM) in Australia and worldwide.1–3 Understanding the transmission of gonorrhoea in MSM is the key to its successful control. It has been widely assumed that rectal gonorrhoea is transmitted by unprotected receptive anal intercourse (RAI).4 ,5 However, a recent mathematical model has shown that gonorrhoea would not be eliminated by consistent condom use during penile–anal sex as transmission can occur between other anatomical sites.6 This is consistent with a recent empirical study showing gonorrhoea positivity in MSM is increasing after adjusting for condom use during anal sex.7 These studies suggest that sexual practices other than penile–anal sex, such as digital–anal (‘fingering’) and oral–anal (‘rimming’) sex, may play a key role in gonorrhoea transmission in MSM.8
Gonorrhoea transmission is still occurring in the setting of condom use for penile–anal sex. If, however, the penis is not solely involved in the acquisition of rectal gonorrhoea, a plausible alternative mechanism is required. There have been three studies showing gonorrhoea can be detected in human saliva by culture,9–11 suggesting that saliva may play a central role in gonorrhoea transmission among MSM. Saliva use as a lubricant for anal sex is a common practice among MSM (87%)12; however, very little is known about the role of saliva in the transmission of sexually transmitted infections (STIs). The aims of this study were to (1) quantify the proportion of MSM engaged in other anal sexual practices (rimming, fingering and use of partner's saliva as a lubricant for anal sex) and (2) identify the risk factors associated with rectal gonorrhoea in MSM.
Methods
Population and sampling
This cross-sectional study was conducted at Melbourne Sexual Health Centre (MSHC) in Victoria, Australia, between 31 July 2014 and 30 June 2015. MSHC is a free and public walk-in sexual health service located in the city of Melbourne. It provides approximately 40 000 consultations annually and about 37% of these were for MSM.13 All new patients attending MSHC for the first time and those who were not seen at MSHC for >3 months were required to complete a computer-assisted self-interview (CASI) that collected their demographic details and sexual behaviours history.
MSM were defined as men who self-reported having any sexual contact with other men. All MSM who were required to complete CASI were invited to answer six additional questions on the computer after completing CASI. All MSM attending for STI testing will be offered testing according to the Australian guidelines,14 which include pharyngeal and rectal swabs for gonorrhoea. Urethral swabs for gonorrhoea were only taken in symptomatic patients. All swabs were plated onto GC Agar medium for culture.
Measurement
This questionnaire was designed to examine three different types of anal sexual practices other than penile–anal intercourse: (1) receptive rimming (participant's partner rimmed the participant's anus); (2) receptive fingering or penis dipping (participant's partner inserted their finger or dipped their penis into the participant's anus) and (3) whether the participant's partner used their saliva as a lubricant when they inserted their fingers or penis into the participant's anus. In addition, demographic characteristics (ie, age), number of male partners, condom use for RAI, HIV serostatus and laboratory diagnosis of gonorrhoea were collected as part of the routine care at MSHC. All behavioural data were from the three months prior to the study. RAI was categorised as ‘no RAI or always used condom’ or ‘not always condom use’ in the last three months.
Statistical analysis
MSM who were tested for rectal gonorrhoea on the day were included in the analysis. Urethral gonorrhoea is usually symptomatic among MSM,15 and men with urethral symptoms would tend to access to healthcare and receive treatment promptly.7 Hence, we excluded MSM who tested positive for urethral gonorrhoea as a proxy for recently acquired infection.16
Descriptive statistics and frequency distribution of the study variables were computed. Gonorrhoea positivity was calculated as the number of positive cultures divided by the number of tests, and the 95% CI was calculated based on the ‘exact’ binomial distribution.17 χ2 test was used to examine the association between other anal sexual practices, age group and condom use for RAI. Univariate and multivariate analyses were conducted to investigate whether anal sexual practices were associated with rectal gonorrhoea. Age, condom use for RAI, pharyngeal gonorrhoea diagnosis and HIV serostatus were included in the multivariate model as potential confounding factors. The crude and adjusted population-attributable fraction (PAF) of rectal gonorrhoea associated with anal sexual practices was calculated for those practices found to be significantly associated with rectal gonorrhoea. All analyses were performed using Stata V.13.1 (Stata, College Station, Texas, USA).
