Article Text

Abstract
Background Testing for gonorrhoea with nucleic acid amplification tests (NAATs) is not recommended in low-prevalence populations as it results in high numbers of false positive results. The aim of this study was to examine temporal trends of gonorrhoea positivity by NAAT and culture in heterosexual men in Victoria, Australia following recent increases in gonorrhoea notifications.
Methods Three data sources between 2007 and 2014 were used in this study: notification data from the Victorian Department of Health, Medicare testing numbers of single chlamydia and dual NAATs performed, and electronic records on heterosexual men attending Melbourne Sexual Health Centre (MSHC).
Results Notifications of gonorrhoea by NAAT (with/without culture) in heterosexual men in Victoria rose threefold from 74 in 2007 to 238 in 2014, while the number of dual NAATs ordered over the same period underwent a fivefold increase from 14 061 to 71 860. The overall proportion of NAATs that were positive for gonorrhoea in Victoria was low and fell from 0.53% in 2007 to 0.33% in 2014 (Ptrend=0.002). Of the 28014 new heterosexual men attending MSHC, the gonorrhoea positivity by culture was 0.9%, and chlamydia positivity by NAAT was 8.5%. The positivity of both infections did not change over time.
Conclusions These data suggest that gonorrhoea prevalence in heterosexual men is low and stable, despite annual increases in notifications. Guidelines in most countries recommend restricting testing to groups or populations with prevalence over 1%, symptomatic individuals or those at increased epidemiological risk. These data indicate gonorrhoea testing should not automatically accompany chlamydia screening in low-risk heterosexual men.
- GONORRHOEA
- CHLAMYDIA TRACHOMATIS
- EPIDEMIOLOGY (GENERAL)
- MEN
Statistics from Altmetric.com
Introduction
It is recommended in the Australian guidelines that heterosexuals screen for chlamydia but not for gonorrhoea.1 Since 2007 dual nucleic acid amplification tests (NAATs) that test for both gonorrhoea and chlamydia have become widely available. A recent Australian study reported a 3.5-fold increase in the notifications of gonorrhoea by NAATs in women since 2007 in Victoria as dual NAATs use increased.2 However, gonorrhoea positivity by culture remained stable among women attending a large sexual health service in Victoria.2 The increase in notifications either reflected a true increase in prevalence, more widespread testing or an increase in false positive results from increased use of NAATs in populations with very low prevalence of gonorrhoea (0.2%–0.3%).2 If there was a true increase in gonorrhoea in women, it would be expected that a similar trend would be observed in urethral gonorrhoea in heterosexual men who are mostly symptomatic.
The aim of this study was to describe the proportion of gonorrhoea notifications identified by NAATs in Victoria and the proportion of gonorrhoea and chlamydia cases among all new heterosexual men attending a sexual health centre during 2007–2014.
Methods
Three electronic data sources between 2007 and 2014 were used in this study (see online supplementary table S1): (1) gonorrhoea and chlamydia positivity among heterosexual men attending Melbourne Sexual Health Centre (MSHC); (2) notifications of gonorrhoea diagnoses in Victoria from the Victorian Department of Health (DoH) and (3) number of tests ordered in Victoria from the Medicare Benefits Schedule (MBS). MBS item 69316 represents chlamydia testing alone, and MBS items 69317/69319 represent dual NAATs for chlamydia and a second or third organism, which typically represents the dual chlamydia and gonorrhoea NAATs.3
We used the Medicare testing data as the denominator for gonorrhoea tests undertaken in Victoria, and the number of notifications by NAAT with or without culture from the DoH as the numerator to calculate the ‘dual NAATs positivity’.
All heterosexual men attending MSHC between 2007 and 2014 for their first consultation were included in the analysis. Heterosexual men who reported only sex with women during the last 12 months. This group predominantly represents a population with a very low prevalence of gonorrhoea (<1%) in Australia. Men who have sex with men (MSM), transgender individuals and those self-reported as a sex worker were excluded.