Results
Socio-demographic characteristics
A total of 6406 MSM attended MSHC and completed CASI. All were automatically invited to participate in the study; however, 3807 (59%) MSM declined to participate (figure 1). Of the 2599 (41%) MSM who completed the questionnaire, 1287 (49%) MSM were excluded because 1054 did not have an rectal swab for gonorrhoea and 163 were duplicates (ie, an individual who completed the questionnaire more than once during the study period, and only the first response was included). In addition, we also excluded 50 MSM who tested positive for urethral gonorrhoea and 20 with incomplete responses. Of the 1312 MSM who were eligible and included in the data analysis, 56 (4.3%; 95% CI 3.2% to 5.5%) tested positive for rectal gonorrhoea. A total of 1273 MSM also tested for pharyngeal gonorrhoea and 22 (1.7%; 95% CI 1.1% to 2.6%) tested positive. The age of MSM ranged from 17 to 78 years, with a median age of 29 (IQR 25–37). Thirty-three (2.5%) MSM were HIV positive. The median number of male sex partners in the last three months was 3 (IQR 2–5).
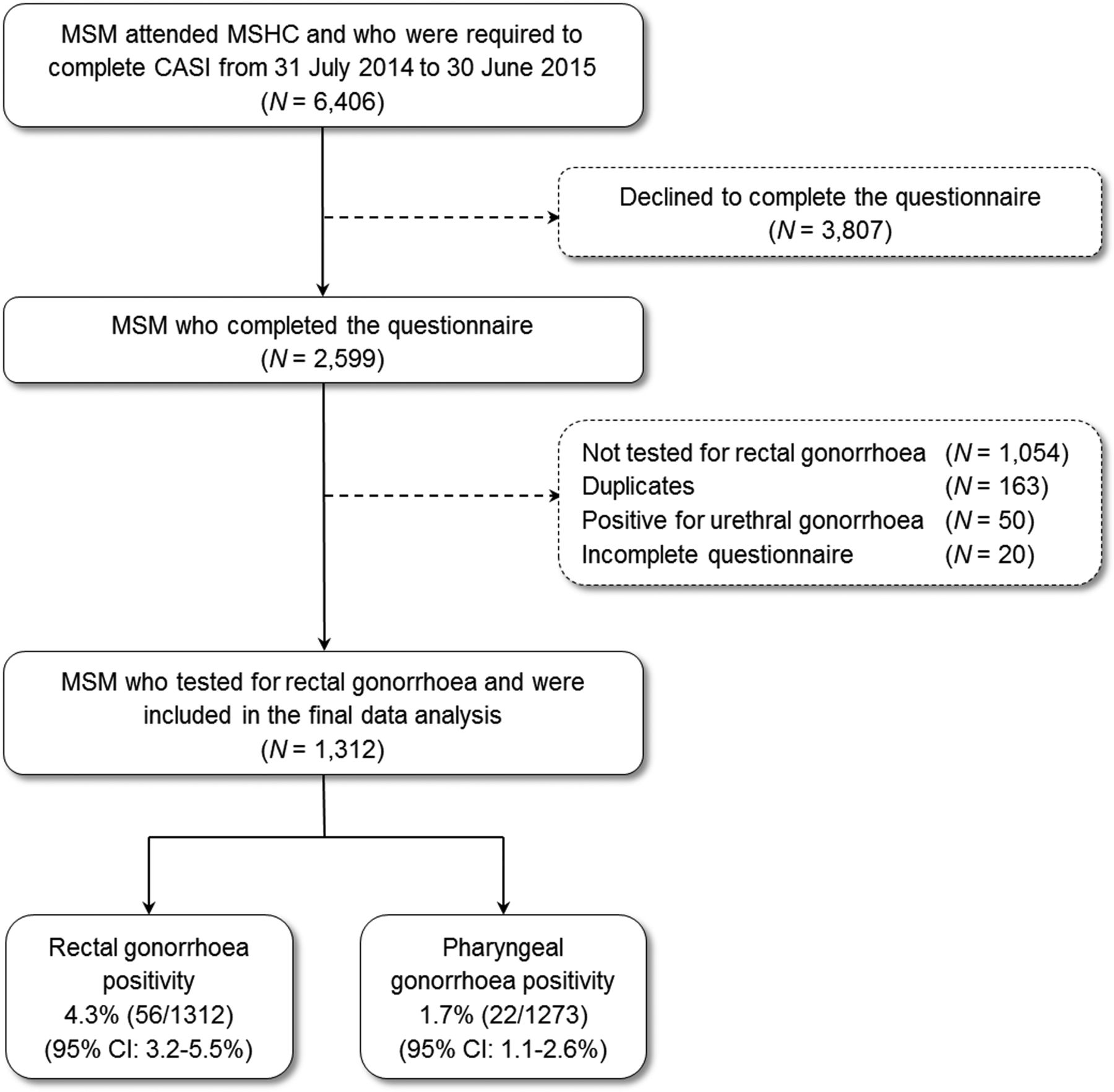
Flow diagram of sample selection for the analysis. CASI, computer-assisted self-interview; MSHC, Melbourne Sexual Health Centre; MSM, men who have sex with men.
Anal sexual practices other than penile–anal intercourse
Of the 1312 MSM, 925 (70.5%) reported receptive rimming, 1106 (84.3%) reported receptive fingering or penis dipping, and 899 (68.5%) reported use of partner's saliva as a lubricant for anal sex in the last three months. The median number of rimming partners in the last three months was 1 (IQR 0–3), and fingering/penis dipping partners was 2 (IQR 1–4). Receptive rimming and receptive fingering or penis dipping did not differ by age group (figure 2). However, MSM aged 25–34 (72.2%) were more likely to use partner's saliva as a lubricant for anal sex compared with the younger (≤24 years) and older (≥35 years) age groups (p=0.026) (figure 2). MSM who reported not always condom use for RAI were more likely to have receptive rimming (78.0% vs 64.5%), receptive fingering or penis dipping as partial anal penetration (92.3% vs 78.6%) and using a partner's saliva as a lubricant (79.2% vs 59.7%) compared with those who used condoms always or reported no RAI in the last three months (p<0.001). No significant association was observed between anal sexual practices and HIV serostatus (p>0.05).

{kind=link}
{kind=link}
Proportion of men who have sex with men (MSM) who engaged in (A) receptive rimming, (B) receptive fingering or penis dipping and (C) using partner's saliva as a lubricant for anal sex, by age groups and condom use for receptive anal intercourse (RAI).
Risk factors for rectal gonorrhoea
In the univariate analysis, rectal gonorrhoea was significantly associated with using partner's saliva as a lubricant for anal sex (OR 2.48; 95% CI 1.20 to 5.10), but not associated with receptive rimming or receptive fingering/penis dipping (table 1). One man with rectal gonorrhoea reported no male sexual partners in the last three months, and he was also HIV positive. In addition, rectal gonorrhoea was strongly associated with pharyngeal gonorrhoea in both univariate and multivariate analyses (aOR 17.31; 95% CI 6.29 to 47.63).
Risk factors for rectal gonorrhoea among men who have sex with men
The adjusted odds of having rectal gonorrhoea were 2.17 (1.00–4.71) times higher among those who used partner's saliva as a lubricant for anal sex compared with those who did not use their partner's saliva for anal sex, after adjusting for age, condom use for RAI, pharyngeal gonorrhoea positivity and HIV serostatus. Receptive rimming or fingering/penis dipping was not associated with rectal gonorrhoea.