Gonorrhoea microscopy and culture were undertaken in men with urethral discharge and those reporting being a contact of gonorrhoea. Gonorrhoea screening was not undertaken among men without urethral symptoms at MSHC in accordance with Australian guidelines.1 All heterosexual men attending MSHC for the first time are offered chlamydia screening. Gonorrhoea specimens were plated onto Thayer–Martin medium by clinicians during the consultation and promptly delivered to the on-site laboratory. Urethral swab, or first pass urine samples are collected for chlamydia detection. Chlamydia specimens were analysed on-site using BD ProbeTec ET strand displacement NAAT (Becton, Dickinson and Company, Sparks, Maryland, USA). MSHC only used culture for the detection of gonorrhoea, and there was no change in testing guidelines during the study period.
In order to examine the trend of gonorrhoea positivity among heterosexual men, gonorrhoea positivity was calculated by dividing the number of culture positive cases by the number of first consultations. Urethral chlamydia positivity was calculated by dividing the number of NAAT positive cases by the number of individuals tested for chlamydia. Descriptive statistics and frequency distributions for year of consultation, gonorrhoea and chlamydia positivity were calculated. A χ2 trend test was used to assess trend of gonorrhoea and chlamydia positivity over the study period.
All statistical analyses were performed using SPSS software (V.21.0, SPSS, Chicago, Illinois, USA). Ethical approval was obtained from the Ethics Committee of Alfred Hospital, Melbourne, Australia (number 507/14).
Results
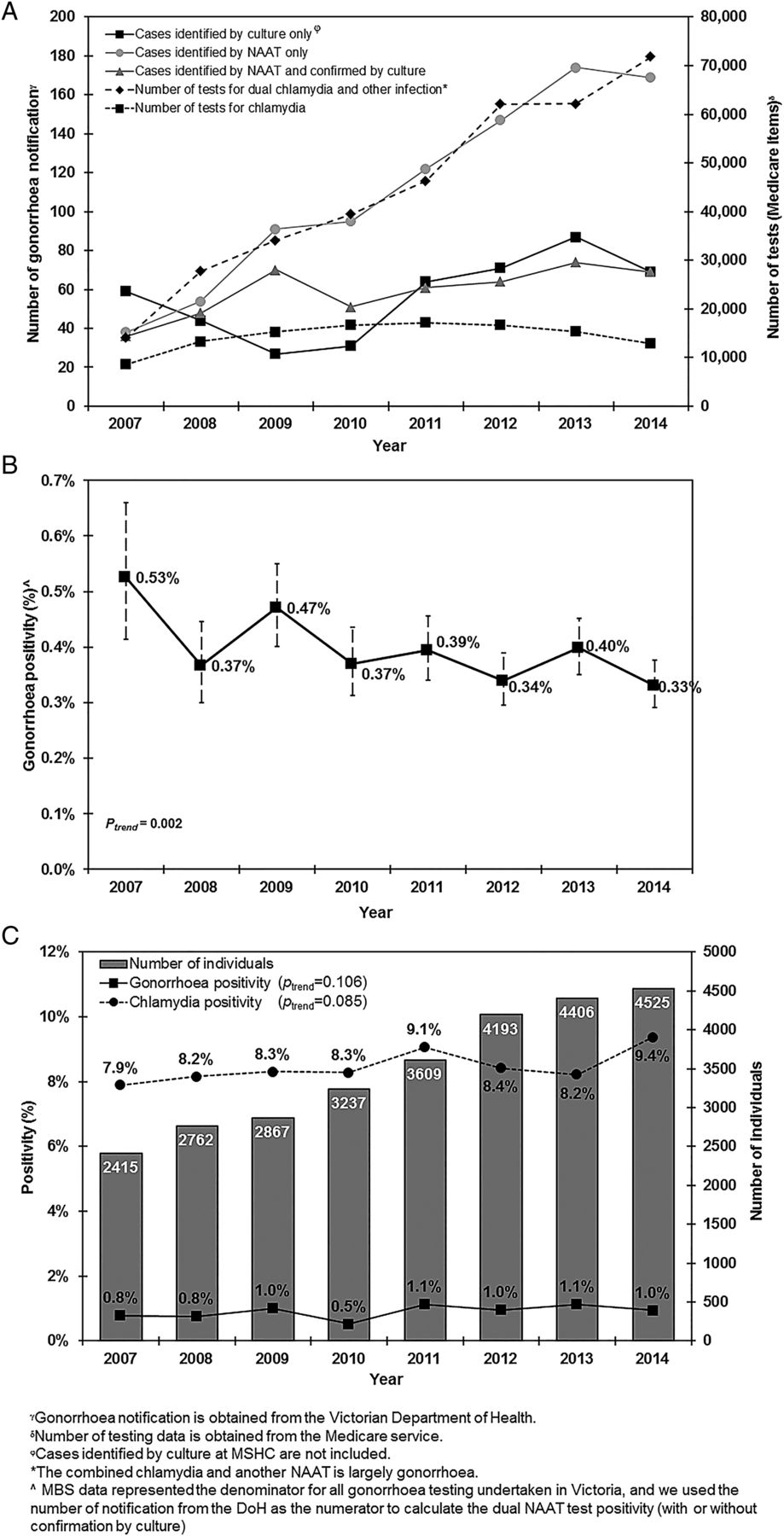
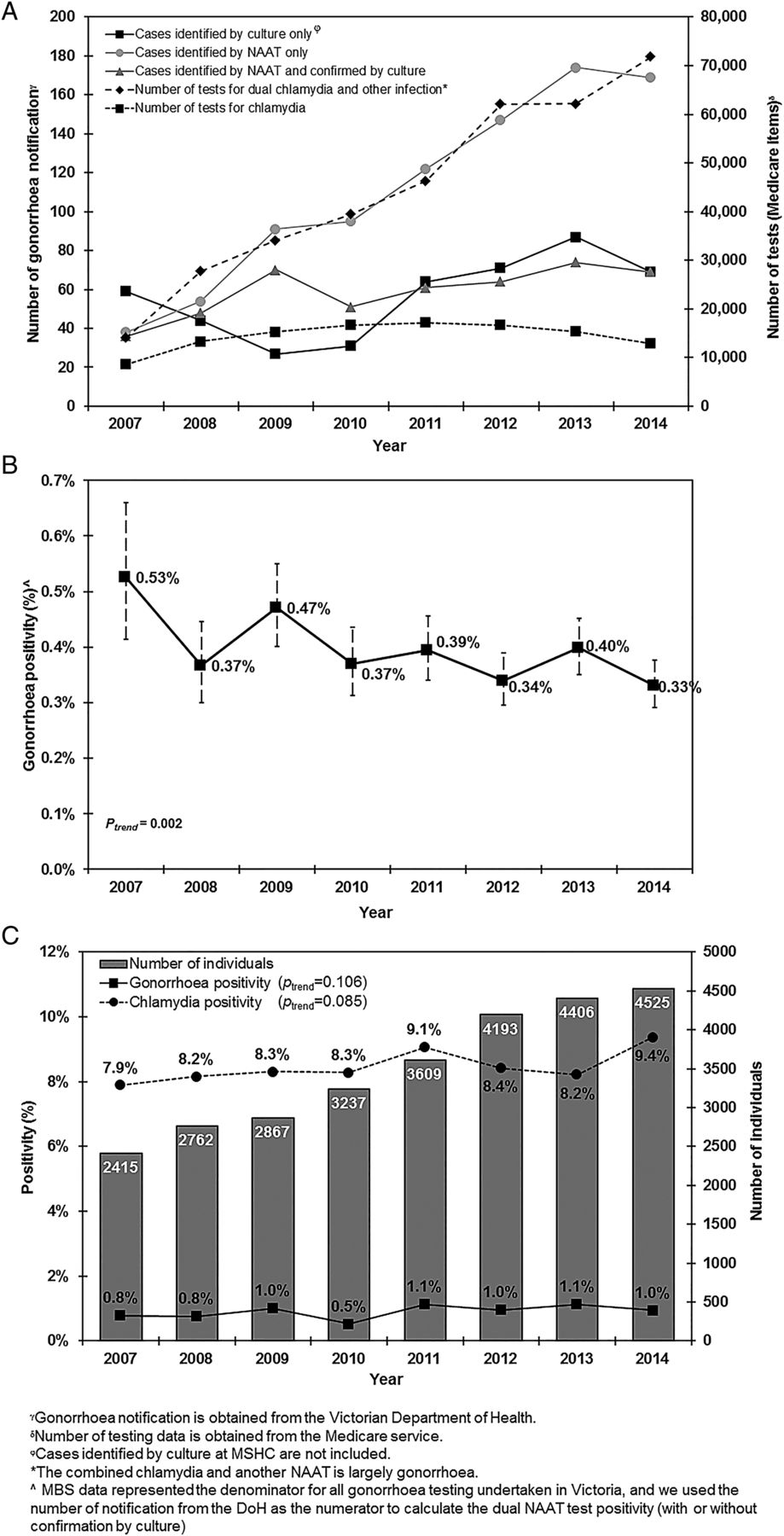
There was a fivefold increase in the number of dual NAATs (MBS items 69317/69319) from 14 061 in 2007 to 71 860 in 2014. The number of chlamydia only NAAT (MBS item 69316) increased only modestly from 8574 to 12 915 (figure 1A).
{kind=link}
(A) Gonorrhoea notifications in heterosexual men, and number of chlamydia testing only (MBS 69316) and dual NAATs (MBS 69317, 69319) in all men in Victoria, Australia, 2007–2014; (B) proportion of gonorrhoea notification identified by NAAT in Victoria, Australia, 2007–2014; (C) gonorrhoea and chlamydia positivity among heterosexual men attending MSHC, 2007–2014. DoH, Department of Health; MBS, Medicare Benefits Schedule; MSHC, Melbourne Sexual Health Centre; NAAT, nucleic acid amplification test.
A total of 12 975 gonorrhoea cases in men were notified to the Victorian DoH between 2007 and 2014, 42% (N=5438) reported having sex with men, only 15% (N=1958) reported previous sexual contact with women and the remaining 43% (N=5579) of