The crude PAF of rectal gonorrhoea associated with using partner's saliva for anal sex was 48.9% (95% CI 7.9% to 71.7%), and the adjusted PAF of rectal gonorrhoea associated with using partner's saliva for anal sex was 41.4% (95% CI −4.1% to 67.0%) after adjusting for age, condom use for RAI, pharyngeal gonorrhoea positivity and HIV serostatus.
Discussion
This is the first study to show that using partner's saliva as a lubricant for anal sexual practices may be a substantial risk factor for rectal gonorrhoea, potentially contributing to about 40% of rectal infections. Our findings, which suggest that saliva may be the key to understanding some rectal infections, also provide a plausible explanation for previous studies showing that receptive anal sexual practices such as fingering or rimming are associated with rectal gonorrhoea. The observational studies are complex because many of the anal sexual practices occur with the same act and sexual partner and it is possible that saliva, operating as a potential medium for transmission, could explain the contradictory observations from different studies. The public health implication for a preventive message for STI is likely to be complex and challenging given that saliva is commonly used as part of sexual activity among MSM. Further larger studies with the power to separate out the independent contribution of different anal sexual activities will help clarify the risks.
Our study does have several limitations. First, sampling bias may have occurred. The response rate in this study is low (∼41%), and if the sexual practices and rectal gonorrhoea infection were different between those who participated and those who did not, it may have influenced our results. Second, this study was conducted at a single urban sexual health clinic, and our findings would need to be replicated at other centres. Hence, our findings may not be generalisable to all community-based MSM because individuals attending our centre may be at higher STI risk than those in the community. Third, all sexual behavioural data were self-reported as in other studies and hence response and recall bias may have occurred. Fourth, we used culture for gonorrhoea testing that is likely to have underestimated the true prevalence of rectal gonorrhoea. In comparison with nucleic acid amplification tests (NAATs), culture has poor sensitivity (53%) for detecting gonorrhoea in the rectum.18 Fifth, the wide CI of PAF (7 % to 72%) and adjusted OR (1.0–4.7) of using partner's saliva use as a lubricant mean our data must be interpreted cautiously. Larger studies are required to verify the association and specific sexual practices involving saliva use for anal sex and rectal gonorrhoea. Sixth, we only adjusted for condom use, HIV serostatus, age and pharyngeal gonorrhoea in the final multivariate model but not for other sexual practices.
Apart from penile–anal intercourse, other anal sexual practices such as receptive rimming (71%), fingering/penile dipping (84%) and use of partner's saliva as a lubricant (69%) are very common among MSM in Australia, and our findings are consistent with previous studies. A large community-based survey in Australia in 2009 has shown that 71% received rimming from their partners in the last six months. The high frequency of rimming and the finding that MSM reported that receptive rimming was associated with the greatest sexual excitement among all anal sexual practices other than penile–anal intercourse highlight the potential difficulty with behaviour change in this area. For example, in that same study, only 11% of MSM were not excited by receptive rimming.19 Other anal receptive practices are also common with a recent study among MSM in Australia showing that 66% had insertive or receptive fingering.20 Saliva use as a lubricant for anal sex is common in Australia, consistent with findings from the USA,12 and Vietnam.21
The ‘Health in Men’ (HIM) study among HIV-negative MSM in Sydney has shown that receptive fingering and receptive rimming are associated with rectal gonorrhoea,8 and there was a positive but non-significant association in this study. Our study and the HIM study had a number of differences that might explain why the findings were different. First, different testing methods were used (ie, NAAT in HIM vs culture in our study). This suggests either false positive cases were included in the HIM study or true positive cases were missed in our study. Second, different study design and outcome measures were used. The HIM study was a cohort study and used hazard ratio as an outcome measure, while this was a cross-sectional study, and ORs were calculated. Third, the measurement of risk factor was different. The HIM study measured the sexual behaviours in the last six months, while we limited to last three months to minimise the recall bias. The average duration of infection for rectal gonorrhoea may be about 12 months.22 Hence, the risk factors might be underestimated if they had an infection for >3 months and did not receive rimming in the last three months. Fourth, the volume of saliva use may also need to be considered. It is suggested that saliva use as a lubricant involves a larger volume of saliva in comparison with the exposure of saliva through rimming; and hence rimming may not have adequate saliva for gonorrhoea transmission. The strong association with pharyngeal gonorrhoea in the adjusted analysis highlights how important the pharynx is in the overall transmission and how important further studies of exploring more complex sexual behaviours and their role in rectal gonorrhoea are.
The association between lubricant use and rectal STIs is not well known. There has been one study conducted by Gorbach and colleagues23 in the USA showing that use of lubricant (either saliva or commercial lubricant) is associated with the combined rectal STI outcome of chlamydia, gonorrhoea or syphilis but not with gonorrhoea alone. Understanding how the use of lubricant can plausibly be associated with rectal gonorrhoea is important given the commercial lubricant is not contaminated before opening. Several studies have shown that gonorrhoea can be detected in saliva,9–11 and this provided a plausible mechanism for how gonorrhoea can be transmitted if saliva is used as a lubricant for anal sex.
There has been one mathematical model of gonorrhoea transmission that includes sexual activities other than penile/anal sex, and this model (2015) supports our findings.6 The model estimates that the prevalence of rectal gonorrhoea is higher among MSM with rimming (4.6%) compared with 4.1% in those who do not. However, the model assumed only 23% of MSM had rimming (vs 71% in this study), which is an estimate obtained from a small sample (N=200) of MSM visiting sex-on-premises venues (SOPVs).24 Sexual behaviours may be different within and outside SOPV. Therefore, the community-based prevalence of gonorrhoea among MSM with rimming would have been underestimated. Furthermore, we estimated that nearly half of rectal gonorrhoea cases would be eliminated if men did not use partner's saliva as a lubricant for RAI although this is a somewhat simplistic interpretation.
It is likely that the public health message from our findings is complicated and involves more than simply recommending that saliva is not used as a lubricant for anal sex. Among men with pharyngeal gonorrhoea, saliva is often present, so the implication is that if transmission from the pharynx to the anus is to be avoided, then anal activities that involve pushing saliva into the anal canal or contaminating the external anus should be avoided. This would mean avoiding rimming, saliva on fingers or saliva as a lubricant for anal sex. To better understand this area, it may be that interventional studies, mathematical models and complex event-level observational studies will require defining how the use of saliva contributes to gonorrhoea transmission in MSM. Furthermore, molecular epidemiology on gonorrhoea genotyping between partnerships may be useful to assess the causal transmission pathways in MSM populations.
Key messages
Other anal sexual practices (rimming, fingering/penis dipping and using partner's saliva as a lubricant for anal sex) are common among men who have sex with men (MSM) in Australia.
Saliva as a lubricant for anal sex may be a potential risk factor for rectal gonorrhoea.
Almost half of rectal gonorrhoea cases may be eliminated if MSM stopped using partner's saliva for anal sex.
References
Footnotes
Handling editor Jackie A Cassell
Contributors CKF conceived the idea that saliva may play a key role in the transmission of gonorrhoea in MSM. EPFC, DL, SW and CKF designed the study. EPFC, DL and CKF were involved in designing the questionnaire. EPFC undertook the statistical analyses. JSH, TRHR and CKF assisted with data interpretation. EPFC prepared the first draft of the manuscript. All authors contributed to the interpretation of the study findings and contributed to the drafting of the manuscript.
Funding This work was supported by the National Health and Medical Research Council (NHMRC) programme grant (number 568971).
Competing interests EPFC is supported by the Early Career Fellowships from the Australian NHMRC (number 1091226).
Ethics approval Ethical approval was obtained from the Ethics Committee of Alfred Hospital, Melbourne, Australia (number 324/14).
Provenance and peer review Not commissioned; externally peer reviewed.