men had sex with people of unknown gender. Of the 1958 cases in heterosexual men, 7% (N=143) had no testing method reported, 23% (N=452) were identified by culture only, 45% (N=890) were identified by NAAT only and 24% (N=473) were detected by NAAT and confirmed by culture. Overall, there was a 2.5-fold increase in gonorrhoea notifications in men who reported having sex with a female partner from 141 in 2007 to 349 in 2014. However, there was a fourfold increase in gonorrhoea diagnoses identified by NAAT only, from 38 to 169, but only a 1.5-fold increase in gonorrhoea diagnoses by culture with or without NAAT from 95 to 138 (figure 1A). Importantly, cases identified by culture only remained stable over the study period (from 59 in 2007 to 69 in 2014). The dual NAATs positivity fell from 0.53% (95% CI 0.41% to 0.66%) in 2007 to 0.33% (95% CI 0.29% to 0.38%) in 2014 (Ptrend=0.002) (figure 1B).
A total of 28 014 heterosexual men attended MSHC for the first consultation between 2007 and 2014 with a median age of 28 years (IQR: 24–35). The overall gonorrhoea positivity identified by culture was 0.92% (260/28014), and chlamydia positivity was 8.5% (2047/23987) in heterosexual men at MSHC between 2007 and 2014 (see online supplementary table S2). No significance temporal trend in positivity was observed for either infection (figure 1C).
Discussion
Between 2007 and 2014 there was a 2.5-fold increase in notifications of gonorrhoea in heterosexual men that occurred in the context of a fivefold rise in the use of dual NAATs in a population with very low prevalence of gonorrhoea (<1%). Furthermore, gonorrhoea positivity identified by culture only remained low (<1%) and stable among heterosexual men attending a large sexual health service in Melbourne over the study period. These findings are consistent with previous studies demonstrating similar effects in women in Australia4 and Britain,5 and indicate that detection for gonorrhoea by NAATs is being used in very low-risk populations when various international guidelines (ie, Australian, US and UK) and the manufacturing guidelines recommend against screening populations with low prevalence of gonorrhoea due to the high likelihood of false positive results.6 ,7 Our findings support current recommendations that gonorrhoea screening should not be done among asymptomatic heterosexual men unless they report specific behavioural risks such as being a contact of infection.
The reason for the rise in notifications is important. If a rise in gonorrhoea notifications was due to an increase in undiagnosed gonorrhoea because of the increased use of dual NAATs, one would not expect the substantial fall in the proportion of gonorrhoea cases detected by NAAT that we observed in our study. The rise in notifications may be due to false positive results from screening a very low-prevalence population of gonorrhoea.6 ,7 We estimate that about 60% of positives would be false positives using the highest specificity (99.7%) from the Cobas package insert, and a prevalence of gonorrhoea of 0.2%. Using confirmatory NAAT on these samples would reduce false positive results but there remain difficulties with the interpretation of discrepant results. Care pathways should include algorithms for managing various testing scenarios from the outset.
There are several limitations in this study. First, the gonorrhoea positivity by culture is based on a single sexual health centre and it may not be representative of the entire community in Victoria. Second, the Medicare testing data used in this study only include Commonwealth funding for laboratory services testing for gonorrhoea and chlamydia. Tests conducted through public hospitals, while small, are not included within these data and we therefore may have overestimated the positivity. Third, the Medicare data do not collect or report data on behavioural characteristics of patients or the anatomical site of the specimen, and therefore may include some specimens from MSM. While MSM represents only about 2% of the adult male population they are tested more frequently and at more sites than heterosexuals.8 The effect of this bias would be underestimation of the positivity because notifications in MSM are excluded from the numerator but testing is not excluded from the denominator.
The third National Survey of Sexual Attitudes and Lifestyles (Natsal-3) in 2010–2012 showed that the weighted gonorrhoea prevalence decreased from 0.4% to <0.1% following confirmatory testing of positive screening results among men in the UK.6 Furthermore, a survey from the English National Chlamydia Screening Programme reported that over half (53%) of the practitioners used dual tests on samples for chlamydia testing in the community setting in the UK.5 Donovan et al9 reported the number of Australian laboratories routinely performing dual chlamydia/gonorrhoea NAATs increased from 9 (32%) in 2007 to 23 (82%) in 2012.
In conclusion, the use of dual NAATs in the context of a population with low prevalence of gonorrhoea is likely to result in false positive results. Gonorrhoea screening using NAAT should be restricted to high-risk populations such as commercial sex workers and MSM.
Acknowledgments
The authors would like to acknowledge A Afrizal for his assistance with data extraction.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Handling editor Jackie A Cassell
Contributors CKF and EPFC conceived and designed the study. PKM performed data analysis and wrote the first draft of the manuscript. CKF, GF and EPFC assisted in statistical analysis. CKF, SNT and EPFC involved in data interpretation. EPFC provided overall supervision of the study. CKF, SNT, WST, MYC, CSB and EPFC revised the manuscript for intellectual content. All authors read and approved the final version of the manuscript.
Funding This work was supported by the National Health and Medical Research Council (NHMRC) (Number 568971). EPFC is supported by the Early Career Fellowships from the Australian NHMRC (Number 1091226).
Competing interests None declared.
Ethics approval Ethics approval for this study was obtained by Alfred Health Ethics Committee (Number 507/14).
Provenance and peer review Not commissioned; externally peer reviewed.